
Abstract
The COVID-19 pandemic mandated a substantial switch in primary health care delivery from an in-person to a mainly remote telephone or video service. As the COVID-19 pandemic approaches its third year, limited progress appears to have been made in terms of policy development around consultation methods for the post-acute phase of the pandemic. In September 2020, the International Primary Care Respiratory Group convened a global panel of primary care clinicians – including family physicians, paediatricians, pharmacists, academics and patients – to consider the policy and health management implications of the move to remote consultations in the primary care setting. The group gave special consideration to how and how far remote consultations should be integrated into routine primary health care delivery. Remote consultations can be a useful alternative to in-person consultations in primary care not only in situations where there is a need for viral infection control but also for the routine delivery of chronic disease management. However, they may not be more time efficient for the clinician, and they can add to the workload and work-related stress for primary care practitioners if they remain the dominant consultation mode. Remote consultations are also less appropriate than in-person consultations for new disease diagnosis, dealing with multiple issues and providing complex care. Ensuring health care professionals have the appropriate skill set to effectively deliver remote consultations, administrative and/or IT support and appropriate reimbursement will be key to achieving optimal integration of remote consultations into routine clinical practice. Addressing digital access and digital literacy issues at a societal level will also be essential to ensure individuals have fair and equitable access to the internet and sufficient security for exchange of personal and health-related data.
Introduction
The global impact of COVID-19 mandated the rapid and, in many regions, substantial switch of primary health care delivery from an in-person to a mainly remote telephone or video service. 1 As the acute phase of the pandemic subsides and we enter a COVID-endemic world, health care systems will need to adjust, as the pendulum swinging between in-person and remote digital care finds a new resting place.
However, almost three years on from the emergence of COVID-19, limited progress has been made in terms of policy development around integrating remote consultation methods as a component of primary health care delivery. Understanding the issues, challenges, pitfalls, benefits and unintended consequences will enable the integration of the remote consultation model into primary health care service delivery in a way which benefits patients, primary care practitioners (PCPs) and society at large.
A remote respiratory consultation is any consultation that takes place without the health care practitioner and patient occupying the same physical space. In primary care, such consultations may take place between the patient and any member of the multidisciplinary team, including the physician, nurse, pharmacist or allied health professional. Remote consultations may also be used to facilitate interactions between primary care and hospital-based clinicians (with/without the presence of the patient) where an integrated model of care is in place. The focus of this paper is on the family medicine model of care, including the diagnosis and management of chronic conditions, which have been estimated to account for at least one-third of all family medicine consultations in developed countries. 2 A significant proportion of consultations involve multiple problems. 2
Remote consultations are not new. Telephone consultations have been used successfully for many years in remote and rural areas where distances preclude routine in-person contact. A recent systematic review of remote consultations in the primary care setting indicated they are as effective as in-person consultations. 3 In the community pharmacy setting, tele-pharmacy has the potential to increase access to medication services, especially in underserved, communities without compromising patient safety, although additional research is needed in this area.4-6 However, in today’s digital world, the potential scope for remote consultations is much greater.
Method
In September 2020, the International Primary Care Respiratory Group (IPCRG) convened a global panel of family physicians, paediatricians, pharmacists, academics and patients to explore the experience and learning of primary care clinicians, academic researchers and patients about remote respiratory health care delivery during the COVID-19 pandemic. The panel also considered the implications for health care policy if remote consultations for routine care are to be effectively integrated into the evolving model of primary health care delivery.
The review group included 17 clinicians representing Australia, Bangladesh, Brazil, Germany, Greece, Nepal, Portugal, Spain, Sweden, the Netherlands and the United Kingdom, an academic participant representing the University of Oxford Centre for Evidence-Based Medicine and three respiratory patient representatives.
