
Abstract
Background:
Burnout has risen sharply since the COVID-19 pandemic, especially in healthcare. Emerging evidence suggests adverse childhood experiences (ACEs) may increase burnout risk. This study examined the relationship between burnout and ACEs within the maternal and child health (MCH) workforce and assessed ACE prevalence.
Methods:
An anonymous cross-sectional survey of MCH clinicians (n = 477) was administered via Qualtrics. Eligibility included being ≥18 years old, working in the MCH workforce, and practicing ≥1 year. Burnout was assessed using the Maslach Burnout Inventory-Human Services Survey (MBI-HSS). ACEs were measured using the ACE questionnaire with minor wording modification. ANOVA and linear regression were used to evaluate associations between ACE exposure and burnout.
Results:
Over half (57%) reported ≥1 ACE; 31% reported ≥4. Burnout levels were high (Personal Accomplishment = 26.47 ± 8.94; Emotional Exhaustion = 32.98 ± 8.56; and Depersonalization = 15.62 ± 5.82). Participants with ≥4 ACEs had significantly higher emotional exhaustion and lower personal accomplishment. Those with 1 to 2 ACEs had lower emotional exhaustion and depersonalization than those with zero ACEs.
Conclusion:
The MCH workforce shows a high prevalence of ACEs and elevated burnout. A dose-response relationship was observed, with ≥4 ACEs associated with greater burnout. However, lower burnout among those with 1 to 2 ACEs suggests possible resilience pathways. Workforce programs should account for early life adversity and integrate resilience-informed approaches.
Background
Burnout among healthcare professionals is a growing public health concern, with implications for workforce retention, quality of care, and patient outcomes. Emerging evidence suggests that individual-level factors, including early life adversity, may contribute to burnout risk. However, little is known about how adverse childhood experiences (ACEs) shape burnout among maternal and child health (MCH) clinicians.1-4
The United States continues to have poorer maternal and child health (MCH) outcomes among high-income countries. In 2023, 10.4% of births were premature, 1 and persistent inequalities disproportionally affect Black mothers who experience significantly higher rates of adverse outcomes.2,3 The national maternal mortality rate in 2022 was 22.3 deaths per 100 000 live births. 3 These disparities reflect broader structural and systemic challenges, including fragmented care delivery, policy barriers, and unequal access to resources. 4 These conditions shape the clinical environments in which MCH providers work and may contribute to increased occupational stress and burnout.
A well-supported, community-oriented, and culturally responsive MCH workforce is essential to improving these outcomes. However, burnout has increased across the healthcare workforce in recent years among clinicians in patient-facing roles.5-7 Burnout is characterized by emotional exhaustion, depersonalization, and reduced personal accomplishment, and has been associated with high workload, emotional labor, and reduced well-being.7-10 Burnout is also linked to increased medical errors,11,12 workforce attrition,13,14 and reduced quality of care further exacerbating strain on already overburdened systems. 15 Between 2020 and 2021, the U.S. nursing workforce declined by more than 100 000 clinicians which is the largest drop observed in 4 decades. 16 The MCH workforce may be particularly vulnerable due to its predominantly female composition, emotionally intensive care roles, and the broader sociopolitical context in which care is delivered. 17
Adverse Childhood Experiences (ACEs) refer to potentially traumatic events occurring before 18 years of age, including various forms of abuse, neglect, and household dysfunction. 18 ACE scores represent the cumulative number of such experiences, with 4 or more ACEs commonly considered a high-risk threshold associated with poorer physical and mental health outcomes in adulthood.19,20 Nationally, 63% of U.S. adults report at least 1 ACE, with higher prevalence observed among women. 21 Among healthcare professionals, approximately 68% report at least 1 ACE, and female clinicians are more likely than their male counterparts to report higher ACE exposure.22,23 Given that the MCH workforce is predominantly female and engaged in emotionally demanding care, this population may carry a disproportionate burden of early life adversity. These experiences may shape stress responses, coping strategies, and vulnerability to burnout in clinical practice.
Emerging studies have begun to identify associations between ACE exposure and burnout among physicians and trainees, suggesting that early life adversity may influence professional well-being. 24 However, this literature remains limited in scope and has not examined these relationships within the MCH workforce, a population uniquely positioned at the intersection of high emotional labor, complex patient needs, and systemic health inequities. Understanding how ACEs relate to burnout in this workforce may provide critical insight into the development of trauma-informed and resilience-oriented workforce interventions.
