
Abstract
Introduction
In Sweden, the elderly population is growing, highly specialized care is performed in fewer healthcare units, and increasingly advanced health care is performed at home. These shifts are necessitating that health care providers adapt to changes in existing resources and overall health care costs. 1 The aging population, in connection with people living longer with various diseases and illness, presents major challenges requiring new solutions. Notably, health care quality and access are sometimes inequitably distributed, and the provided care does not always meet the patients’ expectations. Patients today often desire greater independence and more influence and control over decisions that affect their living situation. 2
The changing health care landscape will likely see greater use of various digital health systems (DHSs), 3 and according to the National Board of Health in Sweden, DHS means to use digital tools to exchange digital information in order to achieve and maintain health. 4 However, when considering the use of a DHS, there are several ethical aspects to consider. Health care providers must be aware that individuals show great variability in their ability to use new digital systems. Birkler and Dahl 5 discussed the potentially large gap between citizens’ access to digital technology and competence in using it. Moreover, Fuji et al 6 reported that some patients had apprehensions regarding the integrity and security of the information available online. Patients expressed concern that professionals other than the proper consultant might have access to their health information.
Despite concerns, the digital patient is emerging in response to the new health care environment. The adoption of new advanced information technologies (IT) to connect patients and health care providers means that contact and information exchange can occur at any time of the day. The Swedish Nursing Association notes that health care policies are being adapted to enable patients to become more involved in their own health care, and that new DHS technologies should involve diagnosis, consultation, treatment, and education. 7 Thus, there exists a need to examine patients’ experiences with digital care to guide the best possible implementation of technology in various health care systems.
Caregivers in Region Skåne of southern Sweden plan to implement a new digital primary health care (DPHC) service involving digital written patient dialogues. In the present pilot study, we aimed to explore the patients’ experiences and satisfaction with this DPHC service.
Method
Ethical approval for this study was obtained from the Regional Ethical Review Board in Lund, Sweden (Dnr: 2018/213), and the Office of Medical Service, southern Sweden.
This study included patients who called the Swedish Healthcare Guide by Phone (1177, advisory nurses) about a health condition. 8 Nurses identified the patients who were eligible for inclusion in this pilot study based on their symptoms. Appendix A lists the included symptoms. Eligible patients were informed about the available DPHC. Those who agreed to utilize the digital technology were given a web address (link) to a referenced website, legitimized with a personal bank identification (Bank.ID), and entered their medical history, including reason for contact, background disease(s), and current inconvenience. This record form was then digitally reviewed by a general practitioner (GP), who contacted the patient through a written digital dialogue that could potentially result in counseling, medical prescription, complemented examinations, and/or triage to another care level. All communication was conducted through written dialogues alone.
The GPs (n = 6) who managed the written dialogue were senior employees trained in the DPHC concept. In addition to symptoms, patient inclusion criteria were as follows: age >18 years, Swedish-speaking, and assessed by a nurse to be able to participate in the study. Patients were required to have access to digital technology (computer, telephone, or tablet) and access to the application Bank.ID, which enabled digital identification. Patients were excluded if their diagnoses did not meet the inclusion criteria, if the nurse determined that their anxiety and/or stress precluded study participation or that they were unable to understand information about the study, or if they lacked access to the application Bank.ID.
This study design involved the use of self-reported questionnaires with fixed response options (Appendix B). Patients were consecutively included from June 2018 to April 2019. Nurses working at the Healthcare Guide by Phone included patients all day and night, and the record forms were digitally handled by the selected GPs between 6
After the GP and patient had completed their asynchronous written dialogue, the patients were asked for their permission to send a questionnaire about their experiences, together with a written consent form. If an included patient did not respond to our survey within 4 weeks, a reminder was sent. The present study included 286 patients who agreed to participate after giving their informed consent and demographic data (eg, gender and age).
Statistics
The collected variables were analyzed using the statistical software SPSS version 24.0 (IBM Corp, Armonk, NY), and are described with absolute values (n) and relative frequencies (%), as appropriate. The questionnaire answer relative frequencies were dichotomized to evaluate positive response rates, based on a 5-degree index scale, to objectively obtain overall summaries according to the 3 domains: experience of communication, experience of technical functionality, and general experience of the concept. Index values were used to summarize the percentages, strengths, and appellations as follows: <0.20, no or very bad experience; 0.21 to 0.40, bad experience; 0.41 to 0.60, fairly good experience; 0.61 to 0.80, good experience; and 0.81 to 1.00, very good experience, as inspired by Altman. 9 These index values were described as question index values (Q-IV) and domain index values (D-IV). Finally, overall satisfaction with the concept was described with the median (Md) and interquartile range (IQR), based on a 10-point Likert-type scale.
