
Abstract
Thyroid nodular disease can present in different forms, such as a solitary nodule, multinodular goiter, nodular goiter caused by autoimmune goiter, and nonpalpable thyroid nodules. Among children, thyroid cancer is the most common type of endocrine cancer. Pediatric thyroid cancer is usually detected as a neck mass without any symptoms, leading to variable stages of progression when diagnosed. Papillary thyroid carcinoma is the most common type of thyroid cancer in children with thyroid nodules. We are presenting a case of an 8-year-old male child who was referred to Jimma Medical Center after he developed swelling on the right side of his neck. On examination, multiple, matted 8 × 6 cm, firm to hard, non-tender right lateral neck masses were found, which moved with swallowing. Thyroid function tests were normal. An ultrasound diagnosis of thyroid carcinoma and a cytologic diagnosis of suspicion for papillary thyroid carcinoma (Bethesda V) was made, and an excisional biopsy was advised. A total thyroidectomy was done. A histopathology diagnosis of Papillary thyroid carcinoma (Classic variant) was made. This is an unusual case of Papillary thyroid carcinoma in an Ethiopian child, with plenty of examples previously recorded in the literature but no such report of its occurrence in our setup to our knowledge. When children under 10 have cervical masses, thyroid cancer should be considered. The evaluation of a palpable thyroid mass typically begins with a blood test to check thyroid function, along with ultrasound and fine-needle aspiration biopsy. Currently, fine-needle aspiration biopsy is the most reliable way to diagnose malignancy and determine the appropriate surgical approach. In most cases, treatment will involve a total thyroidectomy. Lymph node dissection is necessary only if lymph node disease is detected during preoperative evaluation.
Introduction
Thyroid nodular disease can manifest in several ways, including a solitary nodule, multinodular goiter, nodular goiter due to autoimmune goiter (Hashimoto thyroiditis or Graves’ disease), and nonpalpable thyroid nodules. 1 Thyroid cancer is the most common type of endocrine cancer among children, although it is rare at a young age, with an incidence of 0.5%–3%.2,3 The incidence of thyroid cancer increases with age, with peak incidence occurring between the ages of 15 and 19. 4 The overall risk of thyroid cancer in childhood thyroid nodules that have undergone surgery is 26.4%. 1 Risk factors for developing thyroid nodules in children include head and neck irradiation, being female, iodine deficiency, and a family or personal history of thyroid disease.5,6
Pediatric thyroid cancer is often discovered as a neck mass without any symptoms, leading to variable stages of progression when diagnosed.7,8 Pediatric thyroid cancer is rare but can be mistaken for other non-thyroid diseases like abscesses, malformations, ectopic thymus, thyroglossal duct cysts, and tumors. 9 Thyroid abnormalities in people under 20 should be thoroughly investigated to rule out cancer, even if diagnostic tests are negative. 10 The initial workup for thyroid assessment includes thyroid function tests, ultrasound (US), and fine-needle aspiration biopsy (FNAB) despite the availability of other tools. 11
Thyroid carcinomas in children are typically well-differentiated and have a malignancy pattern similar to that of adults.12–14 Papillary thyroid carcinoma (PTC) is the most common type of thyroid cancer in children with thyroid nodules, accounting for 5% to 47% of cases.15–17 The classification of differentiated thyroid cancers in children follows the same standard definitions as adults, based on histological criteria set by the World Health Organization. 18 PTC accounts for 90% or more of all childhood thyroid cancers.19–22
Pediatric PTC has four histologic subtypes: classic, solid, follicular, and diffuse sclerosing. 18 Follicular thyroid cancer is rare, while medullary, poorly differentiated, and undifferentiated thyroid carcinomas are even rarer in young patients. 23 It is recommended by the American Thyroid Association that most children undergo total thyroidectomy. This is because studies have shown a higher occurrence of bilateral and multifocal disease. Before undergoing lateral neck dissection surgery, it is important to get cytological confirmation of metastatic disease to lymph nodes in the lateral neck. 23
Case presentation
Clinical findings
We present the case of an 8-year-old male child who was referred to Jimma Medical Center after he presented with a right lateral neck swelling of 1 year to the nearby Gebretsadik Shawo hospital. The swelling started small and grew gradually over 6 months, but then rapidly increased in size. The child has also been experiencing loss of appetite and easy fatigue, but no significant unexplained weight loss was reported. There is no history of irradiation and no family history of thyroid cancer. On arrival at Jimma Medical Center, the child was stable with vital signs of PR = 88 bpm, RR = 24 Br/min, and T = 36.8°C. Upon examination, multiple, matted 8 × 6 cm, firm to hard, non-tender right lateral neck masses that moved with swallowing were detected.