Figure 1 outlines the process undertaken to generate insights by the review group. The group met three times via a virtual platform with a facilitator to discuss current approaches to the delivery of primary health care using remote consultation and to identify and reach consensus on the benefits, challenges and policy implications of remote delivery of care. Relevant literature for consideration by the group was identified via a PubMed search using terms including ‘remote consultation’, ‘video consultation’, ‘telephone consultation’ and ‘electronic consultation’, combined with the qualifying terms ‘primary care’, ‘respiratory’ and ‘COVID-19’, and was used to derive key topics for discussion. Direct quantitative information on the proportion of care delivered remotely prior to and during the COVID-19 pandemic and qualitative experience and insights into the use of remote consultations in the primary care setting were derived from a questionnaire completed by the clinician participants. Finally, participants were asked to share their personal experience of remote consultations prior to and during the COVID-19 pandemic. Research process used by the IPCRG.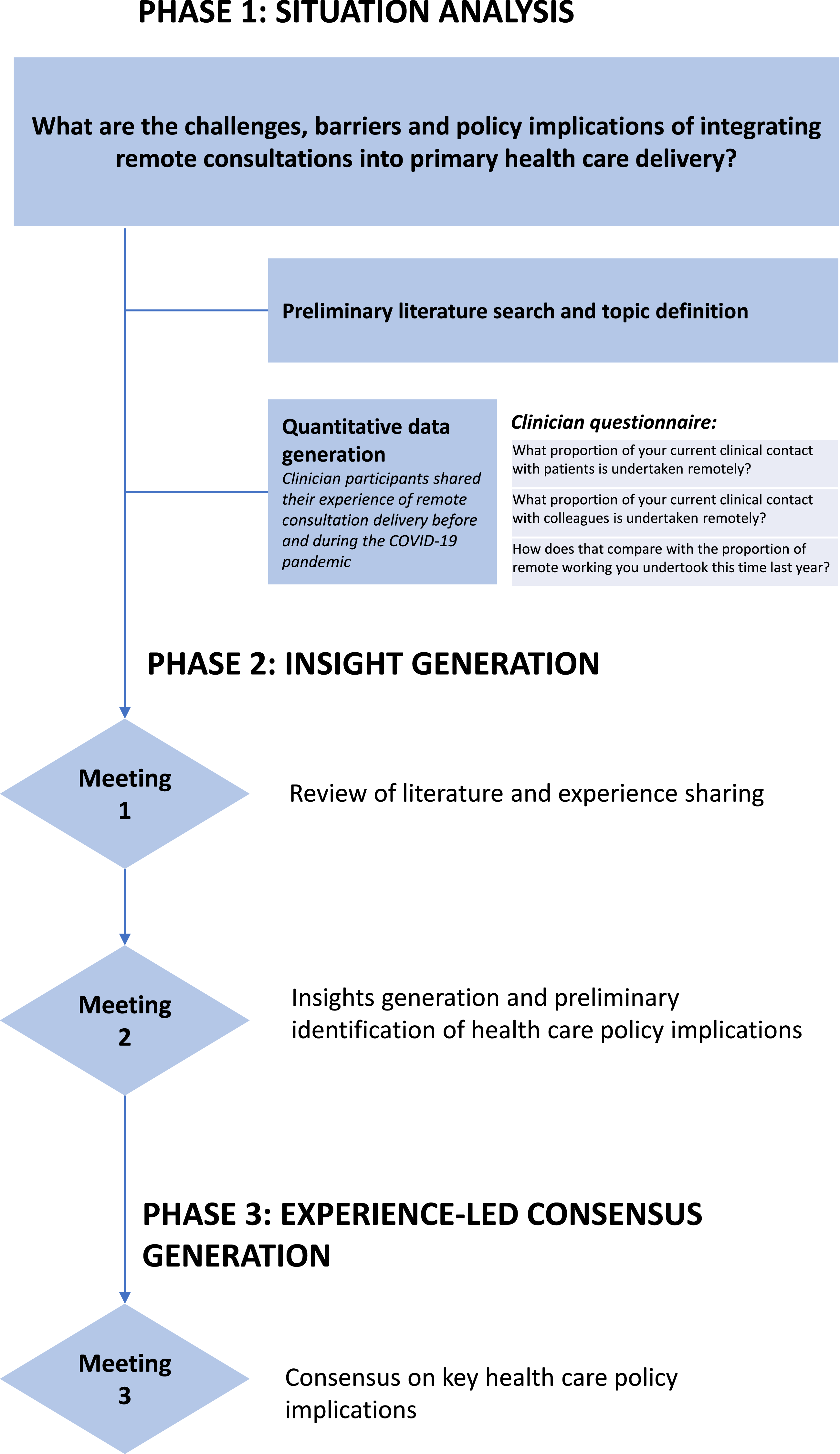
This approach enabled us to look beyond the research-driven evidence base at the tacit knowledge of the structural and process changes and the emotional currency (hope, understanding, trust, reassurance and happiness) that flows in consultations. Further details on the IPCRG and its research process are available in the online Supplement.