Therefore, the purpose of this study was to (1) estimate ACE prevalence in the MCH workforce and characterize burnout levels, and (2) examine associations between ACE exposure and burnout subscales.
Methods
Study Design and Eligibility Criteria
This study employed an anonymous, cross-sectional survey design administered via Qualtrics. The survey aimed to assess burnout and early life adversity among maternal and child health (MCH) clinicians.
Participants were recruited through dissemination of the survey link across professional networks, clinical organizations, social media platforms, and community-based groups serving the MCH workforce. Recruitment materials described the study purpose, voluntary nature of participation, and anonymity of responses. No financial compensation was provided.
Eligible participants were individuals aged 18 years or older who were currently working in the MCH workforce (full-time or part-time) and had at least 1 year of clinical experience. For the purposes of this study, the MCH workforce was defined as clinicians providing direct care to maternal and/or pediatric populations, including doulas, midwives, obstetrician-gynecologists, primary care providers, labor and delivery nurses, pediatricians, and family medicine clinicians. Electronic informed consent was obtained from all participants prior to the start of the survey.
The survey included additional items beyond those analyzed in the present study as part of a broader investigation of MCH workforce experiences. Only measures relevant to ACE exposure and burnout are included in this analysis. The full survey instrument is provided as Supplemental File 1.
Instruments
Adverse childhood experiences (ACEs) were assessed using a 10-item questionnaire adapted from the original Kaiser Permanente-Centers for Disease Control and Prevention ACE Study instrument. 26 The instrument measures exposure to abuse (emotional, physical, sexual), neglect, and household dysfunction occurring before 18 years of age. ACE scores were calculated as the sum of endorsed items (range: 0-10), with higher scores indicating greater exposure to early life adversity. Consistent with prior literature, a score of 4 or more ACEs was considered a high-risk threshold. 20
One item was modified for clarity and cultural relevance: the original item, “Did you live with an adult who had a problem with drugs or alcohol?” was adapted to “Were your parents ever too drunk or high to take care of you or take you to the doctor?” This wording has been used in prior ACE-related research and was selected to improve interpretability across diverse respondent backgrounds while maintaining alignment with the original construct.
Although ACE questionnaires are widely used in both research and clinical settings, there is no single standardized instrument used uniformly across the United States. The version used in this study retains the core domains of the original ACE framework and is consistent with commonly used adaptations in the literature.
Burnout was assessed using the Maslach Burnout Inventory-Human Services Survey (MBI-HSS), a validated and widely used measure of burnout among healthcare professionals.27 The MBI-HSS consists of 3 subscales: emotional exhaustion (EE), depersonalization (DP), and personal accomplishment (PA). Higher scores on emotional exhaustion and depersonalization and lower scores on personal accomplishment indicate greater burnout. Subscale scores were calculated according to standard scoring procedures. 27
Recruitment
The survey was disseminated via clinical networks, professional associations, social media groups, and community-based organizations serving the MCH workforce. Due to convenience sampling and varied organizational responses, some networks did not distribute the survey, potentially contributing to non-response bias.
Statistical Analysis
Descriptive statistics summarized demographic characteristics, ACE prevalence, and burnout scores. Independent t-tests and 1-way ANOVA assessed bivariate associations between ACE exposure and burnout. Multivariable linear regression models evaluated independent associations between ACE categories and burnout subscales, controlling for demographic and occupational covariates.
Results
Demographics for study participants can be found in Table 1. Participants were primarily 30 to 39 years old, female, white, and mostly working full-time in clinical settings. Physicians, certified nurse-midwives, and nurse practitioners were most professional groups (Table 1).
Demographics.

Included in Other are people who identified as Middle Eastern or North African, Mixed, or Native Hawaiian or Pacific Islander.
MBI
For MBI subscales, the mean Personal Accomplishment was low (M = 26.47, SD = 8.94), Emotional Exhaustion was high (M = 32.98, SD = 8.56), and depersonalization was high (M = 15.62, SD = 5.82). Burnout among the sample was high. Means for all 22 MBI statements can be found in Table 2.
MBI Scale Scores.

