
Abstract
Background
An evidence-based eHealth education tool was developed for patients with knee osteoarthritis (KOA). This study aimed to evaluate the long-term effectiveness on patient knowledge level and analyzed the patient's satisfaction with the proposed tool.
Methods
A two-arm randomized controlled trial was performed, with 218 KOA patients allocated 1:1 to two groups by balanced block randomization. Both groups received usual care and additionally, the eHealth group used the proposed eHealth tool during the process. The primary outcome measure was the validated osteoarthritis patient knowledge questionnaire (PKQ-OA). The secondary outcome was patients’ satisfaction with the eHealth tool. Measurements were taken at baseline, post-intervention (T1), 1-month (T2), 3-month (T3), and 6-month (T4) follow-up. Statistical analyses, including ANOVA and chi-square tests, were employed to compare outcomes between the groups.
Results
The results of the PKQ-OA indicated that patients in the eHealth group (38.7% ± 25%, 95% confidence interval (CI), 33.9%–43.4%) performed significantly better than the usual care group (28.8% ± 21.1%, 95% CI, 24.9%–32.9%) in terms of correct responses to the knowledge assessment in T1(P = 0.001). In addition, a higher percentage of patients in the eHealth group (39.4%) achieved a score of at least 50% on the knowledge assessment compared to the usual care group (14.6%). Patients who received eHealth education perceived it as a valuable tool for education. The analysis of follow-up data showed that the knowledge level of the eHealth group was higher than that of the control group at 6 months (F = 0.727, P = 0.471), but there was no significant difference.
Conclusion
Patients educated using an evidence-based eHealth education tool showed significant improvements in knowledge and were more likely to achieve an adequately informed status. The evidence-based eHealth tool could offer a low-cost, effective educational device.
Introduction
Knee osteoarthritis (KOA) is one of the most frequent chronic joint diseases in the world, with an age-associated increase in both incidence and prevalence.1,2 Globally, KOA prevalence increased by 48% from 1990 to 2019. 3 In China, the 10-year average age-standardized prevalence and incidence of KOA was 4.6% and 25.2 per 1000 person-years, respectively. 4 In addition, the southwest region of China had the highest years lived with disability rate from KOA. 5 KOA has led to substantial economic burdens on patients, their families, and society, primarily due to its high incidence and disability rates. 6 The available treatment options of KOA encompass a spectrum of approaches, including non-pharmacological interventions like self-management, lifestyle modification, and physical modalities, as well as more invasive measures such as intra-articular injections and joint replacement surgery.7–11 However, it is important to acknowledge that patients may encounter various benefits and risks when receiving these treatments. Studies indicated that the key to a successful long-term outcome of KOA is optimal patient selection and preoperative counseling.12–14
Patient education is integral to the treatment and care of patients with KOA. Tailored patient education has proven effective in equipping patients with the knowledge and skills necessary for self-management. 15 By providing comprehensive information about KOA, healthcare providers can better engage patients in positive behavior changes, ultimately leading to improved health outcomes. However, studies have reported dissatisfaction with the details provided by healthcare providers for KOA. 16 This dissatisfaction often stems from vague information, limited consultation time, and imprecise explanations of the disease's progression, which together hinder patients’ understanding of KOA and reduce adherence to self-management practices.17,18 Evidence-based patient education entails a systematic approach that integrates the most up-to-date medical best evidence, which could assist patients in comprehending the progression of a disease, as well as the available management alternatives and protective strategies, thereby facilitating self-care. 19 A clinical trial revealed that educating patients with KOA using an evidence-based clinical practice guideline poster resulted in substantial improvements in their knowledge levels. 20 In addition, studies suggested that integrating patient education with clinical practice guidelines and decision-making support could potentially reduce the variability in healthcare delivery.21,22 Therefore, the development and application of such education tools have huge value in enhancing patient understanding and adherence to current practice guidelines.
