
Abstract
This study measures waiting times and consultation times at convenient care clinics (CCCs), and compares them with equivalent times in traditional, family practice, physician offices. The analysis was limited to conditions most commonly treated at CCCs. It was found that patients using CCCs had significantly shorter waiting times from check-in to seeing a clinician than the equivalent waiting times reported by patients at family practice physicians’ offices and that CCC patients had significantly longer consultation times with the clinician than those reported by family practice patients. Applying a correction factor to adjust for potential differences between real waiting times and perceived waiting times did not substantially alter the conclusions. Shorter waiting times may increase satisfaction and thereby encourage patients to seek care; and spending additional time with the clinician may help ensure that all of a patient’s concerns or questions are addressed. This study provides objective evidence from a large database that CCCs provide prompt, satisfying care.
Keywords
Introduction
Patient satisfaction is considered an important dimension of the quality of health care.1-3 Two important determinants of satisfaction are how long the patient waits to see the clinician 4 and the duration of the consultation.5-7 Studies have shown that patients are often dissatisfied on both of these counts.5,6,8,9 However, the primary care physician shortage continues to grow in the United States 10 partly because of overwhelming work schedules, inefficient and unrewarding work environment,11,12 and also because of increasing demand due to aging population. 13 This might lead to patient satisfaction potentially deteriorating still further.
In recent years, alternative options for more convenient health care have become popular. For example, the use of convenient care clinics (CCCs) increased 10-fold between 2007 and 2009. 14 Also known as retail clinics, CCCs typically provide care on a walk-in basis for many common illnesses, in addition to providing basic preventive care and vaccinations. The intention of CCCs is to provide convenient services to patients—saving them time 15 and money16,17 and complementing the work of physicians. 18 However, we are unaware of any published studies that have examined either patient waiting times at CCCs or the amount of consultation time that CCC clinicians spend with their patients.
In this study, we sought to measure CCC waiting times and consultation times, and to compare our findings with comparable measures for traditional, family practice, physician office visits.
Study Data and Methods
We extracted de-identified encounter data from the electronic medical record (EMR) system of a national chain of convenient care clinics. We included patient encounters that occurred between January 1, 2007 and December 31, 2009. We limited our analysis to those encounters where the primary diagnosis code was for one of the conditions most commonly treated at CCCs, 19 namely, upper respiratory tract infection, sinusitis, bronchitis, pharyngitis, urinary tract infection, conjunctivitis, otitis media, and otitis externa. We excluded encounters in which the patient checked in but did not ultimately see a clinician.
A patient’s status throughout their CCC encounter is tracked via the clinic’s EMR. The EMR creates a timestamp at each of the following stages of the visit: when the patient checks in; when the clinician indicates that the consultation has started; when the clinician indicates that the consultation is complete; and any time that the patient spends waiting during the encounter (eg, when a patient remains in the examination room while waiting on test results). These timestamps allowed us to measure waiting times and consultation times as follows:
Time and day of encounters: the time of patient check-in based on the following categories: weekday encounters between start of business and 5 pm; weekday encounters between 5 pm and close of business; and weekend encounters between start of business on Saturday until close of business on Sunday.
Waiting time: the time, in minutes, from patient check-in until the time the clinician started the consultation; and
Consultation time: the time, in minutes, from when the clinician started the consultation until the time he or she completed the consultation, excluding any time spent waiting in between.
Data entry errors or IT errors sometimes generate unrealistic outliers in data. We therefore excluded from the CCC data, as outliers, those encounters with a waiting time greater than 5 hours or with a consultation time greater than 60 minutes.
We were unable to find any US studies that reported equivalent waiting times recorded in the EMRs of family physicians’ offices. Instead, we used self-reported waiting times from a 2007-2009 patient survey (Press Ganey Associates Inc). 20 For consultations with physicians listed under the category family physician, we obtained the following descriptive statistics: number of observations, mean, and standard deviation of patients’ self-reported waiting times. Specifically, this waiting time represents the patient’s estimate of how long they spent in the lobby waiting to be called plus the time they spent in the consultation room waiting to be seen by the physician.
