
Abstract
Objective
This study aimed to estimate the impact of deprivation on the occurrence, health outcomes and health care costs of people with multiple morbidity in England.
Methods
Cohort study in the UK Clinical Practice Research Datalink, using deprivation quintile (IMD2010) at individual postcode level. Incidence and mortality from diabetes mellitus, coronary heart disease, stroke and colorectal cancer, and prevalence of depression, were used to define multidisease states. Costs of health care use were estimated for each state from a two-part model.
Results
Data were analysed for 141,535 men and 141,352 women aged ≥30 years, with 33,862 disease incidence events, and 13,933 deaths. Among incidences of single conditions, 22% were in the most deprived quintile and 19% in the least deprived; dual conditions, most deprived 26%, least deprived 16% and triple conditions, most deprived 29%, least deprived 14%. Deaths in participants without disease were distributed most deprived 22%, least deprived 19%; in participants with single conditions, most deprived 24%, least deprived 18%; dual conditions, most deprived 27%, least deprived 15%, and triple conditions, most deprived 33%, least deprived 17%. The relative rate of depression in most deprived participants with triple conditions, compared with least deprived and no disease, was 2.48 (1.74 to 3.54). Costs of health care use were associated with increasing deprivation and level of morbidity.
Conclusions
The higher incidence of disease, associated with deprivation, channels deprived populations into categories of multiple morbidity with a greater prevalence of depression, higher mortality and higher costs. This has implications for the way that resources are allocated in England’s National Health Service.
Keywords
Introduction
Socioeconomic inequalities in health status are observed in all countries. 1 In Europe, lower socioeconomic position and measures of social and material deprivation are associated with greater morbidity and mortality. 2 This includes the more frequent occurrence 3 and higher mortality 4,5 from chronic conditions, as well as a higher frequency of mental health problems including depression. 6 –8 Deprived areas also show greater use of primary care and hospital services. 9 This has been recognized in the methods used to allocate financial resources for health care in the UK. 10 In England, these currently include a weighting for disability-free life expectancy (DFLE), which is generally worse in more deprived areas, as well as age, sex and historical patterns of health care use. 11
There is a growing recognition that people with multiple long-term conditions are some of the heaviest users of health services and account for the highest health care costs. 12 Multiple morbidity is more frequent in deprived populations. 13 However, little is known about the extent of socioeconomic inequalities among patient populations with multiple morbidity. Is deprivation associated with worse outcomes and higher costs in patients with multiple morbidity? Alternatively, are outcomes and costs determined by the extent of physical morbidity, with deprivation becoming less relevant after the onset of clinical disease? These questions are important in allocating resources, and commissioning services for the important group of people with multiple long-term conditions.
This paper aims to determine how social and material deprivation are associated with health outcomes and health care use in patients with multiple morbidity. The research is part of a larger project to evaluate the cost-effectiveness of lifestyle disease prevention interventions in primary care. Results for the association of depression with multiple morbidity have been reported elsewhere. 14
Methods
Sample selection
The Clinical Practice Research Datalink (CPRD) contains records for about three million patients from approximately 600 family practices in the UK. The recording of clinical diagnoses in CPRD has high predictive value. 15 For this research, the sample was restricted to the 491 CPRD general practices in England that participate in the data linkage scheme that facilitates provision of data for deprivation quintile (Indices of Multiple Deprivation 2010 16 ) by participant postcode of residence. A sample of 300,006 participants over the age of 30 was sampled from participants registered with eligible practices contributing to the CPRD from 1 January 2005 to 30 April 2012. Deprivation scores were not available for 17,067 participants in the sample, who were excluded from the study. Participant records were analysed from later of the date of their registration at the practice or the date on which the practice began to provide research standard data into CPRD. Followup ended when participants ended their registration at the practice, reached the age of 100, died or the date of last data collection for the practice was reached. There were 52 participants who provided less than one day's record who were excluded, leaving 282,887 participants for analysis. Participants were allocated to deprivation categories using the quintiles of the index of multiple deprivation for 2010 (IMD2010) linked at participant postcode level.