Electronic health (eHealth), defined as “the delivery of user-centered healthcare services through information and communication technologies, mainly Internet,” is an alternative medium for the delivery of patient education. 23 According to evidence, self-management and exercise programs for patients with KOA by eHealth approaches significantly improved pain, physical function, and quality of life compared to usual care.24,25 In addition, a systematic review demonstrated that eHealth tools might be as effective as usual care, and possibly more cost-effective, which is a crucial implication for many overly burdened healthcare systems. 26 The beneficial impact of eHealth in enhancing self-management and treatment adherence among patients with diverse medical conditions has been extensively recorded.27–29 Furthermore, compared to traditional face-to-face education methods, eHealth tools offer greater accessibility, scalability, and real-time updates, which are particularly beneficial for managing KOA. 30 However, some participants were observed to use the eHealth intervention in unintended ways, diminishing its overall effectiveness. 31 Additionally, the effectiveness of the eHealth tool may vary by region, raising uncertainty about whether eHealth education is superior to other educational methods. To address these challenges, it is essential to develop an eHealth intervention tool that incorporates advanced feedback mechanisms, such as regular reminders and proactive strategies. Furthermore, there has been no randomized controlled trial evaluating the educational effectiveness and patient satisfaction with evidence-based eHealth tools for KOA patients in southwest China.
Based on the existing research questions, we developed an eHealth education tool for patients with KOA that integrates guidelines from the Chinese Medical Association 32 and Osteoarthritis Research Society International. 33 The primary goal of the study is to assess the influence of the evidence-based eHealth education tool on patient knowledge in comparison to usual care. We hypothesize that the eHealth education tool can lead to a statistically significant improvement in patient knowledge and satisfaction compared to the usual care group. The secondary objective is to initially investigate the tool's long-term educational impact on KOA patients, with the expectation of sustained knowledge retention and improvement over time.
Methods
Study design
In this two-arm prospective randomized controlled trial, patients with KOA received health education through an eHealth patient education tool or usual care. This study was approved by the Ethics Committee on Biomedical Research, West China Hospital of Sichuan University, and prospectively registered on the Chinese Clinical Trials Registry (ChiCTR2100051083). This trial was reported according to the Consolidated Standards of Reporting Trials statement. 34 In addition, the protocol of this study was published. 35 There were no changes to the methods after the commencement of the trial.
Participants
KOA patients in this study were consecutively recruited through referrals to the outpatient physiatry/physiotherapy clinic at West China Hospital of Sichuan University, situated in Southwest China, from January 1, 2022, to June 16, 2023, after providing informed consent. These referrals were facilitated by various communities and regional hospitals spanning Mianzhu county (Sichuan), Longquan district (Chengdu, Sichuan), Mianyang city (Sichuan), and Ya’an city (Sichuan). The recruitment process received support from Jilin University and Heilongjiang University of Chinese Medicine. Specifically, this study was conducted as a multi-center trial focused on clinical settings in the southwestern region of China, an area known for the high prevalence of KOA. The inclusion criteria were the following: (a) aged between 45 and 80 years, (b) had KOA (Kellgren–Lawrence grade 2 or greater) with symptoms lasting for at least 3 months, (c) with adequate hearing and eyesight, (d) have an Internet-enabled device and access to the Internet, and (e) fluent in oral expression. Patients were excluded if they presented one of the following: (a) were unable to read or write in Chinese, (b) had hearing and vision impairment, (c) had fibromyalgia or a systematic arthritic condition, (d) had knee replacement surgery, and (e) had a history of clinic visits or an appointment with any physician/therapist/healthcare professional for evaluation of KOA. These exclusions were made to focus on the effects of the intervention on KOA patients alone and to improve the internal validity of the study.
Sample size
We utilized the PASS software (NCSS Statistical Software) to calculate the required sample size. The calculation of the sample size was conducted by taking into account the difference between groups in the primary outcome, assuming that participants in the eHealth group would exhibit a correct response rate of 55.3%, while those in the usual care group would have a rate of 39.5%. 20 To ensure sufficient statistical power, a power of 95% and a significance level of 5% (two-sided test) were employed, with a value of 0.5 standard deviations used to determine the sample size. By applying these parameters, a Z-score of 1.96 was obtained. Considering a dropout rate of 20%, a sample size of 108 per group (total of 216 participants) is required.