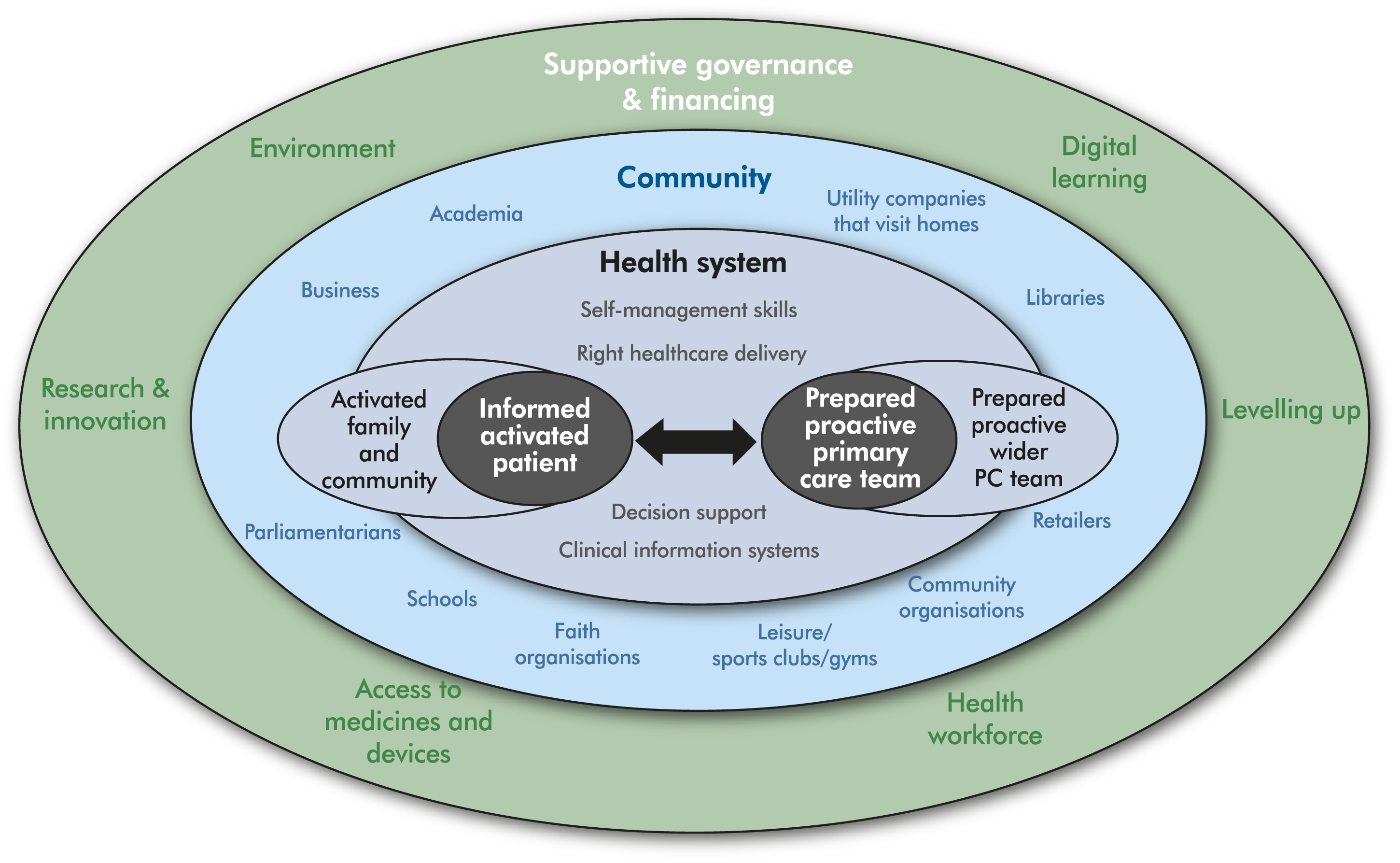
The Chronic Care Model7,8 provided a useful framework to consider the implementation of remote consultations for chronic disease management, including during acute exacerbations (Figure 2). The Chronic Care Model puts at the centre of the health system an activated informed person living with a chronic condition interacting productively and building a relationship with a prepared proactive practice team. It is essential that patient and PCP preference for consultation mode is elicited as part of relationship-building. The model defines the elements of the system that support this relationship and interaction. They include an activated community and practice team that can offer support and action, high-quality clinical information systems and decision support, a health care system that prioritizes self-management support and the potential to redesign services to better meet patient need. Expanded Chronic Care Model (adapted by S. Williams from Barr et al).