Diagnostic assessments
Thyroid function test (TSH = 1.84 µIU/ml), Complete blood count, Renal function tests (RFT = Creatinine-0.446 mg/dl and Blood urea nitrogen (BUN)-14.35 mg/dl), and Liver function tests (LFT = Aspartate aminotransferase (AST)-25 U/L and Alanine aminotransferase (ALT)-26.76 U/L) were normal. The blood group is O positive and the Rh factor is also positive. A US scan of the abdomen did not show any significant abnormality. However, a neck US showed that the thyroid gland was enlarged in size and echogenicity, with an Isthmus measuring 14 mm and a right lobe 10 × 6 cm hyperinsular mass containing calcification and cystic components, but no neck lymphadenopathies. A diagnosis of thyroid carcinoma was made based on these findings. An FNAB was performed from the upper, middle, and lower aspects of the mass, which showed a high cellular yield composed of smooth outlined papillary fragments with fibrovascular core and cells having intranuclear pseudo-inclusion and longitudinal grooves, along with pigment-laden macrophages in a hemorrhagic background. A cytologic diagnosis of “suspicious for papillary thyroid carcinoma” (Bethesda V) was made, and an excisional biopsy was advised.
Therapeutic interventions
The patient was admitted to the pediatric surgical ward at JMC for elective surgery. The patient was kept on nil per os (NPO) and commenced on maintenance fluid and ceftriaxone. The patient underwent general anesthesia, and a total thyroidectomy was performed. The specimen was then sent to the Department of Pathology at JMC for histopathologic examination.
Gross and microscopic findings
Multiple small and one large irregular, firm tissue pieces were received. The aggregate measured 12 × 10 × 3 cm. The cut section showed grayish, dark-brown areas in the larger masses and cystic spaces filled with colloids in the smaller masses. No lymph nodes were present. Figures 1 and 2. On microscopic examination of Hematoxylin-eosin-stained sections, there was a papillary-like growth with a fibrovascular core, as well as solid sheets of round cells with limited cytoplasm. The chromatin appeared powdery, and the nuclei had a distinct orphan Annie-eye appearance, nuclear groove, and pseudo-nuclear inclusions. Additionally, there were areas of necrosis, hemorrhage, and calcifications. Based on these observations, a diagnosis of Classic variant PTC was made. It was not possible to perform immunohistochemistry and genetic testing due to the limited setup. Figures 3–5.

Gross findings.

Cut section through the larger mass (right) and smaller masses (left).