ACEs
Characteristics of ACEs in the sample can be found in Tables 3 and 4. Fifty-seven percent reported ≥1 ACE, and 31% reported ≥4 ACEs. Emotional and physical abuse were the most prevalent ACE categories.
ACE Exposure Among Participants.

Totals reflect complete ACE item responses; missing data were excluded listwise, resulting in fewer than 477 total responses.
ACE Exposure by Category and Count.
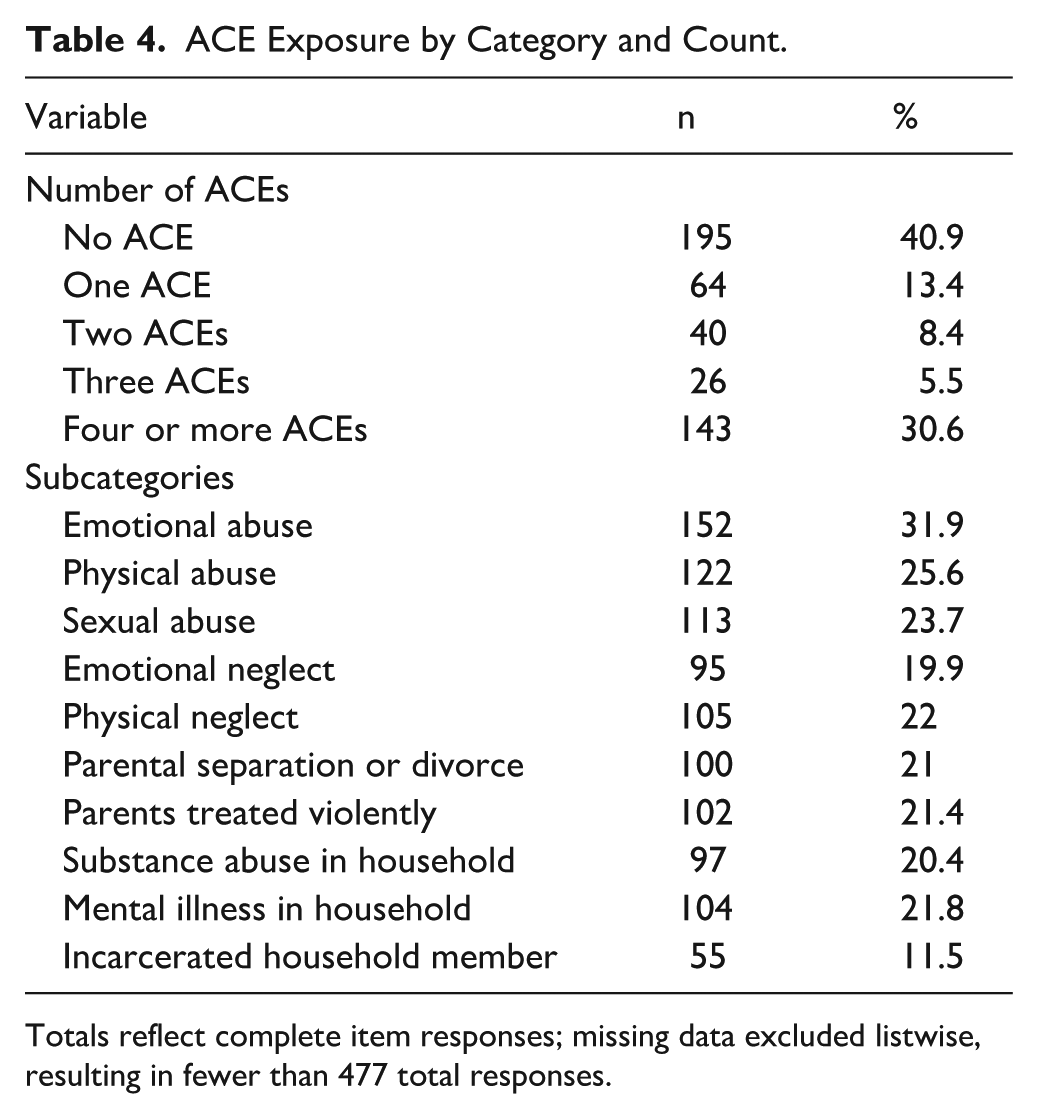
Totals reflect complete item responses; missing data excluded listwise, resulting in fewer than 477 total responses.