We were likewise unable to find any U.S. studies that reported consultation times recorded in the EMR at family practitioners’ offices. To establish a benchmark for the face-to-face time that physicians spend with their patients, we used data from the 2007-2008 National Ambulatory Medical Care Survey (NAMCS). 21 The NAMCS survey represents a national sample of visits to non-federal employed office-based physicians who are primarily engaged in direct patient care. We extracted NAMCS encounters for physicians whose type of office setting for visits was defined as “private solo or group practice;” whose physician specialty was “general and family practice;” and whose physician specialty group was “primary care specialty.” We included only NAMCS encounters where the primary diagnosis code was one of the most commonly treated conditions at CCCs, as listed above. We used the variable “time spent with MD” as the measure of consultation time with the physician.
We calculated a range of descriptive statistics on the CCC EMR data, and we used 2-sample t tests to assess differences between the CCC data and the 2 benchmark groups. Statistical analyses were performed with SAS statistical software, version 9.2 (SAS Institute Inc, Cary, NC) and Microsoft Excel (2010).
Study Results
Table 1 shows the number of encounters, as well as the age and gender characteristics of the CCC study population and for the benchmark population for the family practice physician consultation time (NAMCS). We did not have this information available to us for the family practice physician waiting times (Press Ganey Pulse Report). Table 2 shows that 47.8% of the CCC encounters occurred outside of customary regular office hours.
Study Population Descriptives.

Abbreviations: CCC, convenient care clinic; NAMCS, National Ambulatory Medical Care Survey.
Study population encounters, including common conditions (upper respiratory tract infection, sinusitis, bronchitis, pharyngitis, urinary tract infection, conjunctivitis, otitis media, and otitis externa) encounters.
Convenient Care Clinic Encounters by Time and Day of Service.
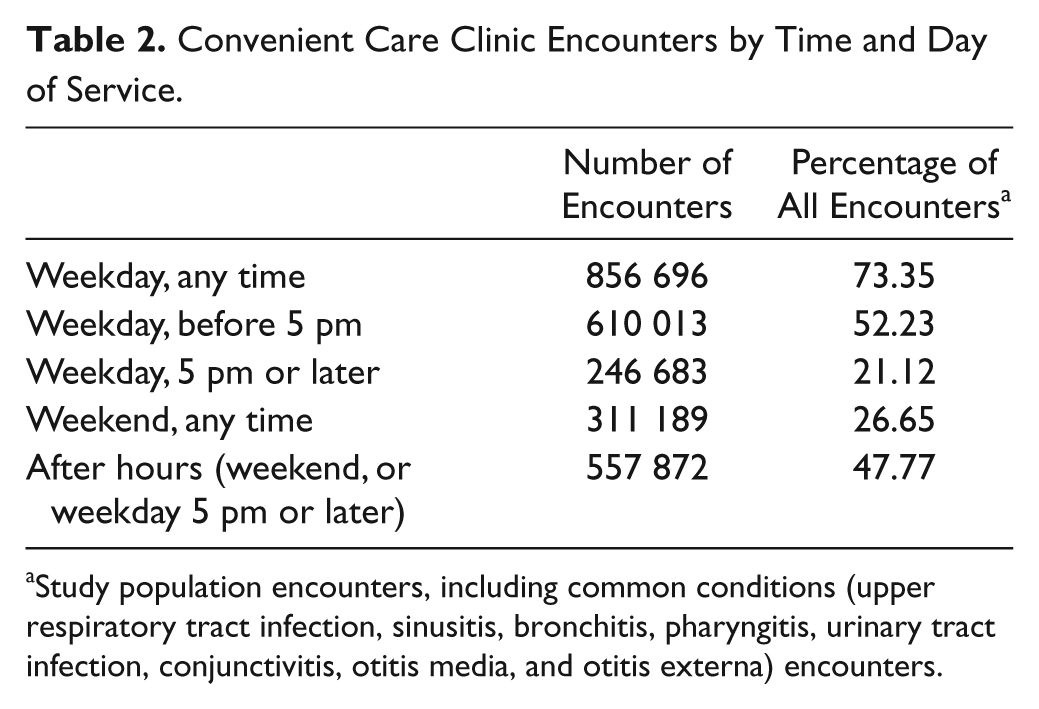
Study population encounters, including common conditions (upper respiratory tract infection, sinusitis, bronchitis, pharyngitis, urinary tract infection, conjunctivitis, otitis media, and otitis externa) encounters.