Randomization, allocation, and blinding
Eligible participants were randomly assigned to either the eHealth or usual care group in a 1:1 allocation ratio by balanced block randomization at the time of obtaining consent. The allocation concealment process was blinded and conducted in the order of recruitment using a computer-generated random allocation schedule operated by a senior statistician at the Centre for Biostatistics, Design, Measurement and Evaluation (CBDME) of West China Hospital, Sichuan University. The patients, research coordinators, and the eHealth physiotherapists received notification regarding the randomly assigned group of each participant through a sealed opaque envelope. However, the participants were aware of their group allocation (eHealth or usual care), as they actively participated in the intervention. The researchers who conducted the data collection and analysis were blinded to group assignment, minimizing potential bias in data interpretation. While the eHealth physiotherapists who delivered the intervention were not blinded, standardized protocols and training were implemented to ensure consistent delivery of the intervention.
Interventions
The intervention was specifically described in the protocol. 35 In brief, we developed an eHealth education tool based on an iterative approach to collaborative persuasive design between healthcare providers and patients.35,36 The eHealth education tool was developed based on an iterative, collaborative persuasive design process involving healthcare providers and patients. Participants assigned to the eHealth group received an invitation QR code to access the eHealth patient education tool (Figure 1(A)). The tool includes the following modules: (a) Education Center: this module includes clinical guideline-based KOA health education, rehabilitation advice, and video guidance; (b) Self-Management: self-monitoring of knee arthritis symptoms during studies; (c) Schedule and Plan: set reminders and make calendars for scheduled evaluations; (d) Communication and Help Center: provide an overview of this tool; remote access to designated physiotherapist; and (e) System Backend: researchers can download patient information in this module (Figure 1(B) and (C)). Participants in the eHealth group received education through the utilization of the eHealth education tool, in addition to their usual care. To ensure the educational content is tailored to individual needs, each module of the tool is designed to adapt to the patient's progress and preferences. The intervention was administered within a week following randomization, during which a video consultation with a physiotherapist was conducted, lasting up to 90 min based on the patient's preference. To encourage participants to engage with the information and utilize the tool, automated push notifications will be sent through the WeChat messenger platform twice a week for a minimum of 6 months. Additionally, the Schedule and Plan module allows participants to set personalized reminders and plan their use of the tool based on their individual care needs, ensuring that they are consistently reminded to access the educational content and update their symptom tracking.

Overview of the eHealth education tool. (A) Patients can access the eHealth education tool via invitation QR code. (B) Features of the tool. (C) Backend of the database (physicians).
Patients in the usual care group were subjected to customary care, encompassing a diverse array of care practices available at the outpatient clinic of West China Hospital, without any restrictions imposed by study protocols. This approach, in contrast to standard care, may not accurately represent the care received in real-world settings. 37 To facilitate the completion of follow-up questionnaires and access to the intended KOA care, all control group participants were contacted by an assistant via telephone or WeChat messenger (Tencent Holdings Ltd, Shenzhen, China), who provided them with the necessary instructions.
Outcome measures
Participants completed outcomes at post-intervention (T1), 1-month (T2), 3-month (T3), and 6-month (T4) follow-up after the randomization. The time intervals for measurements were chosen to capture both short-term and long-term effects of the eHealth education intervention. The post-intervention assessment allows for immediate evaluation of knowledge acquisition and user satisfaction. The subsequent follow-ups at 1, 3, and 6 months are intended to assess the retention of knowledge over time, as well as the sustained impact of the intervention on patient behavior and self-management of KOA. All tools and questionnaires used in this study have been obtained with the necessary permissions from the respective copyright holders. In addition, as this study is designed to evaluate the long-term effects of an eHealth intervention, interim analyses and stopping guidelines were not applicable, as the intervention's effects are expected to evolve over time and require a longer duration of assessment.
Primary outcome
The validated osteoarthritis patient knowledge questionnaire (PKQ-OA) 38 was the primary outcome measure, consisting of 7 single-choice and 14 multiple-choice questions, with a total of 31 correct answers. Specifically, the PKQ-OA has shown a high internal consistency (Cronbach's alpha = 0.89) and construct validity when compared to clinical assessments of KOA knowledge. In addition, greater disease knowledge is indicated by higher scores, and achieving a score above 50% on the knowledge section of the questionnaire was categorized as being sufficiently informed. 39
Secondary outcome
The secondary outcome measure was a questionnaire 20 consisting of six closed questions, which can assess patient satisfaction with the consultation, the eHealth patient education tool, and their trust in the physiotherapist.