Results
Table 1 presents the respondents’ demographics and overall satisfaction with the concept.
Demographic Data of the Patients. a
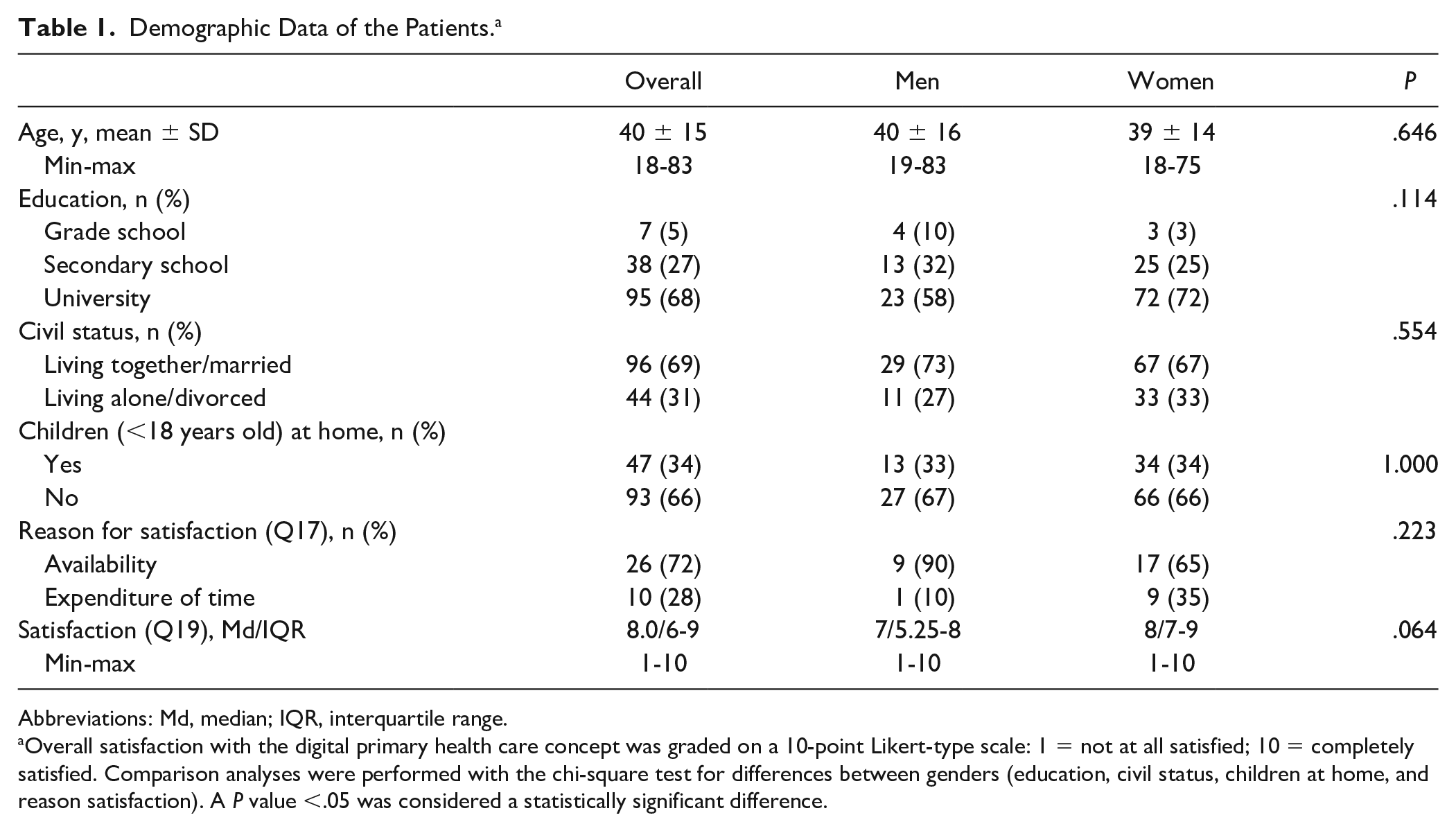
Abbreviations: Md, median; IQR, interquartile range.
