
Abstract
Background:
Individuals living in poverty often visit primary healthcare clinics for health problems stemming from unmet legal needs. We examined the impact of a medical-legal partnership on improving the social determinants of health (SDoH), health-related quality of life, and perceived health status of attendees of a Legal Clinic Program (LCP).
Methods:
This was a pre-post program evaluation of a weekly LCP established within an urban primary healthcare clinic to provide free legal consultation. Patients aged 18 years or older were either approached or referred to complete a screening tool to identify potential legal needs. Those identified with potential legal needs were offered an appointment with LCP lawyers who provided legal counsel, referrals, and services. For those who attended the LCP, changes in SDoH and health indicators were collected via a self-reported survey 6 months after they attended the LCP and compared to their baseline scores using paired t-tests, McNemar’s test for paired proportions, and the Wilcoxon Signed Rank Test for related samples.
Results:
During the 6-month evaluation period, 31 participants attended the LCP and completed both the baseline and 6-month surveys; 67.8% were female, 64.5% were white, 90.3% were not working full-time, and 61.3% had a household income of $700 to 1800 per month. At follow-up, 25.8% were receiving at least 1 new benefit and there was a statistically significant reduction in food insecurity (35.5% vs 9.7%, P < .05). Also, perceived health status using the visual analog scale (ranges from 0 to 100) significantly improved from 42.5 points (SD = 25.3) at baseline to 56.6 points (SD = 19.6) after 6 months (P < .05).
Conclusions:
The LCP has the potential to improve the health and wellbeing of patients in primary healthcare clinics by addressing unmet legal needs and SDoH.
Keywords
Introduction
Social determinants of health (SDoH) are social and economic factors and conditions that influence health outcomes. It is estimated that 30% to 55% of health outcomes are attributable to SDoH. 1 In fact, SDoH such as stable housing, food insecurity, unemployment or job insecurity, and immigrant or refugee status are all factors that collectively have a more significant impact on health and health outcomes than healthcare and lifestyle choices.1,2 Furthermore, people living in poverty are more likely to report multiple concurrent SDoH, such as unemployment, tenuous housing, and food insecurity. 2 Previous research has found that some of these challenges (eg, discrimination in accessing housing) could be improved through the support of legal services, but populations experiencing difficulties due to SDoH frequently do not have the financial means to access legal services.3 -5
In 2021, 10.6% of the Canadian population was living in poverty according to the Statistics Canada Low Income Measure (LIM). 6 LIM is an international standard for measuring poverty based on household income, using a threshold of 50% of median household after-tax income, adjusted for household size; this is also referred to as LIM-50. 7 People living in poverty have higher burdens of health problems such as mental illnesses, chronic diseases, and multiple comorbidities, and have greater difficulties in navigating and paying for health and legal services.2,4,5,8 Unmet legal needs are an SDoH that jeopardise basic human needs compounding poor health and health inequities.4,5,8 Patients living in poverty often consult their primary care providers for health issues arising from unmet legal needs.9,10 Primary care professionals recognize the association between poverty, health, and legal needs but may not be equipped to provide services other than healthcare.10,11 Legal representation in healthcare settings can facilitate access to legal services to address fundamental legal needs that affect health and SDoH. 11
Medical-legal partnerships are collaborations of health professionals and lawyers that embed legal aid for low-income, vulnerable populations into healthcare settings.9 -11 Through legal screening and intervention, legal clinics assist participants in being able to access housing, employment, and income assistance benefits that may mitigate the instigators of poverty. 11 For example, preventing eviction from housing, addressing unsafe housing conditions, seeking court action to gain spousal support, appealing rejected disability income benefit applications, and settling other court actions. The HeLP children study found that a medical-legal partnership was able to successfully assist 89% of patients referred to the program with legal issues, primarily related to income and housing. 12 However, a scoping review found that medical-legal partnerships have not been extensively implemented and evaluated in the Canadian context. 9
An innovative Legal Clinic Program (LCP) was established as a weekly clinic set in a primary care medical clinic in partnership between a family health team (FHT), Hamilton Community Legal Clinic (HCLC), and Legal Aid Ontario (LAO) to provide primary care and free legal consultations to low-income, vulnerable populations. 13 This paper explores the impact of the LCP, specifically focused on those living in poverty, through the following research questions:
RQ1: What is the effectiveness of the LCP on SDoH-related factors (eg, income benefits, job employment, and food security)?
