
Abstract
Introduction
Telephone consultation between physicians and patients is widely used in primary care and can provide a convenient alternative for the in-person visit. 1 One approach has been to substitute in-person follow-up visits (as compared with triage or urgent visits) with telephone consultation.2, 3 Implementation of telephone visits may have unique benefits and challenges for an underserved and immigrant population. Underserved patients may have restricted work schedules and limited resources for travel and value the convenience of a phone call. Home-bound elderly or disabled persons may similarly prefer telephone visits. However, language, cognitive, and literacy barriers may complicate scheduling and performing telephone visits in this population. Cultural preferences for in-person versus telephone visits may also be unique.
Gouverneur Health, an urban safety-net clinic in New York City, implemented in 2015 a quality improvement initiative to use telephone visits instead of in-person visits for regular follow-up in adult primary care. We aimed to determine the feasibility of using telephone visits with a culturally and linguistically diverse patient population. Secondary aims include characterizing patient and physician acceptability of telephone visits.
Methods
Patient Population
The study was conducted in the ambulatory care practice at Gouverneur Health in New York City. Gouverneur employs 20 predominately bilingual primary care providers and serves almost 9000 patients a year. This community-focused practice serves a culturally and linguistically diverse population. Only 24% of patients indicate English as their primary language, 40% are Spanish-speaking, and 20% speak Chinese dialects.
Intervention
The telephone visit pilot was conducted during a 6 month period in 2015, though the intervention has been sustained to present after the initial pilot data collection period ended. During the initial pilot period, only attending physicians were included. The project was introduced to the staff through a series of brief presentations at staff meetings during which the potential benefits of telephone medicine, guidelines for billing and documentation, and an orientation to the telephone visit note in the electronic health record were discussed. Physician participation in the pilot was optional.
Participating physicians determined at the end of an in-person visit whether or not a patient was eligible for telephone follow-up. Physicians excluded a patient from a telephone visit for a variety of reasons, including impaired patient communication or cognition or need for physical exam at follow-up. Patients could decline a telephone visit, even if the physician believed they were eligible. Patients received a scheduled time for a telephone call with their physician and a reminder call was performed prior similar to in-person visits, though telephone visits could be performed unscheduled as well. The number of telephone slots per session varied based on availability in the physicians schedule, but ideally were scheduled 1 per 3-hour session, and 2 per 4-hour session. A Frequently Asked Questions sheet for physicians and a flyer for patients were developed to clarify the billing and scheduling process.
Measures
Assessment of Patient Acceptability
Within a week after their telephone visit, all patients were contacted by a research assistant by phone for a brief (10 minutes) satisfaction survey. The survey was a modified version of previously developed instruments, but it also included de novo items.4,5 Surveys were conducted in English, Spanish, Mandarin, and Cantonese.
Assessment of Physician Acceptability
After 6 months of the telephone visit pilot, all physicians who conducted telephone visits (n = 10) completed a brief satisfaction survey. Physicians (including those who chose not to perform telephone visits) were also invited to participate in a focus group to elicit their beliefs regarding the logistical, organizational, and administrative barriers to conducting telephone follow-up visits, usefulness and suitability of telephone visit to address patient concerns, disadvantages, and advantages of using telephone visits, opinions on which patients benefit the most from the service, and suggestions for improving the process.
Patients and physicians could participate in the telephone visit pilot but choose not to participate in its evaluation. The New York University School of Medicine Institutional Review Board determined that the study should be considered a quality improvement project rather than research.
Analysis
Descriptive statistics were used for results of the patient and physician surveys and chart review. Focus groups were recorded and transcribed by the research assistant. The study team reviewed transcripts for themes. A sample of participating physicians reviewed focus group findings to verify completeness and accuracy.
Results
Data were collected from April 2015 to January 2016. During this time, 85 of a total 270 scheduled telephone visits were completed. This represents a “show rate” of 31% (85/270). Of the remaining scheduled telephone visits, 27% (73/270) of patients went in-person during the scheduled time either because of confusion or by choice, 25% (68/270) were unreachable (ie, patient did not answer phone or the phone went to voicemail, wrong number, or phone disconnected), 9% (24/270) refused the call (ie, patient was too busy to talk), and in 7% (20/270) the physician did not call the patient as scheduled.
Patient Satisfaction Survey
Seventy-five of the 85 patients (88%) who received telephone visits completed a survey about their experiences with the telephone visits (Figure 1). Overall, the majority of patients (84%) reported being highly satisfied with receiving telephone visits for their medical care. For example, over 90% of patients felt they could talk to their doctor about everything they wanted to on the telephone and that their doctor also understood them well. In contrast, approximately one-third did not like having a telephone visit with the doctor because the doctor could not touch or see them and 50% reported that they would prefer to discuss their medical problems with their doctor in person.