Overall satisfaction with the digital primary health care concept was graded on a 10-point Likert-type scale: 1 = not at all satisfied; 10 = completely satisfied. Comparison analyses were performed with the chi-square test for differences between genders (education, civil status, children at home, and reason satisfaction). A P value <.05 was considered a statistically significant difference.
Table 2 presents the respondents’ overall experiences, summarized as percentages, strengths, and appellations.
Present Domain Index Values (D-IV) Summarize the Percentages, Strengths, and Experience Appellations. a

Evaluation inspired by Altman (1991). <0.20 = no or very bad experience; 0.21-0.40 = bad experience; 0.41-0.60 = fairly good experience; 0.61-0.80 = good experience; and 0.81-1.00 = very good experience. The overall experience is described as a mean D-IV.
Communication
Table 3 presents the overall relative answers to questions in the domain communication. The D-IV of 0.57 suggested a fairly good experience regarding communication abilities (Table 2). Patients expressed that the DPHC concept imposed limitations in communication compared with a personal visit (Q1), and carried a risk of incorrect assessment (Q2). However, the majority of patients felt validated (Q3) and had a sense of trust in the communication (Q4) through the written dialogue. Compared to a personal visit, patients felt that the written dialogue provided the same opportunity for advice, support, and teaching (Q5), and that some specific female/male diseases were easier to communicate with the DPHC concept (Q8).
Domain Communication: Summary of Relative Questions Values, Answer Options, a Question Index Value (Q-IV), and a Mean Domain Index Value (D-IV). a
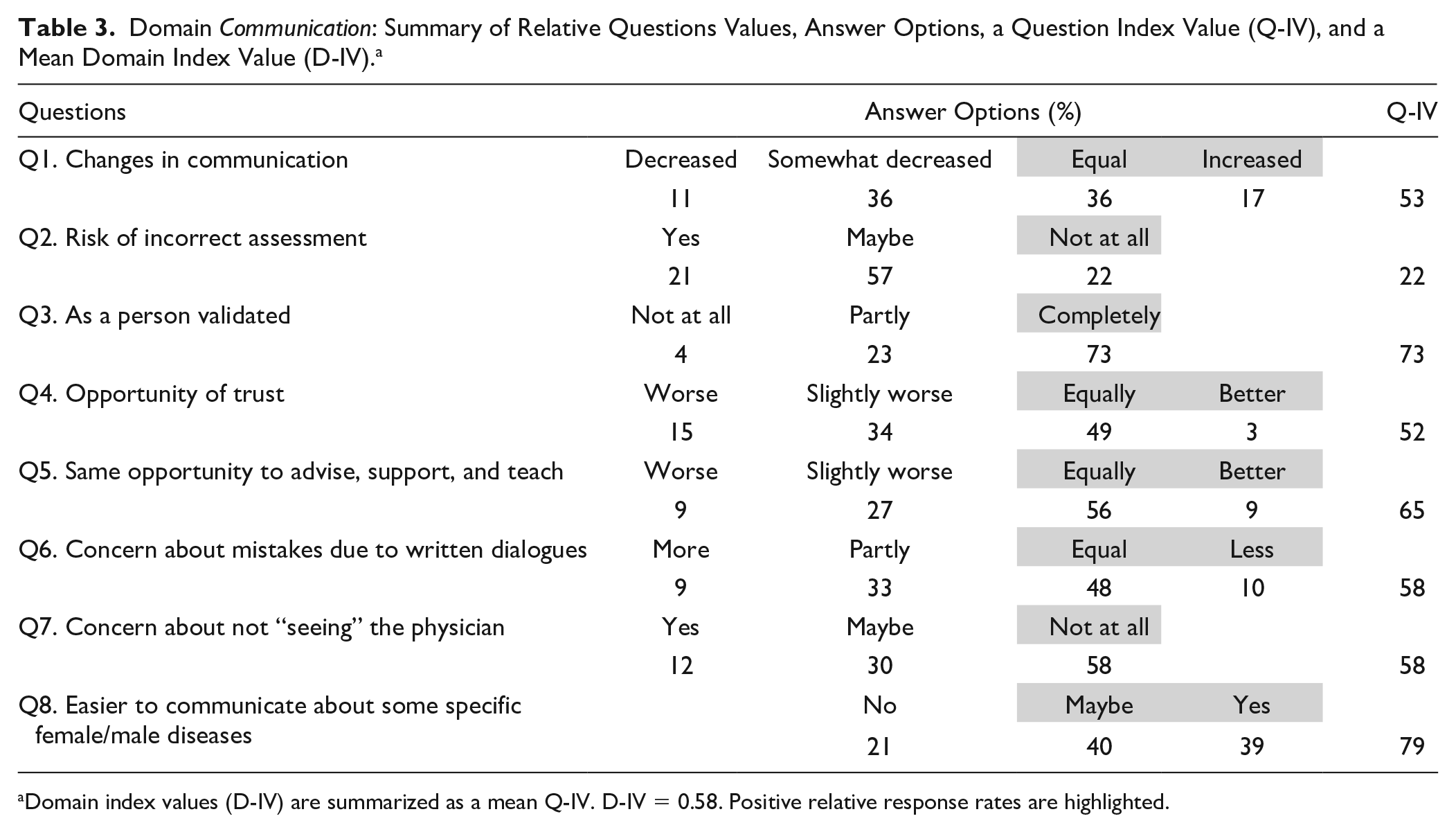
Domain index values (D-IV) are summarized as a mean Q-IV. D-IV = 0.58. Positive relative response rates are highlighted.
Technical Functionality
In the domain technical functionality, patients described their experience as good, with a D-IV of 0.80 (Table 2). The patients felt the technical design was very reliable (Q9) and that the IT was safe to use (Q10), and expressed that the concept entailed reasonable processing times (Q11) (Table 4).
Domain Technical Functionality: Summary of Relative Questions Values, Answer Options, a Question Index Value (Q-IV), and a Mean Domain Index Value (D-IV).

Domain index values (D-IV) are summarized as a mean Q-IV. D-IV = 0.80. Positive relative response rates are highlighted.
General Experience of Digital Primary Health Care
