
Abstract
Background:
Primary care providers (PCPs) have a responsibility to care for patients with refugee backgrounds, often treating unfamiliar diseases and addressing culturally rooted concerns for which the provider has limited knowledge. Despite mandatory cross-cultural training requirements for medical school accreditation, studies among healthcare providers have reported a lack of training and feeling unprepared in caring for immigrant and refugee populations. Our aim was to determine the experiences, attitudes, preparedness, skills, and barriers PCPs have in caring for patients with refugee backgrounds.
Methods:
Semi-structured interviews were conducted with PCPs which were transcribed, coded, and analyzed using template analysis.
Results:
Nine PCPs were interviewed. Medical specialties included family medicine (n = 5), internal medicine (n = 2), and pediatrics (n = 2). Resulting themes highlighted the complexity of caring for patients, that on-the-job experiences were helpful in building preparedness, while training during clinical degree programs was limited, and that numerous barriers posed as challenges to providing care.
Conclusions:
Caring for patients with refugee backgrounds presents unique challenges that affect the patient-provider relationship. While PCPs find caring for patients with refugee backgrounds rewarding, they are faced with time constraints, cultural differences, and complex challenges that require interdisciplinary strategies to mitigate.
Introduction
The United Nations High Commissioner for Refugees estimated that worldwide 117.3 million persons remained forcibly displaced in 2023, including 31.6 million refugees. 1 The number of individuals displaced has steadily risen the past 12 years due to violence and war preventing safe and secure living environments for millions of people. 1 The United States plays an important role in refugee re-settlement and in 2022 the national annual refugee re-settlement ceiling was raised from 62 500 to 125 000 persons which was the highest it had been since 1993. 2
As displaced persons re-settle across the country and begin utilizing health care services, primary care providers (PCPs) may feel unprepared to treat unfamiliar diseases and address culturally based concerns for which the provider has limited knowledge.3,4 Cross-cultural training is a tool used to help mitigate disparities and improve quality of care by enhancing communication between patients and their providers. 5 Despite cross-cultural training being mandatory for medical school accreditation, 6 several studies have shown educational gaps including a lack of class time, a lack of trainee confidence in caring for immigrant and refugee populations, and poor knowledge ratings related to asylee health issues.7-9 In addition, a quarter of medical residents reported not feeling prepared to treat new immigrants and even among those with immigrant and refugee health training, only about half felt comfortable with their knowledge.5,10 Because cross-cultural training in medical education is relatively new, 7 many providers in the community may have little to no background in cross-cultural training. Additionally, barriers to providing patient centered care noted by clinicians included lack of cultural competency training, burnout, and anxiety. 11
Studies assessing the perspectives of PCPs related to their care for patients with refugee backgrounds are few, especially among providers in the United States. A systematic review conducted by Robertshaw et al 12 assessed both the challenges and facilitators related to the primary care of refugee and asylee patients. Of the 26 included studies, only 1 was based in the United States and this study assessed nurses rather than PCPs. 12 In this review, numerous challenges were identified related to language, interpreters, health literacy, unfamiliar diseases, time demands, lack of training, lack of resource awareness, and rushed appointments. 12 Health care workers in Switzerland highlight personal challenges (eg, feeling emotions related to patient stories and emotional fatigue), lack of time and communication barriers, and a need for more training (eg, transculturality and asylum procedures). 13 General practitioners in Australia noted feeling unprepared and needing more education to care for patients with refugee backgrounds who were living with chronic pain. 14
There is a need to better understand the challenges and preparedness gaps of PCPs caring for patients with refugee backgrounds. An improved understanding has the potential to inform future interventions and care processes to address the needs of PCPs and their patients. Our project aims were to explore United States based PCP experiences, attitudes, preparedness, skills, and barriers related to caring for patients with refugee backgrounds.
Methods
The study followed the consolidated criteria for reporting qualitative studies (COREQ, see Supplemental Material) guidelines. 15 All 9 interviews were conducted by author BB, a board-certified medical doctor (MD) in Family Medicine completing a health equity research fellowship at the University of Utah at the time of this project. The interviewer’s training in qualitative research was largely from coursework during their Master’s of Public Health degree program and mentorship in qualitative methods for this study by authors ST and LG.