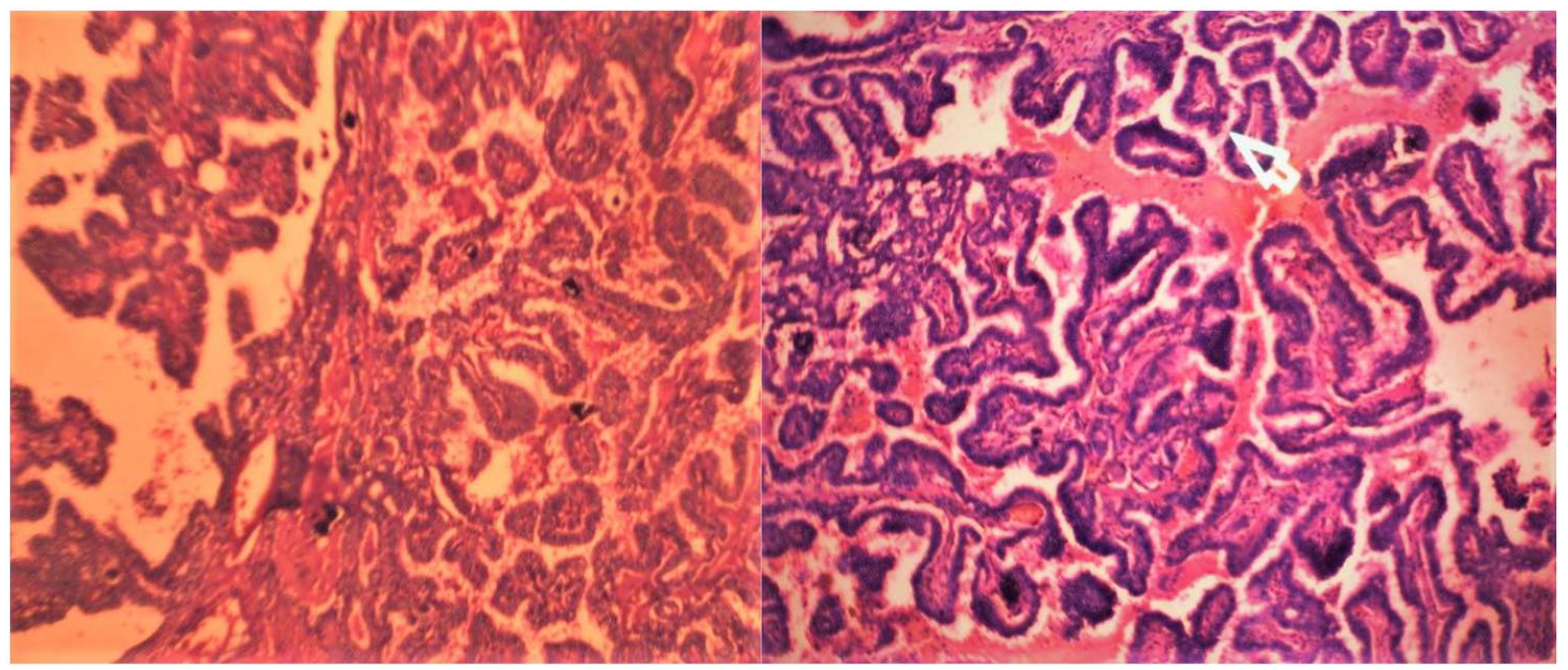
Low power view showing papillae and microvascular core.

High power view showing orphan Annie-eyed nuclei (yellow arrow) and longitudinal grooves (red arrow) (right) and pseudo-nuclear inclusions (white arrow) (left).

Medium power view showing papillae with orphan Annie-eyed nuclei (right) and calcifications (left).
Follow-up and outcomes
The patient remained in the hospital for 3 days after the surgery and was given morphine and ceftriaxone. He had a smooth recovery without any post-operative complications. The patient was prescribed 100 µg of thyroxine per day and was discharged with a follow-up appointment at a pediatric referral clinic scheduled in 2 weeks. During subsequent follow-ups over the next 4 years, both clinical and laboratory examinations were normal, and there were no signs of metastasis.
Discussion
Pediatric thyroid cancer is rare, but the risk of developing it increases significantly with radiation exposure. Other risk factors include a personal history of thyroid disease and a family history of thyroid cancer.1,11,20 The patient presented, however, had no identifiable risk factors. Based on data from the Surveillance, Epidemiology, and End Results Program (SEER) database, sporadic papillary thyroid cancer accounted for just 1.4% of childhood carcinomas diagnosed in the USA from 1975 to 1995. The rates have decreased over time, with 0.59 cases per 100,000 patients between 2007 and 2012 and 0.3 cases per 100,000 patients between 2000 and 2016.24–26
The incidence of thyroid cancer in children is 1:3.6 for males to females. However, this ratio decreases to 1.25:1 in children under 10.26,27 However, the incidence varies by age and gender, with males having a 6:1 higher incidence rate than females between ages 5 and 9. 24 The incidence of thyroid cancer peaks between the ages of 15 and 19 with an average age at diagnosis of 16 years.4,28 Here, our patient was 8 years old and presented with a 1-year duration of multiple swellings in the right lateral aspect of the neck. Others have reported thyroid carcinoma at 11, 15 months, 3, 5, 12, and 18 years.7,10,29–32
PTC behaves differently in children and adults. Pediatric PTC has distinct characteristics that set it apart from adult cases. These include a larger primary tumor during diagnosis, a higher incidence of neck lymph nodes and distant metastases at diagnosis, a greater likelihood of recurrences, and multifocality.3,33,34 The best predictors of recurrent disease are lymph node involvement, multiple thyroid nodules at presentation, and papillary or papillary-follicular histology. Recurrence rates are higher in children (35%–45%) than in adults (5%–20%).35,36 However, pediatric cancers have a better prognosis and respond better to therapy than adult cancers. 37 Pediatric cancers have a better prognosis and respond better to therapy than adult cancers. 35 Luckily, there was no recurrence during the 4-year follow-up period in our case.