7
Let us now turn to the results of the IPCRG’s investigation.
Diagnosis, treatment, monitoring and care coordination
The balance between in-person and remote consultations for chronic disease management may change over time, reflecting the stage of the patient journey from diagnosis to regular review and personalized action planning including exacerbation management. Diagnosis of chronic disease is a core part of primary care and may require several consultations. A series of remote consultations offers the potential for convenient ‘shared diagnosis-making’ over time (e.g. for someone with suspected asthma, which is a variable condition with no single objective diagnostic test). However, remote consulting is most suitable for the delivery of routine care, including assessment and monitoring of disease control and quality of life. A range of tests and evaluations can be undertaken by patients in their own home – including temperature, symptom diaries and questionnaires – using home monitoring equipment, supported by online tutorials. App-based tools are emerging in some countries that support a range of monitoring requirements including electronic peak expiratory flow meters, blood glucose and blood pressure monitoring, and enable spirometry and other more complex evaluations usually limited to the hospital clinic setting.
Checklist to prepare for remote consultations. 10
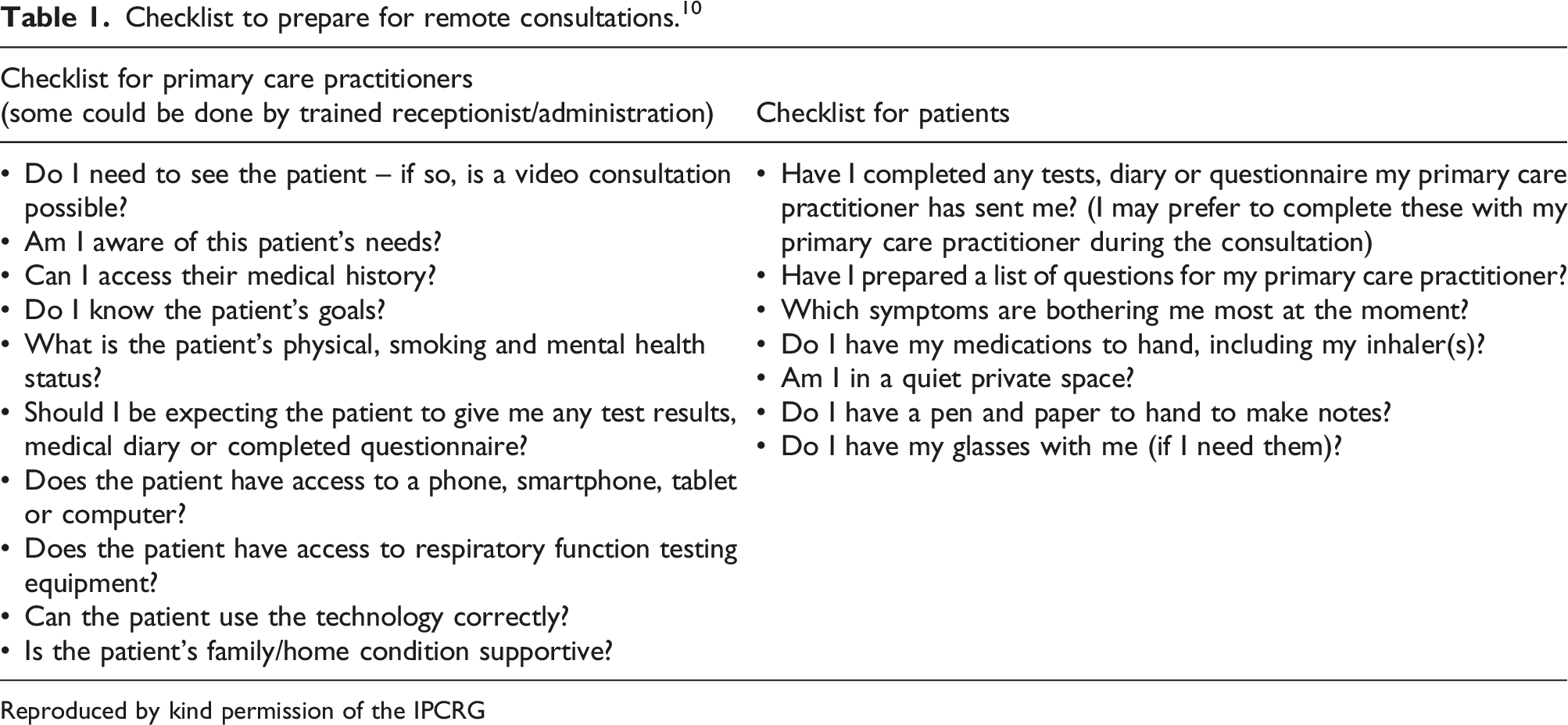
Reproduced by kind permission of the IPCRG
Remote consultations have the potential to improve the coordination of care between primary and secondary care by enabling hospital specialists to co-consult in an efficient way, including electronic record sharing. This could be particularly helpful for people with complex needs, although the potential of a widening digital divide must be closely monitored. From an organisational perspective, if reimbursement is not offered for these value-added services, then incentives work against a large scale-up. Community pharmacists have shown their potential to support medicine-use remotely, as their access to digital tools has accelerated during the COVID-19 pandemic. This allows e-prescriptions to be dispensed and delivered to people sheltering at home and to check actions – such as inhaler use – using video consultation.
Impact of the COVID-19 pandemic and opportunities arising
The rapid shift to telephone and video-consultations during the COVID-19 pandemic was driven by the need to minimize the risk of viral transmission during in-person contact.10,11 This shift appears to have changed the way some people select and prefer to access care, just as new footpaths develop over time, as people find the shortest or most easily navigated route. 12 However, if remote consultations are to become part of normal care everywhere, they need to gain at least the same status and value for patients, health care professionals and health care systems as in-person consultations.