RQ2: What is the effectiveness of the LCP on improving health-related quality of life (HRQoL) and self-reported health status?
Methods
Study Design
This program evaluation used a longitudinal pre-post intervention research design with participants who had legal issues and attended the LCP between April and October 2016. Participants self-completed surveys at baseline during the initial screening for legal issues and then repeated the same surveys 6 months later.
Setting and Participants
The LCP took place in a primary care health clinic in Hamilton, Ontario, Canada within a FHT. Participants were 18 years old and older and were approached in the primary care health clinic waiting room or referred by their primary care doctor, or other healthcare staff within the clinic, to participate. Speaking English was not an inclusion criterion, but the participant did need to bring a translator with them (eg, friend or family member) if required. Participation was voluntary and did not impact the medical care received. All participants provided written informed consent. Ethical approval was obtained from the Hamilton Integrated Research Ethics Board (Project #20161085).
Intervention: The Legal Health Check-Up Clinic
The LCP was a medical-legal partnership with the FHT and 2 law firms that had complementary expertise: HCLC and LAO. The HCLC had expertise in housing, employment, social assistance, and human rights issues. The LAO had expertise in criminal, family, refugee, and estate law. Situated in the FHT clinical space, the LCP provided free legal aid services through a weekly clinic with a lawyer; the 2 law firms alternated on a weekly basis. Participants completed the Legal Health Check-Up survey to determine potential legal issues. 14 Participants who identified a legal issue were offered a 30-min appointment at the LCP with a lawyer who had the appropriate expertise. If the participant consented, information from their Legal Health Check-Up survey and legal appointment were added to their electronic medical record. In addition, if the participant agreed, the legal team was permitted to communicate with the medical team to arrange necessary services, such as coordinating a physical examination to send to the Workplace Safety and Insurance Board.
Following the initial 30-min appointment there were multiple pathways that could be taken. First, all participants would be directed to resources or provided education related to their concerns that may help address their legal needs. For participants who needed more legal assistance, the options would depend on their income level. Low-income participants could qualify for LAO or HCLC services, whereas participants with higher income could be referred to a private lawyer or one of the lawyers staffing the LCP could elect to take on the participant’s case. Participants were also able to come back to the LCP in the medical clinic if they wanted further help or had a new legal need.
Data Collection and Measures
The data was collected from participants self-completing the Legal Health Check-Up survey and a study-specific survey at the time of recruitment while in the clinic, and then repeating both surveys after 6 months using an online survey platform from home.
Legal Health Check-up Survey was a pre-existing questionnaire used to screen for legal issues in 6 categories, including income, housing, employment, education, health, and family/community supports. 14 Some examples of these potential legal issues are workplace discrimination, housing eviction, and challenges in accessing financial benefits.
The study-specific survey asked participants to provide their demographics (age, gender, marital status, household composition, educational status, income level, citizenship status, and ethnicity), health-related quality of life (EQ-5D-3L), and the visual analog scale of perceived health status. 15 It also had food, housing, and income insecurity indicators validated for use in healthcare settings that were not already captured in the Legal Health Check-Up survey.16,17 For income insecurity, participants were asked, “Do you have difficulty making ends meet at the end of the month?” with the response options of “yes” and “no.” 16 Similarly, for housing insecurity, they were asked, “Do you ever worry about losing your place to live?” and for food security, “In the past month, was there any day when you or anyone in your family went hungry because you did not have enough money for food?” with the response options of “yes” and “no.”16,17
LIM-50: Participant status of being below the LIM-50 threshold was determined by comparing their annual household income (projected from the self-reported monthly household income) and household size to the Canadian LIM-50 income cutoffs by household size for the study year. 18
Data Analysis
Descriptive analyses were used to describe participant characteristics and the outcome variables. Paired t-tests and McNemar’s test for paired proportions were used to evaluate changes in each SDoH-related factor for LCP attendees, comparing their scores after 6 months to their own baseline scores. The Wilcoxon Signed Rank Test for related samples was used to assess changes in the number of benefits the participant needed help with at 6 months compared to their own baseline. All statistical analyses were conducted on IBM SPSS version 24.