Diagnosing thyroid cancer before surgery usually involves using different tests such as Thyroid function test (TFT), Ultrasound (US), Fine Needle Aspiration Biopsy (FNAB), scintigraphy, and molecular studies.1,7 US is the preferred method for examining the thyroid gland’s structure, while FNAB is the most precise test for diagnosing nodules. 38 In our situation, we initially used FNAB and US to make the diagnosis.
For pediatric PTC cases, studies suggest total or near-total thyroidectomy as the preferred procedure. Total thyroidectomy is recommended for multifocal tumor occurrence and bilateral lobe involvement, as seen in our case. When a child is diagnosed with malignant cytology, and there is clinical evidence of gross extrathyroidal invasion and/or locoregional metastasis on preoperative staging or intraoperative findings, it is recommended to perform Central Neck Dissection (CND). This approach may decrease the need for second surgical procedures and increase the chances of being free from the disease.23,24,35 As per the American Thyroid Association, performing a lateral neck dissection should only be considered for patients who show signs of metastases during clinical examination or through preoperative US or FNAB. If a patient is diagnosed with PTC and there is no clinical evidence of invasion or metastasis, the surgeon may consider performing a selective prophylactic CND based on the tumor’s location, size, and their own experience. For patients with a single tumor, the surgeon might perform an ipsilateral CND. If necessary, they can pursue contralateral CND based on intraoperative findings. This approach can help to balance the risks and benefits. However, there is no evidence to support the effectiveness of prophylactic neck dissection if there are no initial signs of palpable or radiological disease. Radioiodine therapy is indicated for the treatment of persistent disease that can’t be removed and distant metastases that respond to iodine.23,39 In our case, total thyroidectomy was done, lateral neck dissection and radioiodine ablation were deferred as per the guideline and the patient was put on 100 µg of thyroxine daily. The frozen section was not performed due to limited setup, hindering intraoperative options for lymph node dissection and outweighing risks and benefits.
Conclusion
This is an uncommon case of PTC in an Ethiopian child, with plenty of examples previously recorded in the literature but no such report of its occurrence in the country to our knowledge. When children under 10 have cervical masses, thyroid cancer should be considered. Palpable thyroid abnormalities should be investigated for possible malignancy. Palpable thyroid mass evaluation typically begins with a blood test to check thyroid function, along with US and FNAB. Currently, FNAB is the most reliable way to diagnose malignancy and determine the appropriate surgical approach. In most cases, treatment will involve a total thyroidectomy. Lymph node dissection is necessary only if lymph node disease is detected during preoperative evaluation.
Footnotes
Acknowledgements
We thank the patient for cooperating and consenting to the publication of this case report.
Authors’ contributions
B.H.T., as the corresponding author, prepared the case report, including the text and figures. T.D.B. and M.M.M. were responsible for performing the grossing and microscopic examination of the pathology sample and revising the case report. G.A.M. performed the surgery and edited the case report.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics statement
Case reports are exempt from ethical approval by the institutional review board (IRB) of Jimma University as long as written informed consent is obtained from the patient and identifying details are removed.
Informed consent
Written informed consent was obtained from the parents of the patient for their anonymized information to be published in this case report.