While remote consultations are the default approach when infection control is the prime concern, other drivers should be considered to ensure that the quality of, satisfaction with and equitable access to a good quality patient–clinician interaction is maintained post-pandemic. For example, sound distortion from phones or videos can make a remote consultation extremely challenging for a patient with hearing loss, and more than one in four people over 60 years of age are affected by disabling hearing loss. 13 Solutions, and appropriate education, are needed to ensure that individuals with hearing loss (estimated to be 0.6 billion people worldwide) have access to technology that addresses their needs such as headphones, auto-captioning and sign language services to support video consultations. 14
Patient challenges and opportunities
The potential benefit for patients and their preferences and expectations must be a core consideration when deciding on consultation mode. These preferences and expectations are influenced by their cultural and organisational context, as well as personal experience, finance, levels of general health, proximity of the health care facility and availability of technology and technological literacy. Relational continuity – the relationship that builds trust, empathy and rapport between a patient and their clinician over time – is highly valued in primary care because it improves diagnosis and outcomes.15,16 A patient may have different preferences for a specialist outpatient compared to a primary care consultation and these factors may be weighted differently in these contexts. This is important as most of the literature is based on outpatient settings.
Patients’ digital access and digital literacy
For patients comfortable with and able to use internet-based services (and who have access to any necessary equipment for observations), remote video consultations may be preferred. 17 Video consultations for routine review could also have advantages for the primary care team, enabling PCPs to gain insight into the patient’s home situation. It may be possible (with consent) to involve family members living apart from the patient in the review process. Where a relationship already exists, the consultation is for a routine or single simple issue and physical observation is not needed, telephone consultations may be sufficient, more convenient and straightforward than video consultation and with fewer barriers to access.
Clinician challenges and opportunities
In-person consultation is an important way for PCPs to use all their senses to identify and assess more general changes in, for example, skin colour, gait or weight. 18 Such consultations also facilitate the raising of issues that the patient themselves may not recognize or only reveal during ‘doorknob’ moments – those moments at the end of the consultation when the patient has their hand on the doorknob ready to leave and then raises a new issue.19-21 Clinician participants felt uncertain about the validity of clinical judgements when physical examination was not possible, which contributed to the cognitive stress clinicians experienced with remote consulting. Indeed, remote consultations may be less ‘information rich’ than face-to-face consultations and so perhaps more limited in dealing with multiple or complex issues. 22 Loss of human contact, threatening their identity as a clinician, has been reported by PCPs when the ritual of the in-person contact is lost. 21 For all these reasons, remote consultations are likely to be an addition, rather than a replacement, for the holistic patient evaluation and care that is the essence of primary health care.