Results
Sociodemographic Characteristics
The demographic characteristics of participants who attended the LCP and completed both the baseline and follow-up survey (n = 31) are listed in Table 1. A large proportion of these participants (83.9%, n = 26) were found to be below the LIM-50 cut-off, meaning they were experiencing poverty.
Sociodemographic Characteristics of LCP Participants Who Completed Both the Baseline and 6-Month Follow-Up Surveys.
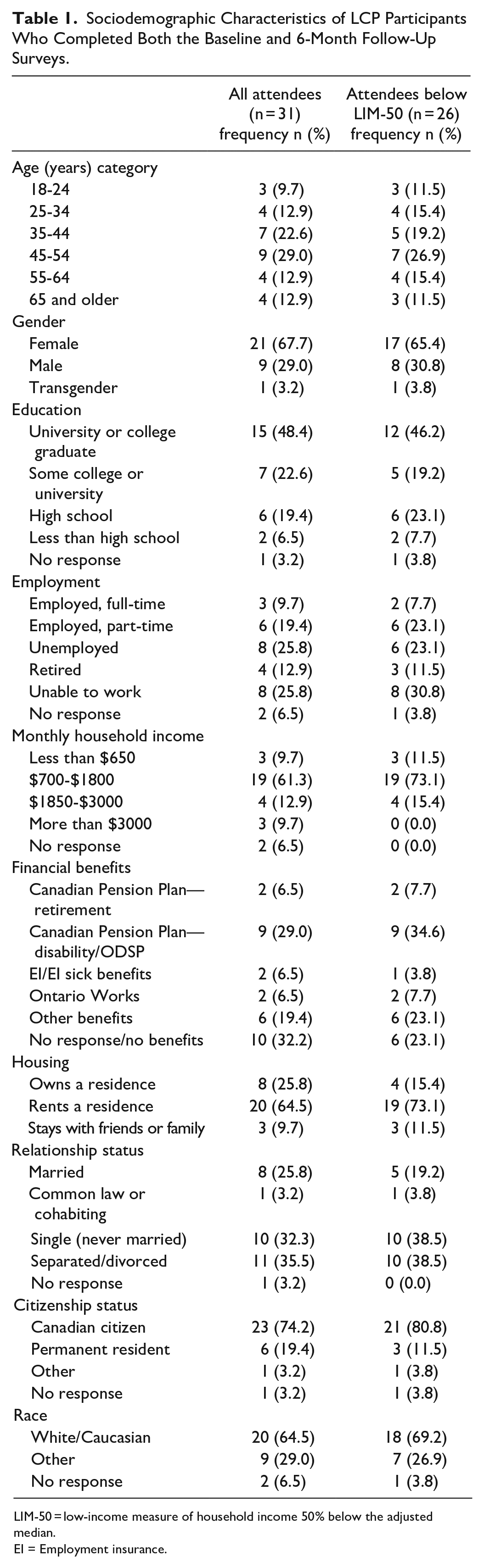
LIM-50 = low-income measure of household income 50% below the adjusted median.
EI = Employment insurance.
For the full sample, the majority of participants were female (67.7%), white (64.5%) between the ages of 35 to 54 years old (51.6%), were not working full-time (90.3%) and had a monthly income between $700 to $1800 (61.3%), and the most common category of education was college/university graduate (48.4%). While the participants below LIM-50 were similar, it was noted that they were more frequently living alone (single/separated/divorced, 77.0% vs 67.8%) and renting their residence (73.1% vs 64.5%).
Income, Food, and Housing Insecurity
At follow-up, 8 participants (25.8%) reported receiving at least 1 new benefit in the last 6 months, and for the subgroup under LIM-50, 6 participants (23.1%) reported receiving a new benefit during this period. Changes in income insecurity, food insecurity, and housing insecurity measures were evaluated and reported in Table 2. While income insecurity did not show a statistically significant improvement among attendees, the frequencies demonstrate that some participants did become aware of additional benefits that they could seek help in accessing. In addition, there was a significant reduction in food insecurity among participants (P = .005) with the proportion of participants reporting going hungry in the last month decreasing from 35.5% to 9.7%.