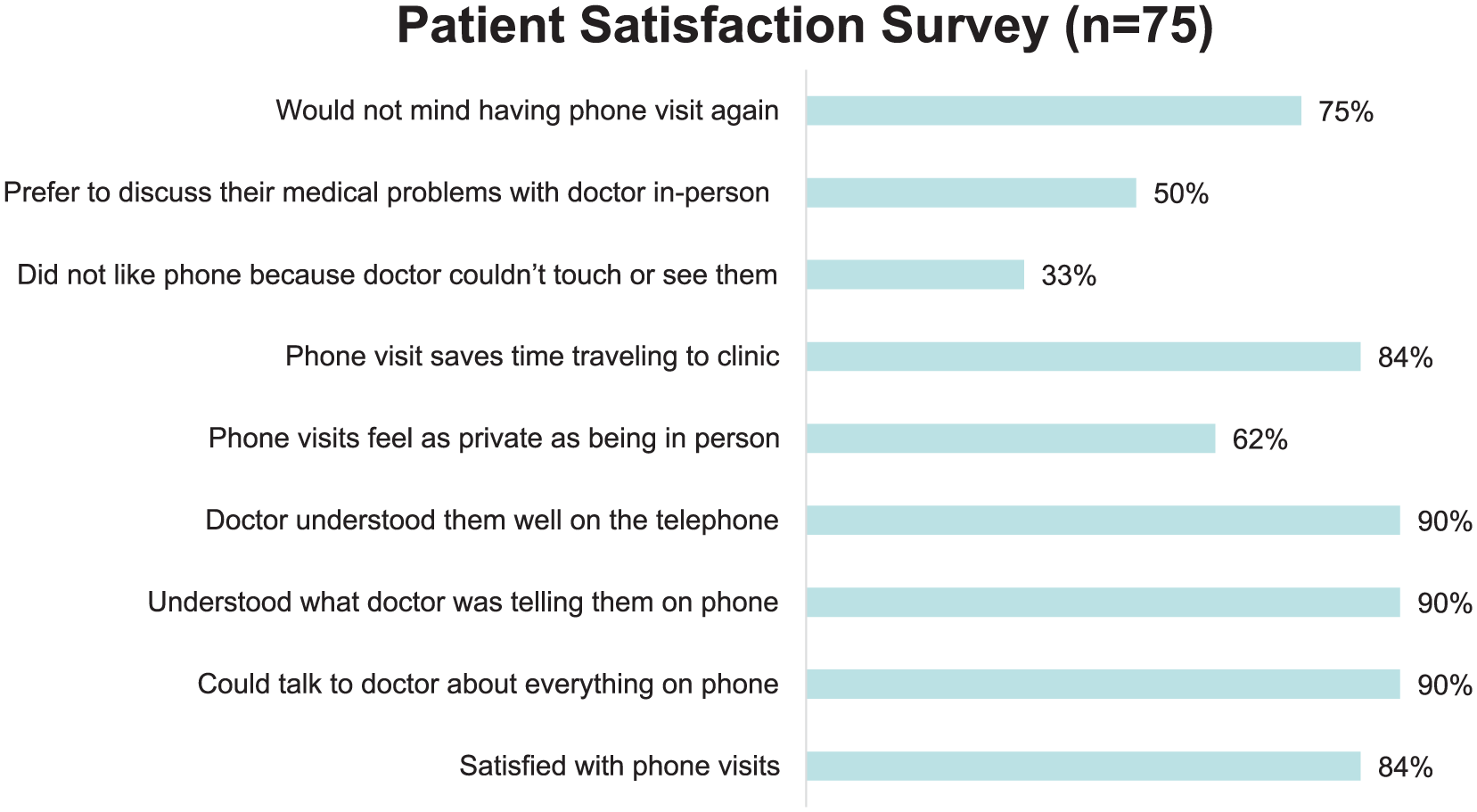
Patient satisfaction survey.
Physician Satisfaction Survey
Ten of the 20 primary care physicians in the practice opted to participate in the pilot and completed a survey about their experiences delivering medical care via telephone. All physicians felt they were able to communicate adequately with patients over the telephone; they could safely care for select patients over the phone; and that telephone visits could improve continuity of care for patients. Majority of physicians also felt that patients followed up on recommendations (eg, blood tests, vaccinations) after telephone visits just as much as they did for in-person visits (89%) and that telephone visits are more time efficient than in-person follow-up (78%).
In terms of the potential reach of telephone visits, on average, physicians estimated that telephone visits were appropriate for 27% (SD 19.8%; range 10%-60%) of their patients. The following services were considered the most appropriate for telephone visits: (a) lifestyle/behavioral counseling; (b) acute, nonemergency care (eg, flu symptoms); (c) medication titration; and (d) discussing laboratory results.
Physician Focus Groups
Two physician focus groups (n = 7 and n = 10, with some overlap in participation) were conducted in December 2015 and February 2016. Physicians who chose to participate in the telephone visit pilot were more likely to be advocates for the approach, and generally had very positive feedback. One of the focus groups included nonparticipating physicians, but we were unable to elicit reasons for nonparticipation.