Consultation time constraints
Clinician participants reported that remote consultations take longer than in-person. Indeed, remote consultations may increase clinician workload if used as a wholesale substitute for in-person consultation. 23 Telephone call times may be extended by the need to explain everything verbally (as opposed to demonstrating, or providing a written list) and confirming understanding. Video consultation times may be prolonged because the people most likely to need primary care – such as the older, frail population – may have the lowest level of technological literacy and may need additional guidance on the technical aspects of the consultation. This apparent conflict with the assumed efficiency of virtual consultations in the literature and in policy statements may be due to the remote consultation case-mix which has changed during the pandemic, to include complex cases.
Upskilling
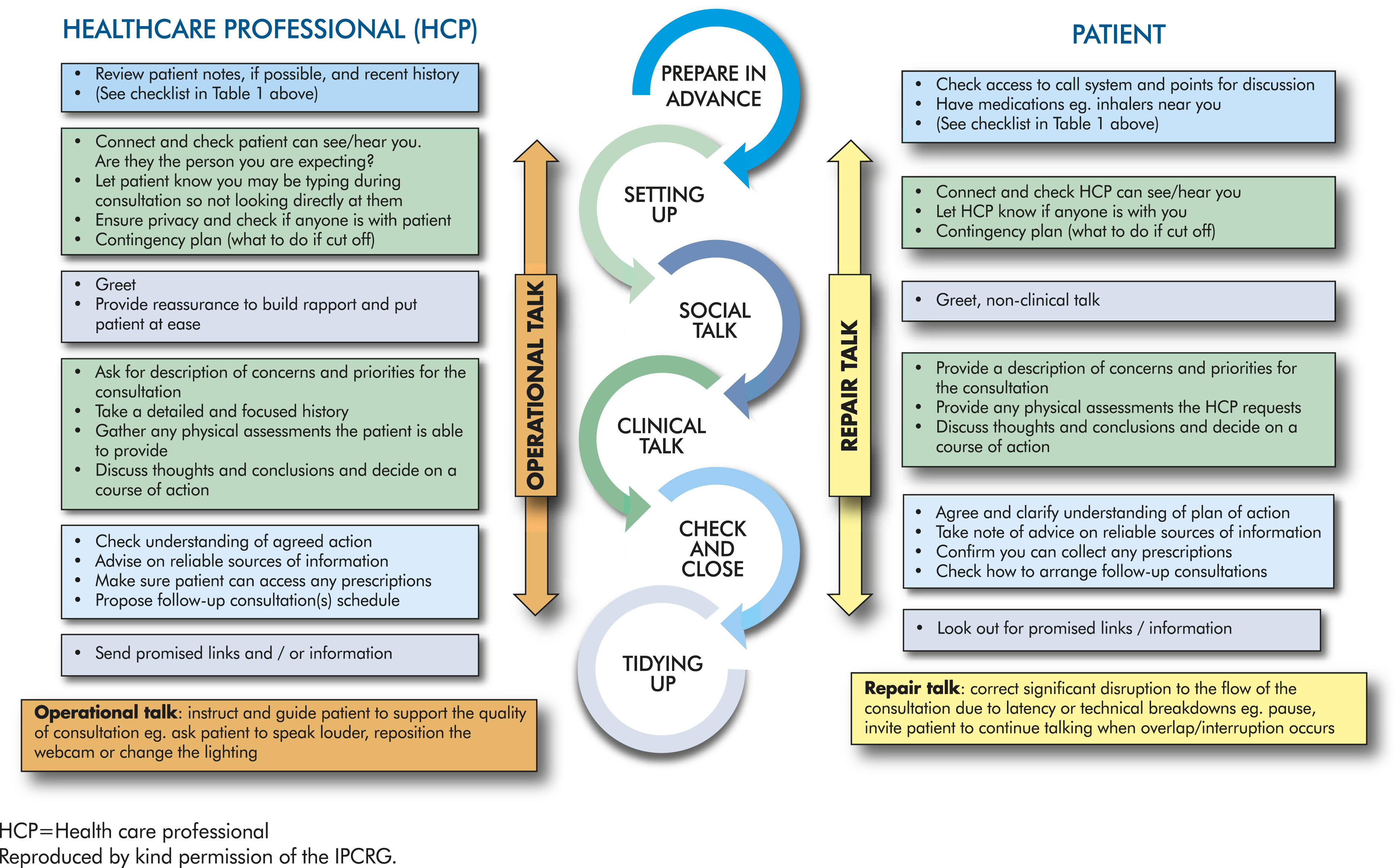
Specific clinical skills are required for remote consultation, and there are five types of ‘talk’ that clinicians need to learn and adopt to make consultations run smoothly and effectively: setting up, social, clinical, operational and repair (Figure 3).