Change in Income, Food, and Housing Insecurity After 6 -months Compared to Baseline.
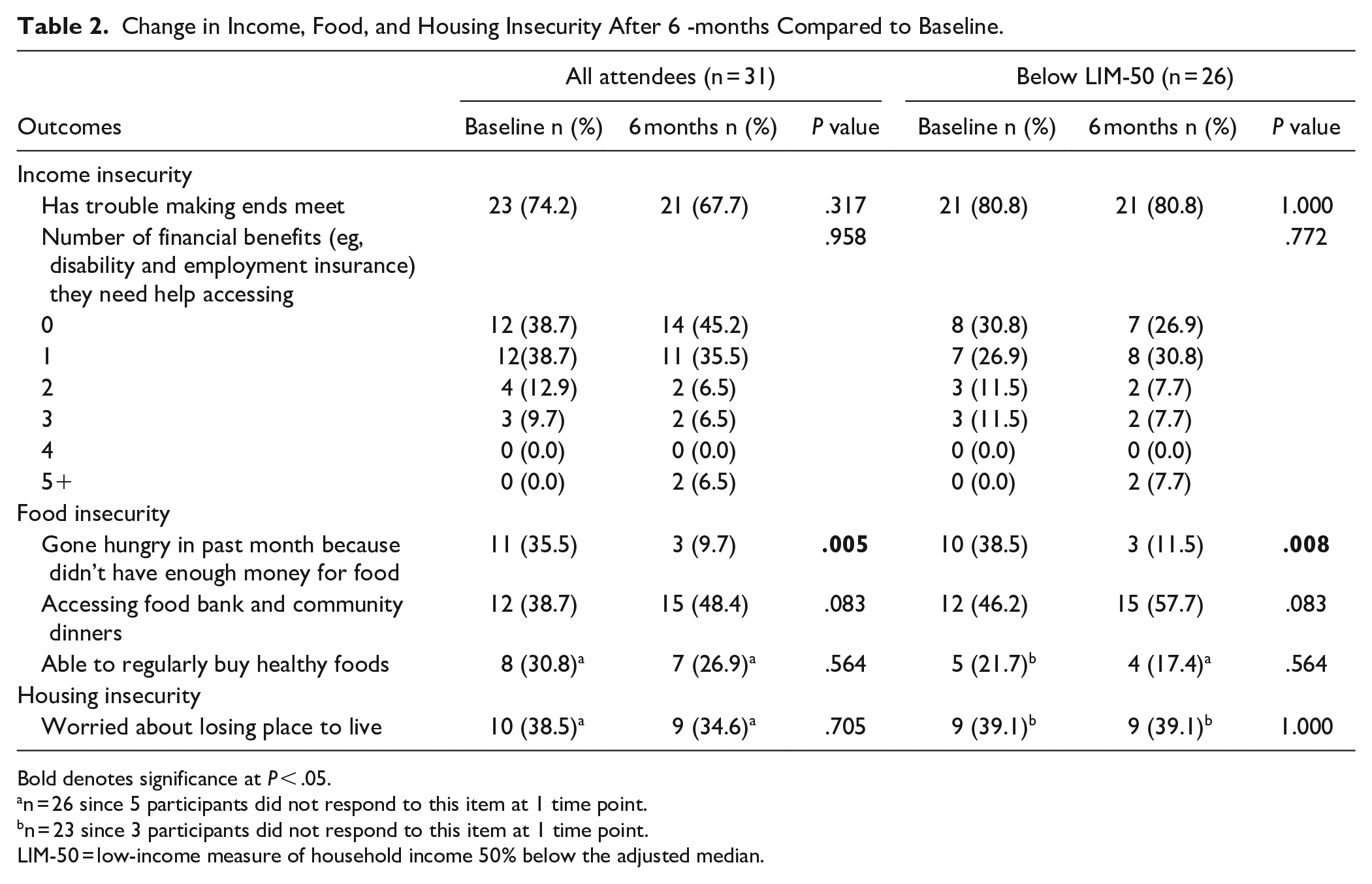
Bold denotes significance at P < .05.
n = 26 since 5 participants did not respond to this item at 1 time point.
n = 23 since 3 participants did not respond to this item at 1 time point.