There was no relationship established with participants prior to the study starting, other than author BB working in the same department as one of the interviewees. Participants knew that the interviewer was the principal investigator of the study along with being a physician-researcher with a background in Family Medicine and Public Health. The interviewer commenced this project with an assumption that PCPs may not have adequate training or may feel unprepared when caring for patients with refugee backgrounds. Author BB was interested in improving the quality of care delivered to patients with refugee backgrounds.
Study Design
This project was built around broad a priori categories including provider experiences, attitudes, preparedness including educational background, skills, and barriers. We took a post-positivist and constructivist approach with our research questions and we employed a deductive template analysis approach to collecting and interpreting our data, a subtype of thematic analysis.16,17
Participants were eligible if they identified as a PCP which included medical doctors and advanced practice providers, were not in a medical training program (eg, medical school, residency, and fellowship), and had treated at least 1 patient with a refugee background during their career. Participants were selected using purposive and snowball sampling methods. Recruitment efforts began by asking providers at the author’s institution for interview suggestions. Potential participants were contacted by e-mail from August to September 2023 with an introduction to the study idea and an invitation to participate. If a provider was interested, an eligibility survey and informed consent document were sent to the provider. The eligibility survey was self-completed online. 18 One-on-one interviews were conducted virtually using the Zoom video conferencing software from August to October 2023. 19
An interview guide was developed utilizing the general topics of experiences, attitudes, barriers, and educational background, skills, and preparedness related to the care of patients with refugee backgrounds. Questions were developed through literature review and discussions with subject matter experts (eg, academic faculty and patient advocacy representative). Both the audio and visual content of the interviews were recorded. Minimal field notes were taken during the interviews. Interviews lasted between 30 and 60 min. Transcripts were checked for accuracy against the audio and/or video recordings.
Study Analysis
Two coders reviewed each transcript and coding was conducted using Dedoose software. 20 The coding tree utilized is reported in Figure 1. Coded excerpts were analyzed by authors and summarized descriptions of each of the main themes were developed. Demographic data were analyzed using descriptive statistics. Sample size of this study was limited to 9 participants due to the study’s funding structure, therefore, a specific data saturation endpoint was not established.

Coding tree utilized for interview transcript data template analysis regarding primary care provider experiences, attitudes, preparedness and skills, and barriers related to caring for patients with refugee backgrounds.
Funding and Ethical Approval
This project was funded by a New Mentored Research Award through the Health Studies Fund Grant program at the University of Utah Department of Family and Preventive Medicine. This study was deemed as exempt by the University of Utah IRB, application number 00167109.
Results
A total of 18 individuals were contacted for this study and 9 providers (50%) agreed to participate. The mean age of participants was 44.9 (SD = 10.3) years, and the majority were female (n = 7, 77.8%). Work experience as a PCP ranged from 3 to 27 with an average of 13.6 years. As a PCP, about half of the providers had less than 15 years of work experience (n = 5, 55.6%) and the other half had 15 or more years of work experience (n = 4, 44.4%; Table 1).
Descriptive Characteristics of the 9 Primary Care Providers Interviewed Regarding Their Experiences, Attitudes, Preparedness and Skills, and Barriers Related to Caring for Patients With Refugee Backgrounds.