Statistical analysis
Statistical analysis was performed using Stata, version 14.1 (StataCorp). Data were confirmed to have a normal distribution using the Shapiro–Wilk test. Two-tailed t-tests (for continuous variables) and the chi-square test (for categorical variables) were used to compare baseline measures between the two groups. Baseline characteristics of the two groups are presented as mean and standard deviation for continuous variables and as number and percentage for categorical variables.
The treatment effect was evaluated by analyzing the change in the primary outcome between groups using multivariable regression models. These models were adjusted for potential confounders, including stratification variables such as the use of arthroscopy, use of non-steroidal anti-inflammatory drugs, and the correct rate of the intervention. An interaction between the month of assessment and treatment group was included as fixed effects in the regression model at the T1 assessment.
Subgroup analyses were performed, with pre-specified subgroups based on age, BMI, previous interventions, education level, and income level. The pre-specified subgroups were identified based on clinical relevance prior to the study, whereas additional subgroup analyses based on other factors were considered exploratory and performed post hoc. This distinction between pre-specified and exploratory analyses is made to avoid post hoc interpretations of the data.
Correlations between continuous variables (age, BMI, previous interventions, education level, income level, and patient-reported knowledge scores) were analyzed using Pearson's correlation coefficient (r) for normally distributed data and Spearman's rank correlation (ρ) for non-normally distributed data.
Due to the high dropout rate, the intention-to-treat analysis was not performed. Instead, a per-protocol (PP) analysis was conducted for follow-up data. Two-way repeated-measures ANOVA was used to analyzed the follow-up data over multiple time points. All statistical tests were two-tailed with a significance level of 0.05.
Results
Participant characteristics
Out of the initial 315 patients with KOA assessed for eligibility, we ultimately included 218 patients from September 2021 to August 2022. The trial was completed as planned, with follow-up data collection concluding on August 2023. The flowchart of this study is presented in Figure 2. The baseline demographic characteristics of the participants are detailed in Table 1, and it is worth noting that patient demographics were comparable between the eHealth and usual care groups.
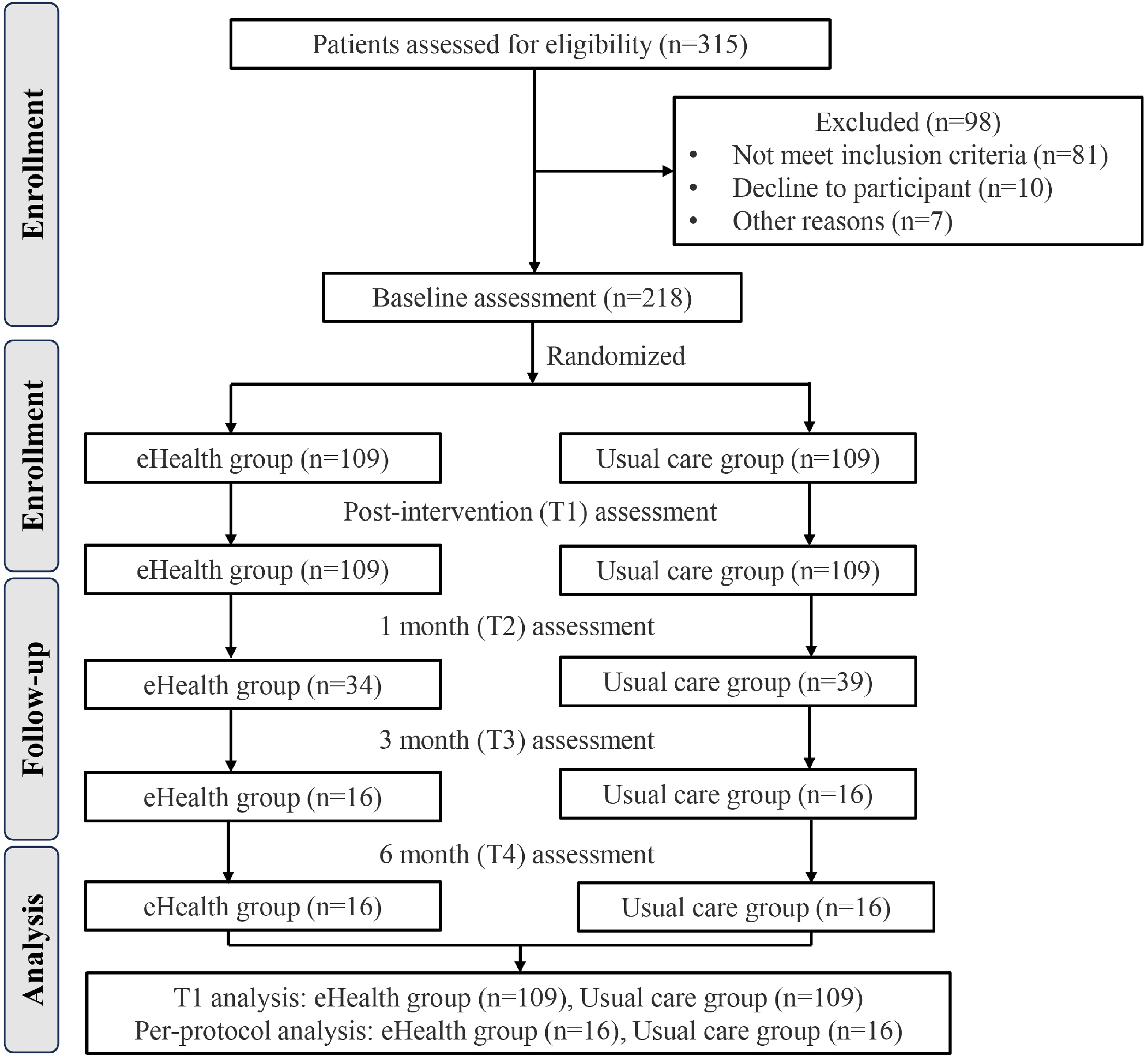
Flowchart for participant selection and assignment.
Baseline demographic and clinical characteristics of the patients.

BMI: body mass index.
The vast majority of patients (over 95%) had undergone various interventions before their initial visit. Among these, physical therapy (n = 163) was the most commonly received, followed closely by traditional Chinese medicine treatment (n = 145). Arthroscopy (n = 12) was the least frequently utilized intervention (Table 1).