LIM-50 = low-income measure of household income 50% below the adjusted median.
Health-Related Quality of Life
There were no statistically significant changes in any of the health-related related quality of life domains from the EQ5D observed in this study (see Table 3), but it was noted that there were some small improvements in those below LIM-50 in mobility (66.7% vs 58.3%) and being able to perform usual activities (83.3% vs 75.0%). Please see Table 3.
Change in Health-Related Quality of Life and Self-Reported Health Status After 6 Months Compared to Baseline.
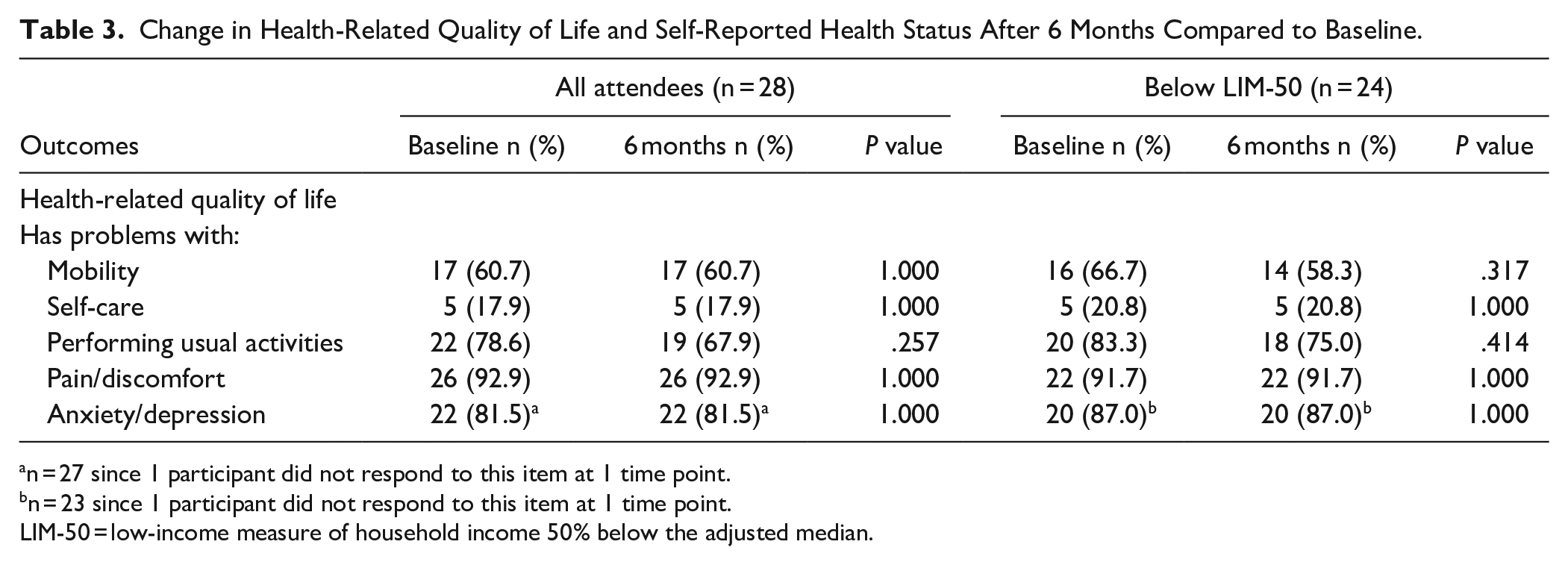
n = 27 since 1 participant did not respond to this item at 1 time point.
n = 23 since 1 participant did not respond to this item at 1 time point.
LIM-50 = low-income measure of household income 50% below the adjusted median.
A significant change in perceived health status on a visual analog scale of 0 to 100 was observed in all attendees (baseline score = 42.5, SD = 25.3 and 6-month score = 56.6, SD = 19.6; P = .012) and an even larger difference in those below LIM-50 (baseline score = 37.9, SD = 23.1 and 6-month score = 54.4, SD = 19.0; P = .013). This represents a relative improvement of 33.2% and 43.5%, respectively. Please see Figure 1.

Change in perceived health status mean score on Visual Analog Scale between baseline and 6 months for all attendees and for the subgroup below LIM-50.