24
PCPs may need administrative support and/or training from IT teams to ensure they are competent and confident with the consultation platform and can guide patients through any issues in real time.
9
Delivering effective respiratory remote consultations in primary care (adapted from Wherton et al).
24
Reimbursement for remote consultations
Without appropriate reimbursement to incentivize behaviour for patient benefit, remote consultations are unlikely to become a routine part of primary care delivery post-pandemic. 25 The pandemic has revealed and relied on health care activity that may not normally have been reimbursed; now leaders of health care systems need to review what is effective for patient benefit and what adds most value to their health care system. It is likely that adjustments will be required to reimbursement systems – and to invest in technology and technology support – if the systems are to be sustainable. 26
Health care system level issues and barriers
Incremental introduction of remote consulting is typically the most effective approach to successful implementation, and always in close collaboration with IT departments, 27 although the drama of the pandemic has overridden that in the short term. Long-term success will depend on strategic investment in infrastructure, training and incentives to make best use of the resources available and minimize the risk of unintended consequences (such as diminution of the patient/clinician relationship, inefficient organisations, delayed diagnosis and delayed access to specialist care).
Building infrastructure
Basic dependability should be prioritized over advanced functionality, and the technology should be perceived not as a plug-in but as integral to a wider administrative and clinical workflow. 24 Health care systems will need to develop substitutes for scheduling, flagging which method the patient will use for the consultation and if anyone else will be present, checking-in with a receptionist, waiting, getting access to test results, explaining if a clinician is running late, note-taking and recording the calls by patient and clinician and so on. 24 Systems need to highlight patient preferences, language needs and their access to home monitoring equipment. Better systems and skill-mix may reduce the time spent by PCPs but will require training of administrative teams.
Ensuring privacy and security
Remote consultations should not compromise on the ethical standards for care delivery and the protection of patient privacy and confidentiality.26,28 Some countries have mandated the digital platforms that may (or may not) be used for the delivery of remote consultations. This may be less convenient for patients, as it may not be the system they are used to or to which they have easy access. On the other hand, clinician participants reported that some of their patients seem unconcerned about privacy and choose to conduct telephone consultations from their office desk, whilst shopping or even whilst driving. This creates a dual problem for the clinician: they cannot control privacy, and they also have to contend with poor sound, disrupted connectivity, background noise and distracted patients.
Societal level issues and barriers
For some people, remote consultations have enabled the Chronic Care Model’s vision of an informed patient interacting with a prepared proactive practice team. However, of considerable concern is that remote consultations also have the potential to be disabling and to worsen health inequalities by making it more difficult for some patients to access health care.29,30 Health services cannot assume that the poorest and most vulnerable in society have access to a mobile phone for remote consultations (or to receive texted results and reminders). 30 Video consultation also requires the PCP and patient to invest in equipment to enable remote observations and incur costs associated with access to the internet, which may increase inequity. Ironically, patients from rural areas, who might particularly appreciate remote consulting to overcome distance, may be the least likely to have stable internet access.