An independent samples t-test was used to determine a association between the 3 MBI subscales and not having an ACE and having at least 1 ACE. Results can be found in Table 5. Participants with ≥1 ACE had significantly lower PA scores compared to those with no ACEs. Differences in EE and DP were not statistically significant in bivariate comparisons.
Burnout Subscales by ACE Group (Independent Samples t-Test).

Independent samples t-tests compare participants with ≥1 ACE to those reporting no ACEs. Significant at P < .001.
A 1-way ANOVA compared burnout subscales across ACE exposure levels (0, 1, 2, 3, and ≥4 ACEs). Results can be found in Table 6. The mean differences between groups for Personal Accomplishment (F = 4.212), Emotional Exhaustion (F = 5.635), and Depersonalization (F = 8.068) were all statistically significant (PA P = .002; EE P < .001; and DP P < .001). Burnout differed significantly by ACE exposure, with ≥4 ACEs associated with highest emotional exhaustion and lowest personal accomplishment (Table 6).
One-Way ANOVA Results for Burnout Subscales Across ACE Exposure Levels.

Results reflect 1-way ANOVA comparing mean burnout scores across ACE exposure categories (0, 1, 2, 3, ≥4). *Significant at P < .005. **Significant at P < .001.
Linear regression
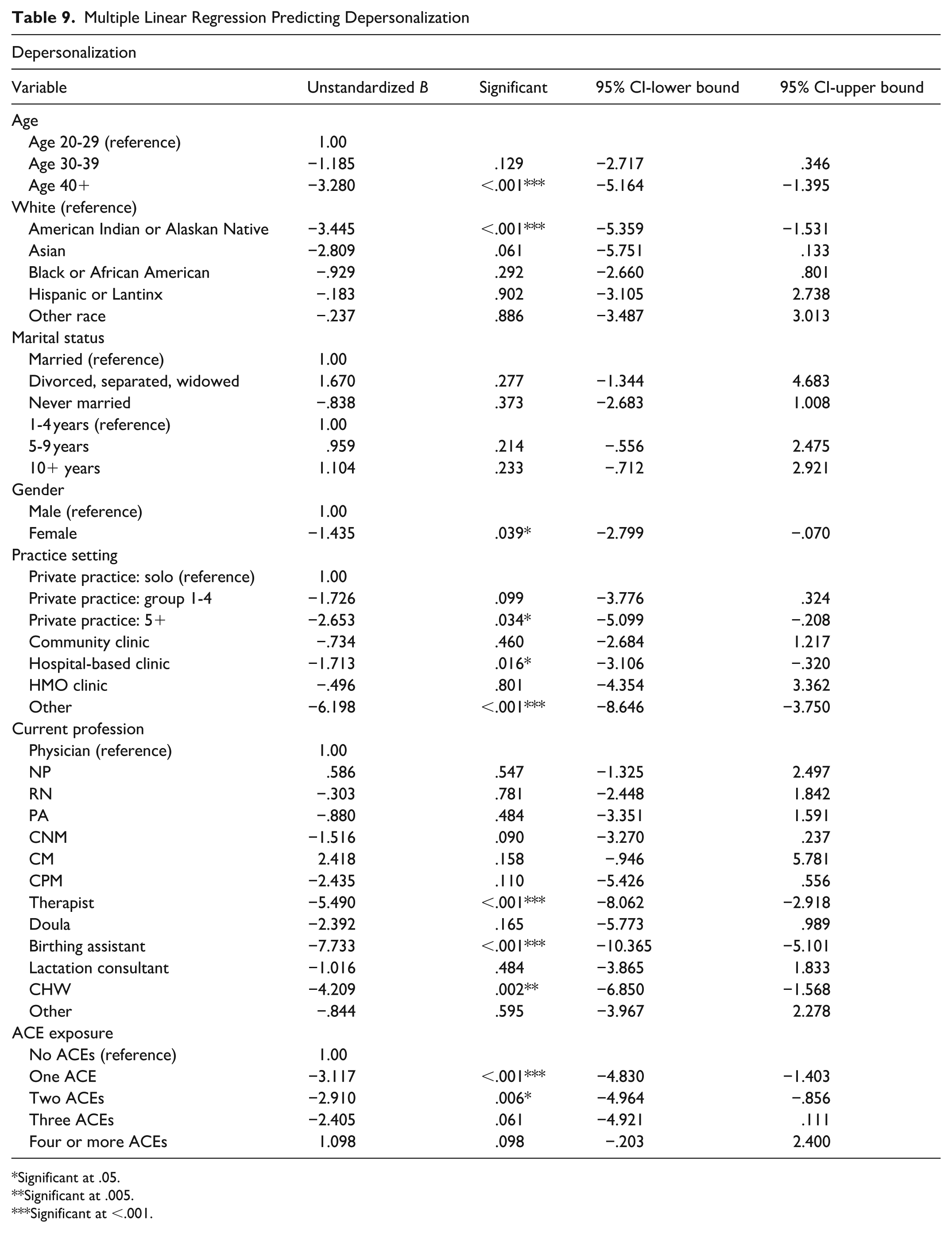
Multiple linear regression controlled for age, race, marital status, working length of time, gender, practice setting, current profession, and ACEs across all 3 MBI scales. Full regression results for personal accomplishment, emotional exhaustion, and depersonalization are shown in Tables 7 to 9. Participants with ≥4 ACEs reported significantly higher emotional exhaustion and lower personal accomplishment. In contrast, those with 1 to 2 ACEs showed significantly lower emotional exhaustion and depersonalization compared to those with no ACEs. Older clinicians and individuals in certain professional roles demonstrated lower burnout across subscales.
Multiple Linear Regression Predicting Personal Accomplishment.

Significant at .05.
Significant at .005.
Significant at <.001.
Multiple Linear Regression Predicting Emotional Exhaustion.

Significant at .05.
Significant at .005.
Significant at <.001.
Multiple Linear Regression Predicting Depersonalization
Significant at .05.
Significant at .005.
Significant at <.001.