Physicians who had participated in the pilot were very supportive of the intervention and the benefits of telephone visits. Specifically, they believed that telephone visits improved time management because of their brevity. One stated, “These televisits are gifts to me, they really help me to manage my days.” They felt that patients had different expectations for telephone calls, which made them more focused. For example, if a patient came in-person, they might expect laboratory tests to be done, but over the telephone this was not expected. One commented,
I think their (patients’) expectations is that you’re not going to spend an hour on the phone . . . it’s a different environment . . . it’s like the more they waited [in the clinic waiting room] the more you feel obligated to spend more time, and which on the phone is not a thing.
Many felt that formalizing the telephone visit helped them get “credit” for work that had previously been doing but did not have protected time for in their schedules. Physicians felt that telephone visits improved patient-centeredness through greater access to and continuity of care, and convenience for patients who did not have to take off work or travel to clinic.
Focus groups also provided valuable feedback on drawbacks of the implementation of telephone visits and recommendations for improvement. Issues such as scheduling, reminder calls, billing, and confusion about documentation were addressed. Physicians also commented on what types of patients and issues were most appropriate for telephone visits, such as medication management for chronic disease, discussion about laboratory test results, lifestyle counseling, and depression follow-up. They did not think telephone visits were appropriate for patients with cognitive challenges or hearing problems, diagnoses that require an examination or point-of-care testing, or new patients.
Discussion
We found that participating patients and physicians in an urban safety-net clinic serving a predominately immigrant population were highly satisfied with the use of telephone visits to replace in-person follow-up visits in primary care, though completion of the visits was low and only half of physicians participated. Physicians estimated that telephone visits were suitable for about one-third of their patients, and were most appropriately used for lifestyle/behavioral counseling, acute, nonemergency care (eg, flu symptoms), medication titration/chronic disease management, and discussing laboratory results. Physicians felt that the visits were efficient and improved their time management, and were patient-centered.
In our patient surveys, patients indicated that they were highly satisfied with their telephone visit (84%) yet preferred in-person visits (50%). While we did not conduct interviews or focus groups with patients and are unable account for this seeming contradiction, it may be that while patients found their immediate needs adequately met via telephone, they may find additional value in the rapport building of the in-person visit with their physician or interaction with other clinic staff. Prior qualitative work has shown that patients are more likely to address a wider range of issues and engage in small talk with their physician at in-person rather than telephone visits. 6 Focus groups performed before the implementation of scheduled telephone visits at the Veteran’s Administration primary care clinics found that patients viewed them as potentially beneficial for routine care but feared losing touch with their providers. 7
We encountered several implementation issues that other clinics considering telephone visits should consider. We found that telephone visits were most likely to be on time if scheduled at the beginning of a session rather than later when a physician was running behind. Only about a third of scheduled telephone visits were performed, in comparison to the clinic’s in-person show rate of 80%. Some patients were confused by the telephone visit and showed up in-person. Initially, some patients received automatic reminder calls misdirecting them to come in-person rather than await a phone call. The electronic health record initially did not automatically generate a billing sheet for telephone visits and required updating. The clinic’s largest payor, a Medicaid managed care organization, reimbursed for telephone visits, however the rest did not, including Medicare, and the clinic decided not to bill the uninsured.
We anticipated issues with recommended follow-up from the telephone visit. For example, arranging an appointment with a specialist or laboratory or radiology tests may need to be done on-site rather than remotely. However, on our survey the majority of the physicians felt that patients followed up on recommendations after telephone visits just as much as they did for in-person visits (89%), though we were unable to quantify this from chart review. Further research is needed to ensure that recommended care such as vaccines, HIV testing, or smoking cessation counseling that are provided on-site and same day are received by clinic patients who participate in telephone visits.
Physician participation was voluntary with only half of the 20 clinic physicians participating in the pilot, and survey data were limited to participating physicians. Nonparticipating physicians participated in focus groups, however they were mixed in groups with participating physicians. Perhaps for this reason among others, nonparticipating physicians were not as vocal and we were unable despite direct questioning to elicit reasons that physicians chose not to participate. In addition to logistical challenges such as scheduling and reminder calls associated with telephone visits, at the time of implementation, the clinic was experiencing several major workflow changes, including conversion from ICD-9 to ICD-10 and mandatory electronic prescribing, which may have decreased interest. Similarly, patients also could have chosen not to use a telephone visit even if their physician recommended it, and we did not collect data from those patients. Important operations variables such as whether telephone visits replaced in-person visits, or just added to the number of contacts that patients had with the clinic, were unable to be assessed. The length of our study also did not allow us to include important measures of chronic disease management such as hemoglobin A1c levels or blood pressure in the study population.
The use of telephone visits has been sustained in the Gouverneur Primary Care Clinic, and has now expanded to include nurses and nurse practitioners. The clinic is part of New York City Health and Hospitals, the largest safety-net system in the nation. In 2017, leadership at Health and Hospitals used information learned in the pilot to develop a strategy and workflow for dissemination of telephone visits across 17 ambulatory care facilities. Lessons learned from our implementation can be used to expand access and provision of high-quality primary care to other vulnerable populations.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a grant from NYC Health + Hospitals. The sponsor was not involved in the design and conduct of the study; collection, management, analysis, and interpretation of the data; and preparation, review, or approval of the manuscript.