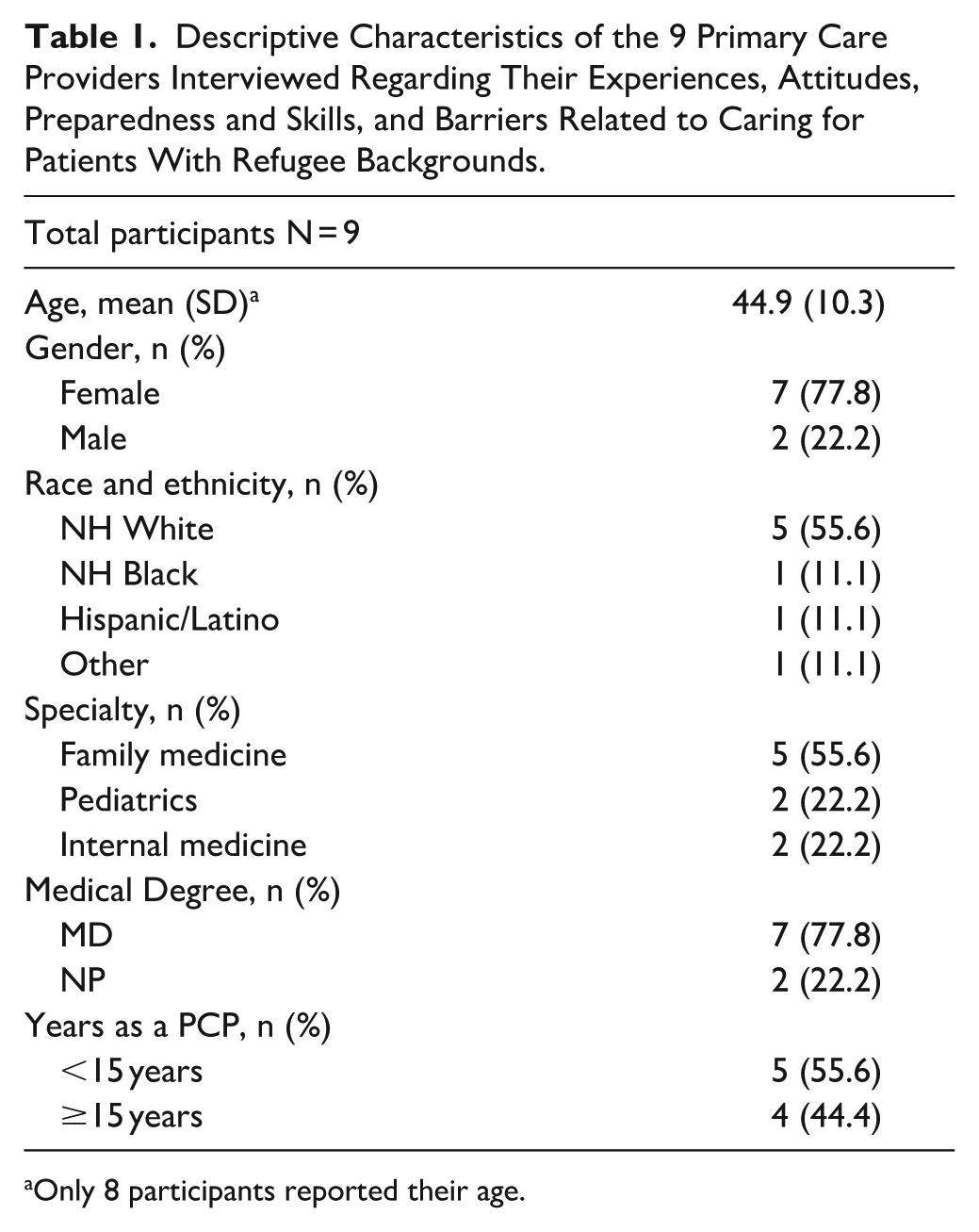
Only 8 participants reported their age.
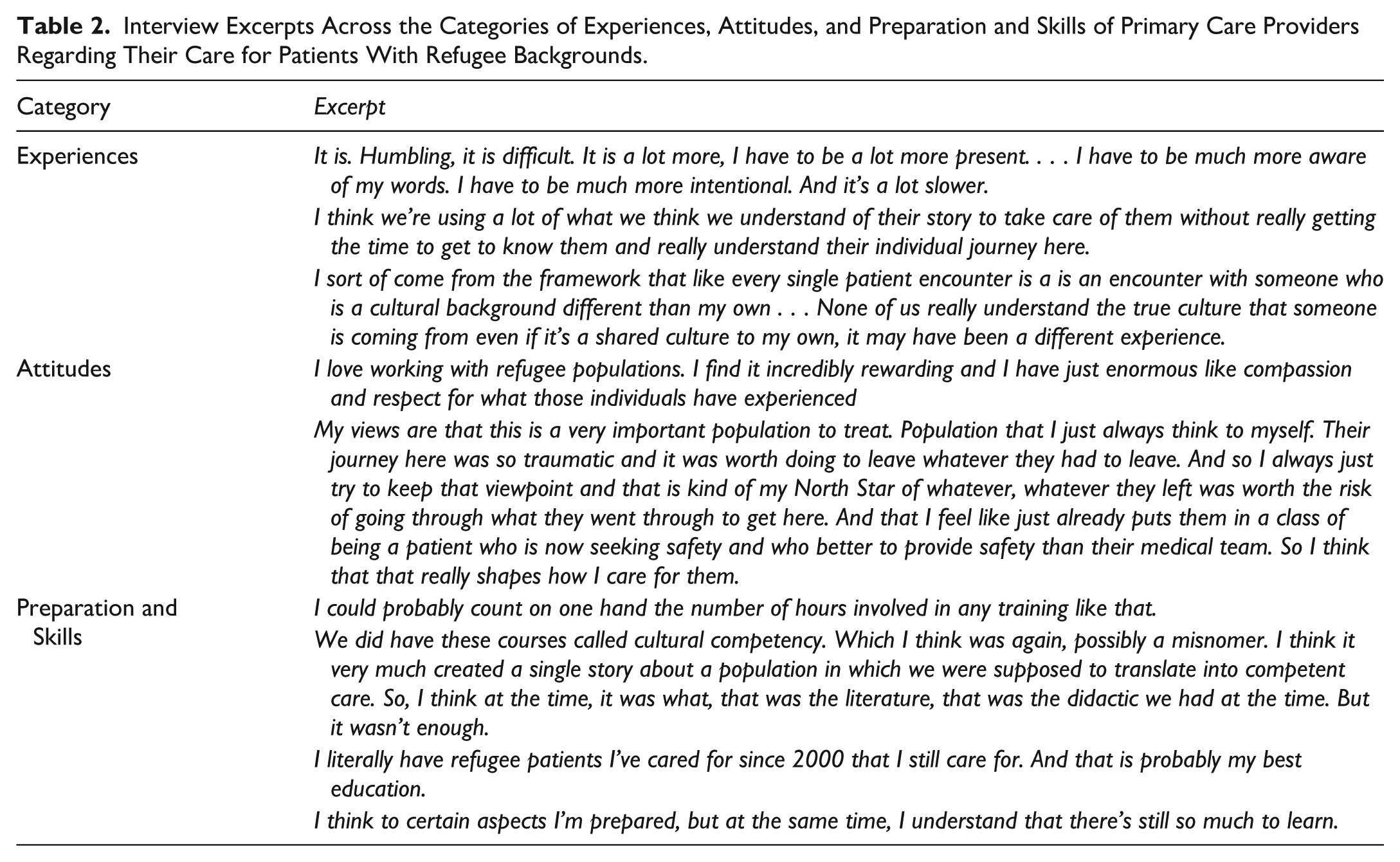
Themes that emerged from analysis of the coded excerpts were organized into 4 broad categories: (1) experiences, (2) attitudes, (3) preparation and skills, and (4) barriers. Selected interview excerpts from each of these categories can be found in Tables 2 and 3.
Interview Excerpts Across the Categories of Experiences, Attitudes, and Preparation and Skills of Primary Care Providers Regarding Their Care for Patients With Refugee Backgrounds.
Interview Excerpts Related to Barriers Experienced by Primary Care Providers Regarding Their Care for Patients With Refugee Backgrounds.

Experiences
Experiences refer to a provider’s observational and lived events while caring for patients. Some providers had extensive history in caring for patients with refugee backgrounds (eg, participating in initial refugee immigration screening evaluations), while for others, patient encounters were infrequent.
Experiences Theme 1: Caring for Patients With Refugee Backgrounds Is Complex and Communication Challenges Are at the Forefront
Providers noted that caring for patients was complex across multiple domains. Communication barriers, care coordination, treatment of less familiar medical conditions, obtaining patient medical history and records, and managing psychosocial issues contributed to this complexity. Although providers described their experience communicating with patients as positive, they also noted difficulties. These included conveying medical information (eg, patient instructions not available in the patient’s language), coordinating care logistics (eg, transportation), and navigating foreign social and cultural backgrounds (eg, styles of communication and tones conveying different meanings).
Experiences Theme 2: Providers Have Awareness of the Cultural Differences That May Play a Role in Their Experience Caring for a Patient
Navigating cultural differences was a large part of the providers’ experience. Providers were aware and understood that patients had diverse cultural and experiential backgrounds, some of which were traumatic, and that building trust was an integral part of the care process. Providers reflected on their own privileges and found it difficult to process or relate to some of their patient’s history. For example, 1 provider internally asked, “when you say you lived in a camp for 4 years, what does that mean?” Cultural differences may set different expectations for patient care, can make navigating care related to gender challenging, and small gestures like eye contact or who is allowed to speak can lead to confusion or be mis-interpreted. Furthermore, social and cultural differences may create a difference in prioritization of health-related topics that providers need to navigate (eg, having kids sleep in separate beds, breast/bottle feeding timelines). Providers expressed that working together and negotiating is needed and were aware of the dangers of stereotyping.