Even after adjustment, those with ≥4 ACEs had significantly lower PA compared to those with without ACEs. Several non-physician roles also showed lower PA compared to physicians. Practice setting was also associated with burnout outcomes, with several non-private practice settings demonstrating lower personal accomplishment compared to solo private practice (Table 7). MCH workers with ≥4 ACEs had significantly higher EE, while those with 1 ACE had significantly lower EE compared to those with none (Table 8). Participants with 1 or 2 ACEs had significantly lower DP compared to those with no ACEs. Those with ≥4 ACEs were still associated with higher DP, though not statistically significant (Table 9).
Discussion
One-third of the sample had a ≥4 high-risk ACE score in this sample of MCH workers. This is a much larger proportion relative to national estimates, 21 suggesting that a sizable portion of the workforce has experienced multiple forms of early life adversity. These experiences may influence emotional resilience and stress responses within the clinical environment. It is also possible that individuals who have experienced early adversity are drawn to caregiving professions, such as MCH, due to personal meaning derived from prior experiences, as over half of the sample reported at least 1 ACE.
Overall, the results are consistent with literature demonstrating a dose-response relationship between ACEs and health outcomes, 25 as well as emerging evidence linking ACE exposure to burnout.30 In this study, individuals with ≥4 ACEs consistently demonstrated higher burnout symptoms, particularly higher emotional exhaustion and lower personal accomplishment, even after adjusting for demographic and occupational factors. Depersonalization was also higher among those with ≥4 ACEs, although not statistically significant, which may reflect a threshold effect or sample-related limitations.
Interestingly, individuals reporting 1 or 2 ACEs demonstrated significantly lower levels of emotional exhaustion and depersonalization compared to those with no ACE exposure. Some studies have explored the relationship between early adversity and resilience, suggesting that positive outcomes may be mediated by factors such as emotional support from family, peers, and community, as well as internal characteristics like optimism, coping skills, and interpersonal relationships. 26 These findings may indicate adaptive coping or resilience among clinicians with moderate exposure to adversity. The path to becoming a healthcare professional often requires navigating challenges and setbacks, and individuals with prior adversity may enter training with developed coping strategies that buffer workplace stress.