Disease states
The research included four conditions known to be associated with lifestyle risks: diabetes mellitus, coronary heart disease (CHD), stroke and colorectal cancer. The conditions were selected because of their negative association with physical activity for a wider study of the effect of lifestyle interventions on disease prevention in primary care. 17 Participants with none of the conditions remained at risk. When participants developed one or more of these conditions, their person-time was allocated to one of nine disease states including those with single morbidity (diabetes only, CHD only, stroke only, colorectal cancer only), dual morbidity (diabetes and CHD, diabetes and stroke, CHD and stroke) and triple morbidity (diabetes, CHD and stroke). As the number of colorectal cancer cases was too small to subdivide into multidisease states, data were analysed for all colorectal cancer cases together as a single morbidity state. Case definitions were based on sets of Read codes that have been reported previously. 18,19 Participants’ person time in each state was further subdivided into depressed and not depressed as reported previously. 14 Prevalent depression was recorded if the participant had a diagnosis of depression in the year of interest or diagnosis of depression ever recorded and a prescription for antidepressant drugs in the year of interest. There were 40,685 participants recorded as depressed during the period 2007–2011. Data for deaths were analysed from the later of 1 January 2007 or start of each participant's record to the earlier of 31 December 2011 or the end of each participant's record.
Health care use was evaluated from participants’ electronic records in CPRD for the period 2007 to 2011. Primary care sue covered consultations at the practice, emergency consultations, home visits, out-of-hours visits and telephone consultations; hospital utilization included inpatient admissions, outpatient episodes, day cases and emergency episodes. Numbers of events per person-year were calculated for each patient. Costs of health care use were estimated using unit costs values from standard reference sources. 20 Drug prescriptions were enumerated and prescription costs were calculated by linking the Multilex drug code for each prescription to the drug cost obtained from the First DataBank Europe (FDBE) database. 21 This provided the cost of each prescribed drug for each participant.
Statistical analysis
Person years, incident events and deaths were tabulated by deprivation quintile and number of conditions. Relative rates were estimated from a Poisson regression model adjusting for age group and sex. Predictors were deprivation quintile and number of conditions. The interaction term between deprivation and number of conditions was found to be significant both for incidence (P = 0.0098) and mortality (P = 0.0009). Relative rates were therefore estimated for each quintile of deprivation and category of number of conditions, using the least deprived quintile and lowest category of morbidity for reference.
A two-part model was used to estimate costs in each state for each quintile of deprivation. At the first stage, a probit model was fitted in order to estimate the probability of costs being nonzero. At the second stage a general linear model (GLM), with a log link and gamma errors, was fitted adjusting for age group, sex, number of comorbidities, depression status and deprivation quintile. The model was used to predict mean costs for each category. Weighted mean values for predicted costs for each deprivation category were obtained by averaging across age groups weighted according to the age distribution of the European Standard Population.
Results
Data were analysed for 141,535 men and 141,352 women; 43% of men and 48% of women were 55 years and older; the more deprived quintiles tending to have a slightly younger age distribution. There were 266,981 participants aged 100 or younger who had no disease of interest at the start of their observation period. There were 33,862 incident events, with new diagnoses of one of the four conditions of interest including diabetes mellitus, CHD, stroke or colorectal cancer. Incident events resulted in a single condition state in 82% of instances, dual condition states in 16% and triple condition states in 2%. There were 13,933 deaths, including 53% in participants at risk with no study conditions, 35% in participants with a single study condition, 11% associated with dual conditions and 2% associated with triple conditions.
Incidence of single, dual and triple morbidity by deprivation quintile. Figures are frequencies except where indicated. Data analysed from start of each participants' record.