Attitudes
Attitudes capture the thoughts, feelings, and emotions PCPs had regarding their care for patients with refugee backgrounds. Figure 2 depicts several words providers used to describe their experiences and attitudes.

A balance of words used by primary care providers describing their experiences and attitudes caring for patients with refugee backgrounds.
Attitudes Theme: Caring for Patients Brought up Various Emotions and Attitudes for Providers
Providers expressed feeling empathy and respect when caring for patients with refugee backgrounds and acknowledged the difficulties patients had endured. They also found this work rewarding. On the other hand, frustration was a common emotion expressed and related to the challenges of the visit (eg,, getting behind schedule, communication barriers, challenges in care continuity, lack of follow-up, and a feeling of not being able to give the best possible care due to various barriers).
To help elicit further depth, providers were read a short clinical vignette during the interview regarding a patient who had fled their country and arrived in the United States 1 year ago, was accompanied by their 3 children, did not speak English, and presented with the chief complaint of pain. Providers were asked to describe their initial thoughts, concerns, and emotions about this visit. Providers expressed openness and an attitude of curiosity as they wanted to learn more about these patient’s stories. On the other hand, they described an attitude of hesitancy, felt the visit could be chaotic, difficult, and loud.
Preparation and Skills
Preparation and skills represent how prepared providers felt to care for patients along with how helpful certain life experiences were in their preparation (eg, travel and education).
Preparation and Skills Theme 1: Providers Had Variable Levels of Preparation and Skill Levels
In general, providers expressed a wide range of self-rated preparedness to care for patients with refugee backgrounds. One provider exclaimed, “I still don’t feel very prepared at all.” Several skills the providers expressed having were (1) knowing how to access clinical decision making tools (eg, infectious disease diagnosis information), (2) having skills in trauma informed care, (3) understanding the importance of trust in the provider-patient relationship, and (4) having humility and respect toward a patient’s culture. To prepare for a patient encounter, providers discussed obtaining prior health records, learning about the patient’s cultural background, learning about the patient’s immigration history, and inquiring about the interpreter (eg, the interpreter’s gender, relationship to patient, etc.).
Preparation and Skills Theme 2: Health Professional School Training on Caring for Patients With Refugee Backgrounds and Cross-Cultural Care Was Limited
Providers shared that while they may have had some training during their health profession schooling or residency, specifics were generally not memorable. One provider, when asked about receiving training related to caring for patients with refugee backgrounds, responded “I don’t think I got any.” Other providers reflected on having diverse formative clinical opportunities during their training programs. For additional education beyond formal training programs, providers engaged with lectures, conferences, webinars, modules, continuing medical education, and e-mail updates from the CDC. Having co-workers or mentors who cared for patients with refugee backgrounds was beneficial. Providers commented that their personal and/or family history of immigration, working as a nurse, military service, and personal history of travel outside the US were informative and helpful.
Preparation and Skills Theme 3: Doing the Work Is the Best Preparation
There was a prevailing message that just doing the work was the best way to learn and grow along with working in a diverse setting. In addition, helpful resources noted by providers included access to interpreter services, care managers, community health workers, and social workers. Additional care team members, like case managers, could help arrange transportation. One provider commented on having longer appointments. Some providers discussed having snacks or drinks to offer patients. Overall, preparedness was multifactorial, emerging from many elements of a provider’s background. On the job training and caring for patients with refugee backgrounds was very impactful. There was a general sense though that learning must be continuous, shaped by both clinical exposure and intentional engagement, to provide culturally sensitive and high-quality care.
Barriers
Barriers refer to the significant challenges that occur while caring for patients with refugee backgrounds.