The MCH workforce represents a unique population, characterized by emotionally intensive work, close patient relationships, and engagement with individuals and families across complex life transitions. These roles involve navigating both clinical and social dimensions of care, which may amplify the emotional demands placed on providers. At the same time, this work may foster a sense of purpose and connection that contributes to resilience. Resilience in this context may include working within complex systems, recognizing broader contributors to poor perinatal outcomes, and engaging in advocacy efforts to improve care delivery and outcomes.27,28
Practice setting may also play an important role in shaping burnout experiences. Differences between hospital-based and private practice environments, including patient complexity, workload, resource availability, and organizational support, may influence both stress exposure and coping capacity among clinicians. 29 Although practice setting was included as a covariate in this study, future research should more directly examine how these contextual factors interact with ACE exposure to better understand variation in burnout risk.
These findings have important implications for workforce development. Trauma-informed approaches that acknowledge the prevalence of early adversity among clinicians, alongside strategies that support resilience and coping, may be particularly beneficial in high-stress clinical environments where both individual and organizational factors contribute to burnout. 30 Supporting this workforce requires individual-level approaches and organizational strategies that address structural contributors to burnout. 30
Future research should continue to explore mechanisms underlying these associations, including the role of positive childhood experiences (PCEs), which capture supportive relationships and environments during childhood and have been associated with improved adult health outcomes.31,32 Additional work should examine ACE type, frequency, and severity, as well as clinician characteristics such as parental status, prior therapy or treatment, and first-generation professional status. Future studies could also explore occupational outcomes, including turnover intention, leadership roles, career advancement, and workplace factors such as workload, staffing, organizational support, work-family conflict, schedule flexibility, and access to mental health resources. 33
Limitations
This study has several limitations. First, the recruitment materials were labeled as a study on burnout. This could have introduced bias because participants experiencing burnout or interested in burnout may have been more likely to participate than those who were not. Additionally, the recruitment team attempted to contact several MCH associations across different parts of the country and community, but some organizations did not respond or declined to disseminate the survey, potentially contributing to non-response and selection bias.
There are multiple ways to operationalize both ACEs and burnout, and our categorizations may not fully capture the nuances of these constructs. Although the MBI-HHS is an industry standard, the 10-item ACE questionnaire does not include culturally relevant or structural adversities such as racism, immigration stress, community violence, or environmental disasters.
The cross-sectional design also prevents causal interpretation; associations cannot determine whether early adversity leads to burnout or whether burnout contributes to recall or reporting of ACEs.
Finally, resilience was not measured in this study, limiting interpretation of why participants with 1 to 2 ACEs demonstrated lower burnout compared to those with no ACEs. Future research should include validated resilience measures, like PCEs to clarify potential mediating effects.
Conclusion
This study demonstrates that a substantial proportion of the MCH workforce reports ACE exposure, with nearly one-third reporting 4 or more ACEs. These findings suggest that early life adversity may be a meaningful contributor to burnout within this workforce. Participants with 4 or more ACEs showed significantly higher emotional exhaustion and lower personal accomplishment, while those with 1 or 2 ACEs demonstrated lower emotional exhaustion and depersonalization compared to those with no ACEs. Further research is needed to better understand the underlying mechanisms behind adaptive coping or resilience patterns among those with moderate adversity.
Addressing burnout in the MCH workforce is essential to improving provider well-being, retention, and ultimately maternal and child health outcomes. Future interventions should incorporate trauma-informed and resilience-building approaches that recognize the varied experiences of providers. Supporting the workforce requires both organizational policies that address structural contributors to burnout and targeted supports for clinicians with high ACE burden. Future research should explore possibly significant causal pathways including validated resilience measures, PCEs and examine structural contributors to burnout to guide effective workforce policies.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319261442680 – Supplemental material for Burnout and Adverse Childhood Experiences in the Maternal and Child Health Workforce
Supplemental material, sj-docx-1-jpc-10.1177_21501319261442680 for Burnout and Adverse Childhood Experiences in the Maternal and Child Health Workforce by Katherine Cox, Michelle Clausen and Amita Vyas in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
Thank you to all those that participated in the survey.
Ethical Considerations
The George Washington Institutional Review Board reviewed and approved all procedures for this study, including the protection of human subjects.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by the Maternal Child Health Bureau and the Health Resources and Services Administration (HRSA) of the U.S. Department of Health and Human Services (HHS) under grant number T76MC35370 Maternal and Child Health Public Health Training Program. This information or content and conclusions are those of the author and should not be construed as the official position or policy of, nor should any endorsements be inferred by HRSA, HHS, or the U.S. Government.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated or analyzed during this study are available from the corresponding author* on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.