Primary outcome
The PKQ-OA results showed that patients in the eHealth group significantly outperformed those in the usual care group in terms of correct responses on the knowledge assessment. The eHealth group had an average score of 38.7% ± 25%, while the control group scored an average of 28.8% ± 21.1% (P = 0.001) (Figure 3 and Table 2). Moreover, a greater proportion of patients in the eHealth group (39.4%) attained a knowledge assessment score of at least 50%, compared to the usual care group (14.6%) (P < 0.001).

Performance on knowledge assessment survey between two groups in T1.
Multivariable regression models for the association between groups, use of arthroscopy, use of non-steroidal anti-inflammatory drugs, and correct rate in T1.

The correlation analyses for T1 are presented in Supplemental Table 1. The findings indicated a positive association between prior interventions and knowledge scores (r = 0.228, P = 0.001). Furthermore, there was a negative correlation between income level and knowledge scores (r = −0.183, P = 0.007).
Secondary outcomes
The results of the satisfaction survey among patients in the eHealth group revealed that a substantial portion of respondents had completed the entire eHealth education program. Most patients in the eHealth group expressed the importance of having treatment guidelines readily available. Furthermore, those who received eHealth education found it to be a valuable visual aid. It enhanced their trust in their healthcare provider's guidance, improved their ability to remember information through their engagement with the eHealth tool, and increased their likelihood of following the treatment recommendations provided by their physician (Table 3).
Satisfaction survey of the eHealth group in T1.

Follow-up data analysis
The high dropout rate may be primarily attributed to the relatively low educational level of the participants, which led to challenges in understanding the study protocols and adhering to follow-up requirements. Additionally, lower participant compliance with treatment and follow-up schedules likely contributed to the dropout rate. Given the elevated dropout rate, this study employed a PP ancillary analysis to examine the follow-up data of both groups. The baseline demographic characteristics of participants in the follow-up data are presented in Supplemental Table 2.
The results of the repeated measures analysis of variance revealed the following: (a) a significant main effect of group (F = 9.767, P = 0.004); (b) a non-significant main effect of follow-up time (F = 0.727, P = 0.471); (c) a significant interaction effect of time and group (F = 9.61, P < 0.001); and (d) in T1, the results of the simple effect test for the group demonstrated a significant effect (F = 33.442, P < 0.001) (Table 4).
Two-way repeated-measures ANOVA of follow-up data.