Barriers Theme 1: Challenges Occur During the Patient Care Encounter and Include Language Barriers, Cultural Differences, Health Literacy Gaps, and Mental Health Care Delivery Barriers
Language
In circumstances when a provider and patient do not speak the same language, an interpreter is used to overcome this barrier. Providers used in-person, iPad, or telephone interpreters and these methods could be effective when they operated smoothly. However, notable difficulties were mentioned when using interpretation services including longer visits, possible discomfort for patients (eg, the interpreter and patient were from the same community), interpreters not speaking the patient’s dialect, interpreters not translating every word, and concerns for lost information through translation. Providers noted that interpreter quality was important. One provider described an example of a patient who based on an interpreter’s translation, was complaining of feeling paralyzed. The provider described further that “we lost contact with that one interpreter and then when we got hold of another one who spoke a little bit more of the dialect that this [patient] spoke, we found out that this [patient] was just experiencing vertigo. Completely changes the whole, you know, differential diagnosis.” A high level of trust was needed for all parties to work with an interpreter. As 1 provider stated, interpreters not only act as language translators, they also act as “cultural brokers.”
Cultural Differences
Patient’s view of health may differ from the provider based on their culture, religion, or spirituality. Some examples include a patient viewing being overweight as equated with health, or that spiritual problems are the root cause of health issues. Other examples included patients resisting recommendations such as dietary changes, discussing advanced directives, or resisting or refuting a mental health related diagnosis or treatment. There were varied expectations for medical care (eg, the purpose of going to a health provider, preventive care, medications, and birth control). There was a need to set expectations about treatments and their effectiveness, and cultural standards regarding gender roles also posed a barrier.
Health Literacy
Providers were concerned about patient understanding of the health system in the United States along with patient navigation of the health system. Examples of this included navigating a clinic visit (eg, how to establish care), the idea of preventive care services rather than sick care only, and obtaining and understanding how to take medication. Providers commented that they felt patients expected a tangible solution for their problem (eg, a medication), even though it might not be indicated.
Trauma and Mental Health
Providers were aware that patients may have endured traumatic experiences and recognized that patients coming to see them could be triggered or re-traumatized during their visit. Providers mentioned a connection between pain and mental health or trauma. One of the greatest barriers noted was discussing mental health concerns with patients as patients often refuted a diagnosis or treatment regarding mental health concerns. Providers were concerned that psychosocial issues were being missed and that patients often came into the clinic in crisis.
Barriers Theme 2: Challenges Occur That Are Due to System or Social Factors and Include Time Constraints, Health Care Gaps, Past Medical Record Acquisition Issues, Patient Follow-Up Barriers, Transportation Issues, and General Social Needs of Patients
Time
Providers voiced that visits with patients took about twice as long as other visits. This could be frustrating as this might have caused schedule delays or put pressure on the provider to limit the care they knew the patient needed. Patients also might have had a certain expectation about a visit length (eg, patients feeling a 40-min visit was short).
Gaps in Care and Medical Records
Providers were generally concerned that patients had gaps in their health care leading to untreated or undertreated diseases. A patient’s pre-immigration and post-immigration medical care records might not have been easily accessible, and providers might not know how to access this information. There was worry that patients had prior diagnoses that weren’t known to the provider or that if diagnosed during initial screening, the patient might not have had any follow-up. In addition, patients might have been unaware of their medical conditions. Providers also worried about the basic needs of patients being met, including clothing and food.
Clinical Access and Continuity of Care
Providers voiced concerns regarding patient follow-up challenges. Ensuring the delivery of adequate patient instructions and expectations could be difficult due to language barriers. Patients might not have understood that follow-up was needed. Making a phone call to a patient whose preferred language was not English was time consuming, and some clinical staff didn’t have the time to do this adequately. Barriers to follow-up included transportation or finding time away from work. Patients missing visits was a problem and some providers wondered if some patients ever received follow-up care. Patients also had phone number and insurance changes which complicated follow-up attempts. Additionally, electronic health systems, which could be accessed by patients, might not have been offered in the patient’s language.
Transportation
Patients faced challenges due to a lack of transportation. This might have led to not showing up for appointments, missing specialist follow-up appointments, and pose difficulties with coordinating care (eg,, ordering MRI). Some providers seemed to be able to overcome this barrier with the help of care navigators.
Social Needs of Patients
Providers had concerns about the social needs of patients including childcare, navigating a foreign system, career support, clothing, insurance, paying for healthcare, affording care, financial security, affording food, and distance from family and friends. Providers were cognizant that social factors may impact patients.