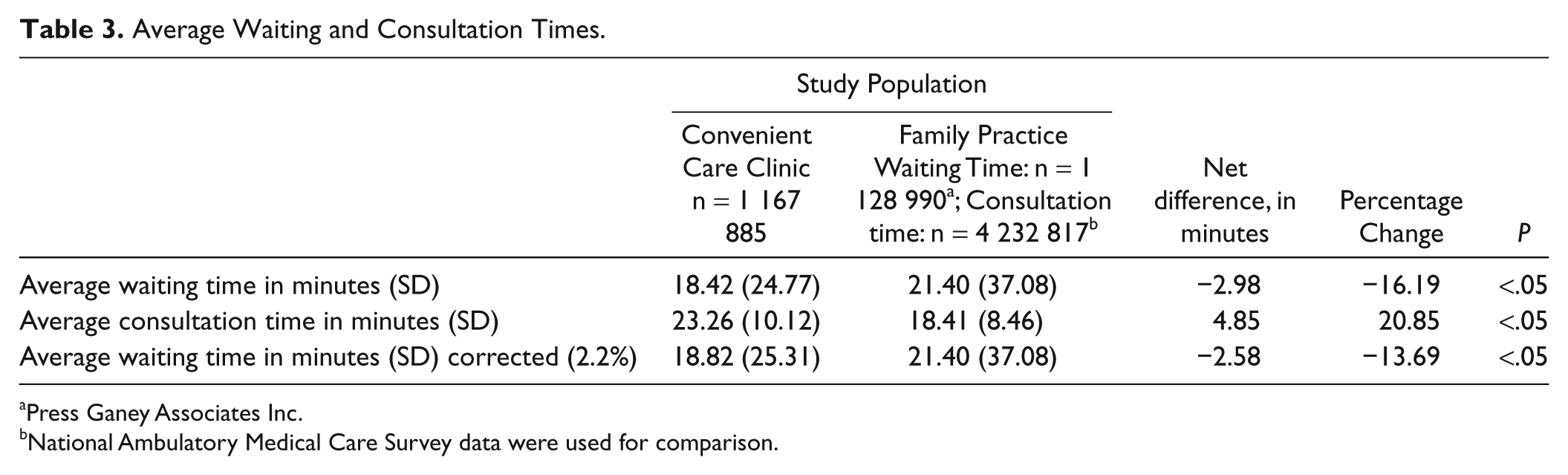
The mean waiting time for CCC patients was 18.4 minutes versus 21.4 minutes for the benchmark family practice patients (difference 3.0 minutes, 95% confidence interval CI = 3.1-2.9, P < .05; Table 3). Patients using CCCs had a mean consultation time of 23.3 minutes versus 18.4 minutes for the benchmark family practice patients (difference 4.9 minutes, 95% CI = 4.9-4.8, P < .05).
Average Waiting and Consultation Times.
Press Ganey Associates Inc.
National Ambulatory Medical Care Survey data were used for comparison.
Smidts and Pruyn 22 examined differences between actual and perceived waiting times in an outpatient clinic. The mean waiting times in their analysis were approximately 22 to 23 minutes, similar to those in the current study. Overall, Smidts and Pruyn found that, in this time range, patients overestimated their waiting time by 2.2% compared with the actual waiting time. When we applied this correction factor to our actual waiting time data to make them comparable to benchmark data, we found that the adjusted waiting time for CCC patients was 18.8 minutes for CCC patients versus 21.4 minutes for the benchmark family practice patients (adjusted difference 2.6 minutes, 95% CI = 2.7-2.5, P < .05). We did not use the corrected comparison for 2 reasons. Because of the lack of the raw data for the comparison group we had to convert the actual time to perceived time and we thought this maneuver awkward, though technically correct. Second, the difference did not affect the implication of our results much.