This domain showed a positive trend, with a D-IV of 0.76 (Table 2), and the Q-IV varying between 0.72 and 0.96 (Table 5). The patients felt well prepared (Q12) and thought that the time aspect was reasonable (Q13). They expressed some uncertainty regarding the physician’s ability to assess correct care needs (Q14: Q-IV of 0.47). However, 81% of the patients would recommend this DPHC concept to others (Q18), and a majority of the patients (72%) experienced equal or greater satisfaction with the service compared with a physical visit (Q16). Among those patients who were more satisfied with the DPHC concept (n = 36; 26%), their main reason was availability (Q17, Table 1). These responses correspond well with the overall satisfaction with DPHC (Md, 8.0; IQR, 6-9; Q19) (Table 1).
Domain General Experiences of Digital Primary Health Care: Summary of Relative Questions Values, Answer Options, a Question Index Value (Q-IV), and a Mean Domain Index Value (D-IV). a

Domain index values (D-IV) are summarized as a mean Q-IV. D-IV = 0.76. Positive relative response rates are highlighted.
Discussion
In the present pilot study, we aimed to explore patients’ experiences with DPHC using written dialogues. Our results demonstrated that the patients had an overall good experience with the concept. Notably, our findings could be affected by our respondent population, since the patients themselves agreed to use the digital concept. The population demographics reveal a fairly young population, with a clear majority of female respondents. This is in line with a stakeholder survey of potential users/patients of digital care, which indicated that a majority of potential users would be women (>70%) aged between 18 and 40 years. 2 Moreover, in line with the results of a Swedish eHealth Agency survey, 10 we found that respondents were open to solutions that could increase access to care, and availability was a reason for satisfaction in our study.
In the communication domain, the participating patients answered that the DPHC concept entailed acceptable communication opportunities, but that the service involved significant changes compared to a personal visit. The patient responses indicated that our concept met the most common types of needs (eg, making the patient feel validated, allowing the patient to feel trust in the communication, and representing an opportunity for advice, support, and teaching), and was responsive to the individual patient’s choices and preferences. We think that this is an important result, as it suggests that the DPHC design was successful in meeting expectations and maintaining a certain level of quality in the digital “meeting.”