Multiple comparisons revealed the following: (1) within the eHealth group, the correct rate at T1 was significantly higher than at T2 (P = 0.002), T3 (P = 0.008), and T4 (P = 0.016); (2) in the control group, the knowledge score at T3 was higher than at T1 (P = 0.011), and at T4, it was higher than at T1 (P = 0.014) (Figure 4).

Line chart of knowledge level assessment between the eHealth group and usual care group of follow-up data.
Safety assessment
The proposed eHealth tool used for KOA patient education did not result in any adverse effects. No negative reactions or safety concerns were reported by participants throughout the duration of the study.
Discussion
To the best of our knowledge, this study represents the pioneering research in southwestern China that demonstrates the efficacy of an evidence-based eHealth education tool in augmenting the knowledge levels of patients afflicted with KOA in comparison to those subjected to conventional care. Patients with KOA who received the evidence-based eHealth education tool reported favorable satisfaction with the tool. In addition, the PP analysis of patient follow-up data found that KOA patients who received the eHealth education tool had a higher level of knowledge over a 6-month period than those who received usual care.
Our findings indicate that the eHealth education tool can better improve the patient's knowledge level compared with usual care after one session intervention. The provision of reliable patient education plays a crucial role in facilitating shared decision-making. 40 Carlson et al. illustrated a noteworthy lack of adherence to guidelines within the American Association of Hip and Knee Surgeons when it comes to managing moderate to severe OA, which indicated a potential deficiency in effectively conveying information to patients as well as the utilization of information by healthcare providers. 21 In addition, Meiyappan et al. indicated that a mere 50% of the total expenditure of $2.4 million allocated to KOA patient in their practice was spent on guideline-supported treatments. They advocated for the integration of clinical practice guidelines into patient education as a means to mitigate disparities in treatment approaches, enhance patient outcomes, and ultimately reduce healthcare expenditures. 22 However, there is currently a lack of relevant research on KOA patient education based on clinical guidelines. According to a recently published trial, patients with KOA who received a poster education based on a clinical guideline demonstrated a significantly improved uptake of knowledge compared to those in the usual care group. 20 For readability and quality of digitally delivered education, it may be valuable for digital interventions to curate content from credible websites, treatment guidelines, or co-create educational resources with people with KOA. 41 Therefore, the present study developed an eHealth education tool based on clinical evidence-based guidelines, which can achieve individual education and management of patients with KOA.
The utilization of the evidence-based eHealth education tool has been demonstrated in this study to enhance KOA patients’ comprehension of treatment efficacy. Early management and patient education can mitigate the challenges associated with KOA. 42 To maximize the effectiveness of educational resources, it is crucial for physicians not only to provide these materials but also to promote patient adherence to their proper utilization. To actively support the management of osteoarthritis through noninvasive interventions, healthcare providers must prioritize the importance of conservative approaches. 43 Furthermore, it is crucial for physicians to discern barriers that are specific to individual patients. Previous studies found that lower socioeconomic status, lower education levels, and lower income were related to lower patient performance on knowledge survey scores.44–46 In addition, less treatment experience was also associated with an inferior knowledge level. 47 The results of the present study are consistent with those of the above studies. We found that previous intervention was positively associated with knowledge score. Additionally, there is a negative correlation between income level and knowledge score. Therefore, the above results suggested that targeting patients with these characteristics may require additional support to achieve an informed state.
To assess the feasibility of the eHealth educational tool employed in this study, an online satisfaction survey tool was used to evaluate six dimensions of patient satisfaction. 20 A majority of patients in the eHealth group expressed the importance of readily accessible treatment guidelines. Furthermore, patients who received eHealth education found it to be a valuable visual aid, which enhanced their trust in their healthcare provider's recommendations, improved their ability to remember information due to their engagement with the eHealth tool, and increased their likelihood of adhering to their physician's treatment recommendations. These results indicate that the evidence-based eHealth educational tool utilized in this study offers a positive user experience.
To investigate the long-term educational impact of the eHealth tool on KOA patients, this study conducted follow-up assessments in the first, third, and sixth months to evaluate their knowledge levels. The PP analysis revealed that KOA patients who received the eHealth education tool exhibited higher knowledge levels at the 6-month follow-up compared to those who received usual care, although the difference was not statistically significant. The high dropout rate observed in this study may be correlated with the patients’ educational background and age. Approximately 46.3% of the participants in this study had an education level lower than junior high school, and the average age of the patients was over 60 years old. Additionally, previous research has shown that education level and age significantly influence treatment adherence.48,49 In addition, the high dropout rate may also have reduced the representativeness of the final sample, thereby impacting the external validity of the study. Future research with better retention strategies is necessary to validate these findings and strengthen the conclusions.