Digital access and digital literacy are societal issues and should form part of a country-level digital strategy, ensuring individuals have fair and equitable access to the internet and sufficient security for personal and health-related data. 29
Conclusion
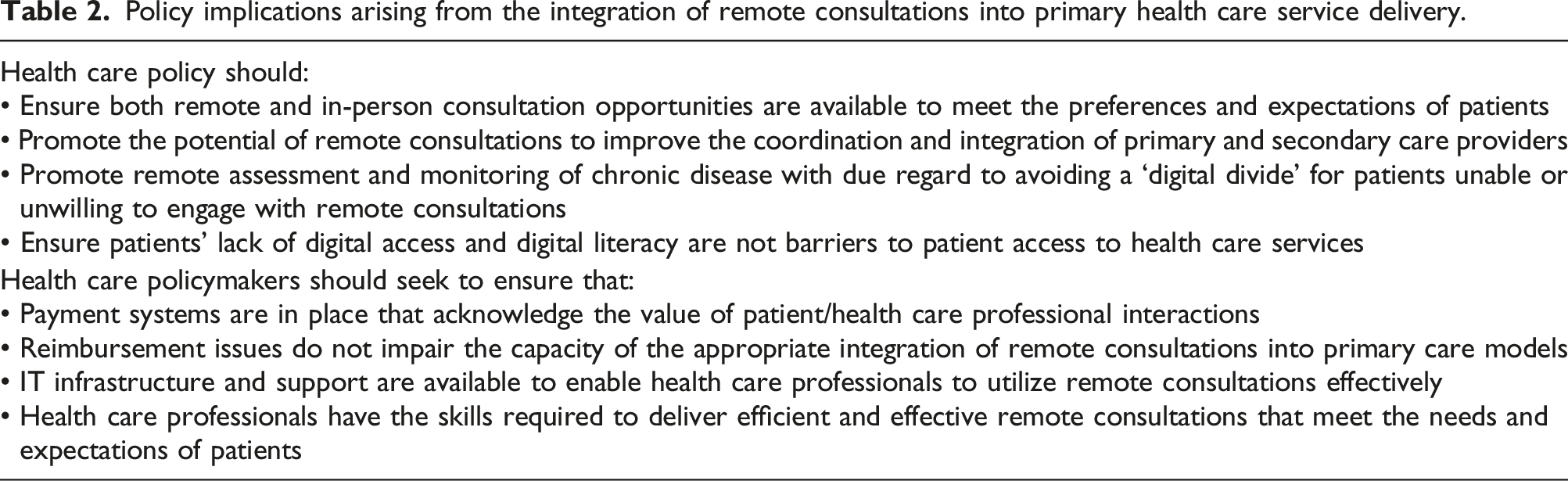
Policy implications arising from the integration of remote consultations into primary health care service delivery.
Future research should seek simple and reliable techniques to identify consultations that are most likely to work remotely. In addition, it would be valuable to explore whether remote consultations conducted by phone are sufficiently comprehensive, more equitable and more feasible than video consultations. Likewise, it is desirable to define appropriate outcome measures, which capture both patient and clinician perspectives, for the evaluation of remote consultations in primary care post-COVID. Such insights will assist in determining when and to what extent remote consultations can be effectively integrated into different health care systems.
Supplemental Material
Supplemental Material – Remote consultations in primary care across low-, middle- and high-income countries: Implications for policy and care delivery
Supplemental Material for Remote consultations in primary care across low-, middle- and high-income countries: Implications for policy and care delivery by Siân Williams, Amanda Barnard, Phil Collis, Jaime Correia de Sousa, Suraj Ghimire, Monsur Habib, Tessa Jelen, Frank Kanniess, Vince Mak, Sonia Martins, Ema Paulino, Hilary Pinnock, Miguel Roman, Hanna Sandelowsky, Ioanna Tsiligianni, Laurine van der Steen and Fabio Weber Donatelli in the Journal of Health Services Research & Policy.
Footnotes
Acknowledgements
IPCRG is a charity with organisational members in 37 countries. It is a Special Interest Group of the World Organization of Family Doctors (WONCA) Europe and an organisation in collaborative relations with WONCA World and the International Pharmaceutical Federation representing global pharmacists. We acknowledge the contribution of all our members and collaborating organisations that facilitate the activities we undertake to support the global primary health care community. The authors thank Dr Tracey Lonergan (IPCRG) for editorial support in the preparation of this manuscript.
Author’s note
The authors received honoraria via IPCRG to support their participation in two online meetings.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by an unrestricted educational grant from Boehringer Ingelheim (BI) International GmbH. There was no participation by BI in any of the meetings, emails or development of the material.
Ethics approval
Ethics approval was not required for this review article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.