Discussion
This study found a 33% improvement in perceived overall health for all LCP attendees, a 44% improvement for attendees experiencing poverty and a significant reduction in food insecurity. This demonstrates the potential beneficial health impacts on perceived health of providing legal services within a primary care clinic. Over 80% of participants who needed legal help and attended the LCP were found to be experiencing poverty (below LIM-50), highlighting the need for legal services that are accessible to low-income patients. Previous research has found that family doctors who have in-house legal services feel more comfortable asking patients about SDoH when they know there is this resource to which they can refer the patient. 19 For vulnerable patients, having this type of service within their primary care setting may help address SDoH in a trusted environment and this study demonstrated that it may subsequently lead to better perceived health status. 11
One quarter of the LCP attendees reported accessing at least 1 new benefit after 6 months (eg, disability benefits and childcare) and 1 quarter were no longer experiencing food insecurity, indicating that the program was achieving success in supporting patients in acquiring these resources. When looking at the change in number of benefits each participant reported needing help accessing, there was no statistically significant improvement, which was unexpected. When taking a more granular look at the data, it became apparent that some participants reported needing help accessing more benefits at 6 months than at baseline, suggesting that they became aware of additional benefits for which they qualified. Consequently, this particular outcome is challenging to interpret statistically as a single value since changes in both directions can be an indicator of success. However, with this more nuanced approach, it was found that the LCP had an impact both on helping participants successfully access benefits and in becoming more aware of additional benefits that they may be eligible to receive.
Although perceived health status did improve significantly, many measures in this study showed no change over 6 months. One reason may be that some legal issues can be slow to resolve (eg, appealing disability benefit decisions). 20 However, even without a change in many measures, perceived health status improved and this may be because previous research has found that medical-legal partnerships can improve patient perceived stress and well-being. 21 Once the participants in this study received legal advice, they may have felt that changes were in motion or had a sense of hope, improving their perception of well-being. This potential mechanism would need to be further explored through a future qualitative study.
A major strength of this study was its whole-person approach, addressing many SDoH simultaneously with the same intervention (income, employment, housing, family situations, food insecurity, etc.). Previous interventions in primary care settings have typically been more narrowly focused, such as targeting those who are unhoused, household utilities, and families with children.9,12,22 -24 Another strength was the pragmatic nature of the study, evaluating the LCP program as implemented in a real-world setting with minimal burden placed on clinic staff and not restricting who was permitted to access the program (eg, low-income parents) or guiding the type of advice or resources provided. The program could therefore be sustained in the same manner it was implemented during the program evaluation period and be available to all patients.
There were some limitations with this study as well. There was a small sample size and there may be some self-selection bias in the patients who opted to attend the LCP and those who opted to complete the surveys. Also, the data was self-reported, which could be affected by recall or social desirability biases, especially for sensitive topics like household income that individuals may not want to disclose. Previous reviews on medical-legal partnerships have noted the challenges in evaluating these types of interventions due to the topic and complexity.9,10 In addition, the program evaluation was only 6 months, which is a short timeframe for some legal issues, and the true impact of the intervention may not be captured (eg, submitting an application for benefits within the study period may not result in acquiring the new benefit for many months).
Conclusions
The LCP was successful in improving food insecurity, assisting patients with accessing benefits, and improving overall perceived health. Legal-medical partnerships may be a more comprehensive approach to addressing patient SDoH, especially for those experiencing poverty. Both patients and family physicians may benefit from this type of program being expanded to other primary care settings.
Footnotes
Author Contributions
GA, JM, and DE conceived of the study. GA, DE, BD, HT, and JM initiated the study design and GA, DE, BD, HT, JM, and SC contributed to implementation. GA and MP provided epidemiological expertise and MP and BD conducted the statistical analysis. GA and MP drafted the manuscript and all authors contributed to and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Local Poverty Reduction Fund through the Ontario Trillium Foundation (Project No. PR10028). HCLC and LAO provided in-kind legal staffing coverage for the Legal Health Clinic during the time period of the study.
Ethical Approval and Consent to Participate
Ethical approval was provided by the Hamilton Integrated Research Ethics Board (Project #20161085) and all participants provided written consent.