Barriers Theme 3: Challenges Occur That Are Due to Provider Knowledge Gaps
Knowledge Gaps
Providers discussed areas in which additional knowledge would be helpful in caring for patients. These areas included infectious diseases (eg, parasite, HIV, and hepatitis C), foreign medications, cultural influences on health (eg, health beliefs and health behaviors), communication, diet, foreign medical systems, finding past medical or screening records, discussing trauma, and how to encourage mental health treatments.
Discussion
This study explored PCP experiences, attitudes, preparedness, skills, and barriers related to caring for patients with refugee backgrounds. Overall, a dual nature was described in the work. It was both frustrating and rewarding. Providers were motivated to help patients with refugee backgrounds the best they could, despite the challenges and variable emotions they faced in doing so. There were varying levels of preparedness among providers, and health professions school training related to the care of patients with refugee backgrounds was limited. Practical, on-the-job type experiences proved to be effective in building provider skill and confidence in caring for patients. Commonly reported barriers included communication difficulties, gaps in medical records, time constraints, cultural misunderstandings, and limited training in refugee health care. Providers showed empathy and a strong sense of professional duty despite these difficulties, and many stressed the value of humility, developing trust, and lifelong learning.
Effective communication is a critical aspect of providing quality medical care. In a review of articles assessing experiences of global PCPs caring for patients with refugee backgrounds, communication was a common theme with challenges being the language barrier, additional time required for interpreter use, concern for inaccurate interpretation, and lack of health information in the patients’ language. 12 Our results support these findings. Our study adds that interpreters can serve as “cultural brokers” indicating that interpreters provide not only word-for-word translation but also add valuable cultural context to what patients are expressing. Interviews with patients with refugee backgrounds emphasize that adequate and open dialogue with providers is essential for setting the base of a good doctor visit. 21 Providers stressed important factors of quality interpretation beyond just language translation (eg, same dialect and comfort level for patient). Language and interpretation barriers are common among PCPs and add difficulties to a patient encounter.22,23 A study in Switzerland identified language barrier difficulties as added time to visits, uncertainty around what was understood from the visit, and reduced care quality. 22 In our study, providers were concerned that patients would not understand that they needed follow-up; or if medication was prescribed that there would be misunderstandings of how long to take the medication. Ultimately, challenges in care delivery may lead to a more superficial or bare minimum type of care. 24 To improve trust and to mitigate communication barriers, health care systems could hire cultural health navigators, a type of community health worker, to support care organization, health communication, and cultural mediation. 25 Additionally, health systems could work with providers and patients to determine best practices to identifying important metrics of interpreter quality and ensuring high quality interpretation is always accessible.
A prevailing theme from our study was the challenge surrounding mental health care for patients with refugee backgrounds. This included difficulties of patient acceptability of both diagnosis and treatment for mental health conditions. Among patients with refugee or asylee backgrounds the prevalence of both post-traumatic stress disorder and depression is estimated at 30% and for anxiety 11%. 26 Prior research describes providers feeling powerless when caring for the psychological needs of their patients, needing more skill and support. 12 In our study, providers worried that patient mental health concerns were not being fully addressed. Due to personal and cultural factors, patients might not recognize or acknowledge symptoms of mental health conditions. In addition, time constraints during visits with patients with refugee backgrounds can make it difficult to have nuanced discussions with patients to address barriers surrounding mental health problems. 27 While this may make discussing treatment options challenging, providers can use tools of trauma informed care to inform their work with patients (eg, trauma recognition and its effect on the patient, avoiding triggers, and patient respect). 28 It is also important to recognize that mental health problems may arise from patient experiences prior to immigration and also experiences adjusting to re-settlement. 29 It would be reasonable for health care systems to offer trauma informed training tools for providers who work with vulnerable patients where a history of violence and risk for mental health conditions are high. Additionally, the delivery of mental health services (eg, therapy) may be strengthened by utilizing community partnerships, expanding the role of interpreters and cultural brokers to help patients better understand mental health services, and improving mental health resources for immigration service providers. 30