In the technical functionality domain, the patients perceived the DPHC IT to be safe for use, possibly related to the fact that the patients had to log in using a bank-ID. This is somewhat in contrast with previous reports that patients were commonly concerned about the integrity and security of information available online. 6 Birkler and Dahl 5 describe 3 main areas of digital security: integrity, accessibility, and confidentiality. Integrity refers to adequate documentation, meaning that the dialogue must be stringently managed when sent, saved, or used in other situations, and accessibility refers to the limitations regarding access to documentation. Notably, when information is saved, it is may become available to someone else, and thus it is not possible to completely protect any information—analog or digital. Confidentiality refers to ensuring that sensitive data are not circulated, which requires great vigilance from users. We believe that the digital patient is aware of the described difficulties, but that patients are accustomed to using digital media in various contexts, and are thus inclined to trust the system and its storage of patient data. However, this is a vast and complicated area that must be further discussed.
With regards to general experience with DPHC, we found overall positive trends. The patients reported that they felt well prepared to use the system, and found the time aspects involved with the asynchronous dialogue to be reasonable. However, only about 50% of respondents felt that the GP had the ability to correctly assess care needs in this system, which can be considered a threat to patient safety. In the situation of nurses providing counseling by telephone, it has previously been reported that both healthcare providers and patients can jeopardize patient safety when detailed communication is lacking. 11
Unfortunately, based on the present pilot study, we cannot determine why the patients perceived a decreased ability to correctly assess care needs in the DPHC setting. It might be because the GPs could not examine vital parameters and/or perform an extended physical examination. Camtö in Sweden has mapped out the benefits and risks of various healthcare methods, and has determined that diagnoses are normally based on the patient’s story (history) and a body examination (status), such that it may not be ideal to assess symptoms in digital dialogues without meeting the patient. 12 However, the patients included in our study had symptoms of diseases and illness that do not necessarily require a physical examination. Future work must be performed to determine which symptoms (and which corresponding patient groups) are most suitable for similar digital healthcare concepts. Importantly, despite various opinions and patient experiences, over 75% of the respondents stated that they would recommend the DPHC to others. Among those patients who were more satisfied with the DPHC than with a physical visit, their main reason for satisfaction seemed to be availability.
The development of relevant, usable, and effective digital health solutions likely requires the assessment of patients’ experiences to guide the design of effective eHealth concepts. 13 It has been suggested that patient-designed and patient-centered digital health tools are more likely to bridge the gap between existing eHealth concepts and the populations that would most benefit, and to realize the full potential of digital eHealth. 14 Based on the results of our present pilot study, we think that a qualitative evaluation is needed to clarify the patients essential experiences and to acquire greater insight into various digital-based concepts.
Strengths and Limitations
It is normally advantageous if existing validated surveys or questions can be used; however, we could not find any existing questionnaire survey suitable for the purpose of our pilot study. Therefore, we conducted literature research to identify queries that emerged in care relationships where patients and caregivers did not have a physical meeting. Based on this research, we believe that our questionnaire questions had reasonable construct validity to investigate nuances of the patients’ experiences with the digital care according to our purpose.
Questionnaire surveys are probably the most common means of asking for information, but normally yield a low response rate. However, low response rates to questionnaires are not necessarily a major cause for concern. The most important factor is that the respondents are representative of the target group being investigated. Studies in Sweden indicate that responses will be received from up to 75% of people older than 70 years, compared with only 40% of persons aged 20 to 24 years. Additionally, women respond more often than men, and highly educated persons respond at a higher rate than individuals with lower education. 15 Thus, the response rate in our pilot study corresponds quite well to our informants’ demographic. Nevertheless, the inability to capture responses from all patient categories, who may be using new digital technologies in the future, may produce a rather misleading picture of reality.
Conclusion and Implications
The patients in our pilot study expressed their satisfaction and described good experiences with the concept of digital primary health care using written dialogues. These findings shed light on the experience of DPHS, and this examination of patient experiences may support decision makers and practitioners in scaling-up digital primary care. The present work provides a knowledge base that will be useful for other areas and countries that intend to implement digital health services into their primary health care systems.
Footnotes
Appendix A
Appendix B
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.