Discussion
We found that patients had significantly shorter waiting times at CCCs than the waiting times reported by patients at family practice physicians’ offices and that CCC patients had significantly longer consultation times than those reported by family practice patients. We believe this study is the first to examine the waiting times and consultation times for patients attending CCCs. One of the aims of CCCs is to provide convenient care, and this study provides objective evidence from a large database on these 2 metrics, as well as providing evidence that almost one half of encounters at CCCs are outside regular office hours.
The ability of CCCs to offer shorter waiting times for their patients has several implications. First, shorter waiting times may increase patient satisfaction. A study by Camacho et al 23 found that patients’ satisfaction with their providers decreased as perceived waiting time increased and that patients were less willing to return for care as their perceived waiting time increased. These findings suggest that patients who experience shorter waiting times might be more proactive with their preventive health care and be more likely to seek treatment when ill.
Although a convincing link is yet to be established between the duration of consultation time and health outcomes, the duration of face time with a clinician is considered to be an important indicator of high-quality health care. 24 A study conducted in 2007 for the Commonwealth Fund found that 44% of surveyed adults felt that their doctor did not spend sufficient time with them. 25 Having additional time with the clinician can help ensure that a patient’s needs are addressed, since the patient and clinician will have more time to discuss treatment options and any necessary preventative care. Taking the time to explain things more carefully could also help the patient to comprehend their clinician’s advice or instructions better, thereby increasing health literacy. 26 This increased communication could ultimately lead to better health outcomes (Committee on Health Literacy) 26 and increased patient satisfaction. 27
Limitations
Our study has a number of weaknesses, the most important being that the waiting time and consultation time estimates we used for physician offices were those perceived by patients, whereas for the CCC encounters they were the times recorded in the EMR. A number of studies have shown that patients’ perceptions of waiting times can be inaccurate,28,29 which is why we attempted to take account of this bias by applying a correction factor to our estimates. Many of the studies examining this issue have focused on patients attending emergency departments.30-33 However, Thompson et al 34 cautioned against using estimates from such studies because of the psychological factors involved. They argued that anxiety levels during emergency department visits affect patients’ perceptions of time, and that therefore the differences between perceived times and actual times seen in emergency room patients may not correspond to office visits, where we would generally expect anxiety levels to be lower.
Although we restricted our analysis to patients attending for the same list of primary diagnoses, we did not risk-adjust the CCC and family physician populations. For example, the average age and gender proportions in the 2 populations were different and might have contributed to the differences seen. Other potential confounders include income, ability to speak English, and the number and severity of comorbidities. However, although all these factors might help explain some of the differences we observed, from any given patient’s perspective, all other above issues being equal it is the unadjusted waiting time and consultation time that are important.
Finally, another limitation with our study is that we only considered one CCC network. The experiences of patients at other CCC networks may be different.
Conclusion
Patients using CCCs appear to experience relatively shorter waiting times and relatively longer consultation times for a range of common conditions. Further research will be required to compare wait times at CCCs during the weekday or during afterhours with EMR data from other health care settings, such as primary care physician offices, emergency departments, and urgent care centers. Additionally, it will be important to measure how waiting times and consultation times vary in each of these settings at different times of the day and by geographical variation, especially in medically underserved areas.
Footnotes
Acknowledgements
We wish to acknowledge insightful comments, suggestions, and proof checks while writing this article by many of our past and present colleagues at Outcomes & Analytics and Clinical Affairs at Walgreen Co.
Declaration of Conflicting Interests
The author(s) declared potential conflicts of interest with respect to the research, authorship, and/or publication of this article: this research was funded by Walgreen Co.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by Walgreen Co.