In our study, providers highlighted the limited or non-existent amount of training from their medical education programs related to the care for patients with refugee backgrounds. This is highlighted by medical student survey data where it is reported that many medical students feel their education is inadequate and they don’t feel comfortable with their current knowledge of asylee related health. 9 Results from our study support that training in health professions school is limited. Providers around the world agree and further comment that this training lack can be detrimental to providing care. 12 In our study, there was a theme that the best way to develop skills and preparedness in this field was from on-the-job experience. Some providers also chose to pursue additional trainings, including webinars, modules, continuing medical education, and CDC updates. A study among medical residents demonstrated that caring for a large number of low socioeconomic patients and racial and ethnic minority patients was associated with preparedness to care for sociocultural diverse patients. 31 Along with formal cross-cultural training, on-the-job experiences in caring for patients with refugee backgrounds may prove to be an effective and efficient way to build preparedness to serve this population. Overall, our findings highlight a need for integrated and easily accessible training on caring for patients with refugee backgrounds, and ideally these trainings will cover principles of trauma-informed and cross-cultural care. 32
Strengths and Limitations
Our results have addressed a gap in the literature regarding the experiences of United States based PCPs on the provision of healthcare to patients with refugee backgrounds. Our study recruited providers with several different backgrounds (eg, specialty type and medical training type). Additionally, there was a mix of experience levels among those interviewed. The funding of this study included support for 9 interviews. Specific methods to ensure data saturation were not used due to our restricted sample size, however, 9 interviews has been hypothesized to be sufficient to achieve code saturation. 33 For further depth of study, future researchers could pursue additional data and analysis for each of the identified themes in this study. In this study, a single individual conducted all interviews, and 1 interview was with a participant in the same department as the interviewer. These factors could have introduced confirmation and affinity biases. These were mitigated by using an interview guide, 2 transcript coders, and intentionally recruiting participants with diverse backgrounds. Our study included providers from a single state although providers did work across different health systems. Additionally, our inclusion criteria were broad and included providers who may have had very limited encounters with patients with refugee backgrounds. While this may have limited some participant input in the study, these providers may have provided important insights regarding training and preparedness gaps. Future research could include larger, multi-state sampling, and triangulate provider data with patient and organizational outcomes. These findings contribute to a growing body of literature emphasizing the experiences of PCPs providing care for populations with refugee backgrounds, highlighting logistical, emotional, social, and clinical factors that influence care for patients with refugee backgrounds.
Conclusion
Health providers in primary care are faced with many challenges as they take on the role of PCP for patients with refugee backgrounds. The experiences caring for these patients may have a dual effect on providers, being both challenging and rewarding. There are numerous barriers that need to be overcome for patients with refugee backgrounds to receive equitable health care. It is prudent that we build highly networked systems that bridge the community and health system that are built on trust, cultural-compassion, and respect. Improving the connection between local social support systems and clinical workflows may help mitigate the numerous barriers described above. Structural and systemic improvements are needed to relieve some of the pressure that is placed on the shoulders of already strained providers and patients acclimating to a new healthcare model.
Supplemental Material
sj-pdf-1-jpc-10.1177_21501319261424335 – Supplemental material for A Qualitative Analysis of the Experiences, Attitudes, Preparation, and Barriers of Primary Care Providers Related to Their Care for Patients With Refugee Backgrounds
Supplemental material, sj-pdf-1-jpc-10.1177_21501319261424335 for A Qualitative Analysis of the Experiences, Attitudes, Preparation, and Barriers of Primary Care Providers Related to Their Care for Patients With Refugee Backgrounds by Benjamin H. Brown, Eliza Taylor, Lilleana Rogers, Sharon Talboys, Lisa Gren, Olanrewaju Onigbogi, Anna Gallegos, Nusrat Hossain Sheba and Kolawole Okuyemi in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
None.
Author Note
Authors Olanrewaju Onigbogi and Kolawole Okuyemi transitioned institutions while this research was being completed. Both from the University of Utah to Indiana University.
Ethical Considerations
This study was deemed as exempt by the University of Utah IRB, application number 00167109.
Consent to Participate
Providers interested in participating in this study were sent an eligibility survey, an informed consent document that outlined how to provide consent for the study, and some test survey questions (which are unrelated to the information in our manuscript). Providers who wished to consent in our study simply continued to move forward in the survey. If they did not wish to participate, they were asked to close the survey and not continue.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by the Health Studies Fund, Department of Family and Preventive Medicine, University of Utah.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data resulting from this research study is not publicly available. If there are questions or inquiries, please contact the corresponding author*.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.