The current study has several limitations. First, it focused exclusively on the use of eHealth tools for educating KOA patients in southwestern China, with the study population limited to non-surgical cases. As a result, there is a significant gap in research concerning KOA patients from other regions of China and those who have undergone surgery. Future studies should aim to comprehensively assess the impact and long-term outcomes for KOA patients across different stages, utilizing eHealth tools that integrate education, self-management, and rehabilitation therapy. Furthermore, there is a need to enhance patient adherence to eHealth education tools, which warrants further investigation.
Conclusion
In conclusion, the evidence-based eHealth education tool not only significantly improved patients’ knowledge about KOA in the short term but also provided a positive educational experience that was well-received by patients. While its impact may need to be reinforced over time, the tool offers a feasible, cost-effective method for enhancing patient education and can be considered a valuable addition to conventional care approaches. Further studies are needed to explore long-term strategies for maintaining knowledge retention and to assess the broader impact of such eHealth interventions on patient outcomes and healthcare utilization.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251317230 - Supplemental material for An evidence-based tailored eHealth patient education tool for patients with knee osteoarthritis: A randomized controlled trial
Supplemental material, sj-docx-1-dhj-10.1177_20552076251317230 for An evidence-based tailored eHealth patient education tool for patients with knee osteoarthritis: A randomized controlled trial by Chong Li, Chuanmei Zhu, Kangping Song, Xiaona Xiang, Xiaoyi Wang, Jing Hu, Zhao Li, Yi Deng, Daoxin Jiang, Lixin Guo, Ting Ren, Luwen Zhu, Haibo Ai, Shaojun Zhang, Zhongliang Liu, Yonghong Yang, Siyi Zhu and Chengqi He in DIGITAL HEALTH
Supplemental Material
sj-doc-2-dhj-10.1177_20552076251317230 - Supplemental material for An evidence-based tailored eHealth patient education tool for patients with knee osteoarthritis: A randomized controlled trial
Supplemental material, sj-doc-2-dhj-10.1177_20552076251317230 for An evidence-based tailored eHealth patient education tool for patients with knee osteoarthritis: A randomized controlled trial by Chong Li, Chuanmei Zhu, Kangping Song, Xiaona Xiang, Xiaoyi Wang, Jing Hu, Zhao Li, Yi Deng, Daoxin Jiang, Lixin Guo, Ting Ren, Luwen Zhu, Haibo Ai, Shaojun Zhang, Zhongliang Liu, Yonghong Yang, Siyi Zhu and Chengqi He in DIGITAL HEALTH
Footnotes
Acknowledgements
The authors are grateful to Prof. Deying Kang and colleagues from CBDME of West China Hospital for providing critical comments on study design, sample size calculations, and help in developing a statistical analysis plan.
Contributorship
Study design: SJZ, ZLL, YHY, SYZ, CQH. eHealth tool development: SYZ, CQH. Funding acquisition: SYZ, CQH. Project administration: CL, CMZ, KPS, XNX, XYW, JH, ZL, YD, DXJ, LXG, TR, LWZ. Writing: CL, ZCM. All authors read and approved the final manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by the Ethics Committee on Biomedical Research, West China Hospital of Sichuan University, and prospectively registered on the Chinese Clinical Trials Registry (ChiCTR2100051083).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Natural Science Foundation of China (82272599), Natural Science Foundation of Sichuan Province (2024NSFSC0533), Sichuan University “Research Special Project on the Comprehensive Reform of Innovative Educational Practices Enabled by Artificial Intelligence” (2024-44), 1.3.5 project for disciplines of excellence, West China Hospital, Sichuan University (ZYGD23014), Sichuan University West China School of Medicine Graduate Education Reform Project (HXYJS202415) and Science and Technology Bureau of Deyang City (Deyang Clinical Research Center for Rehabilitation Medicine, Mianzhu People's Hospital, 2023-64). The funders played no role in the design, conduct, or reporting of this study.
Guarantor
Chong Li and Siyi Zhu.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.