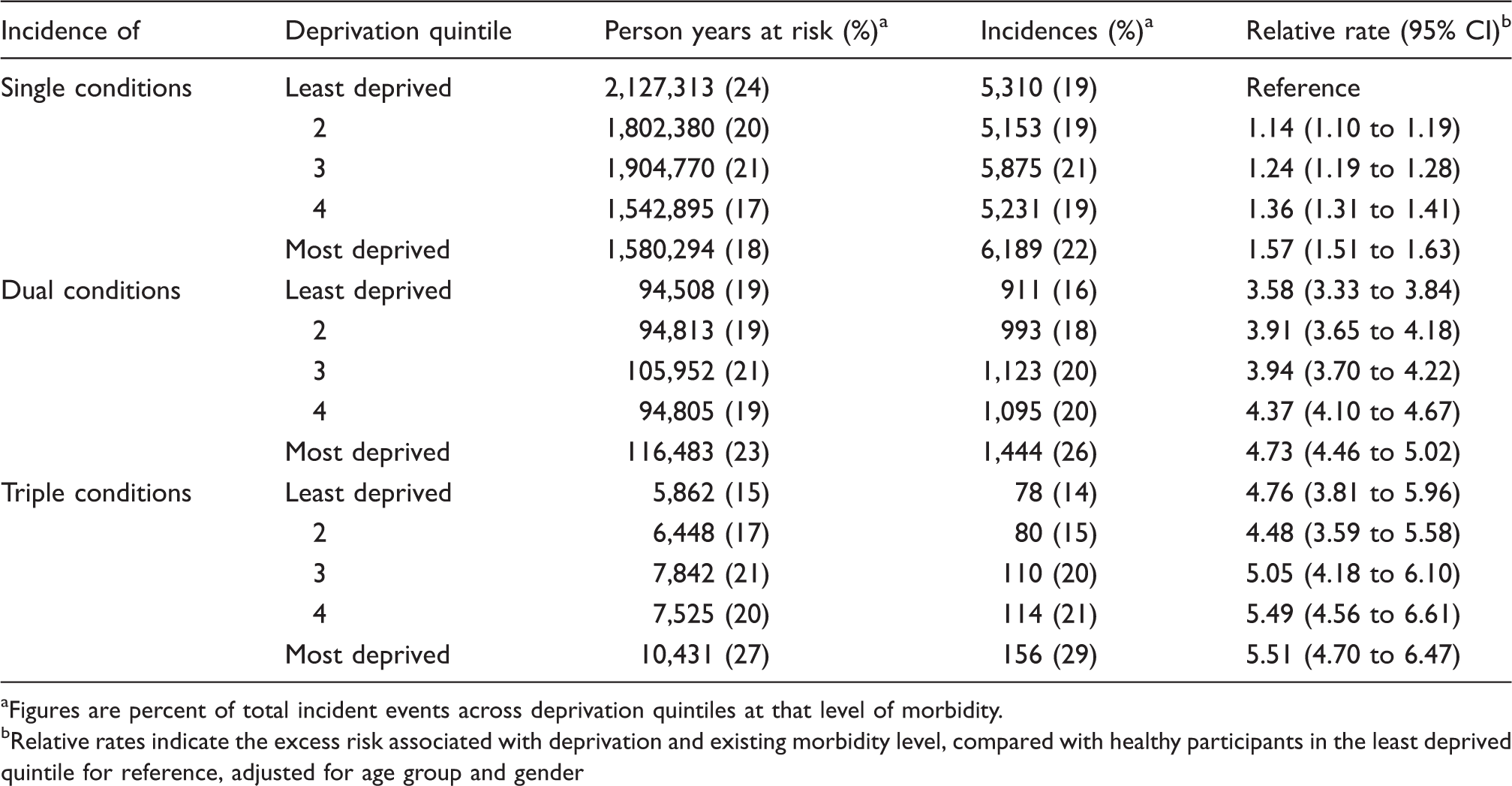
Figures are percent of total incident events across deprivation quintiles at that level of morbidity.
Relative rates indicate the excess risk associated with deprivation and existing morbidity level, compared with healthy participants in the least deprived quintile for reference, adjusted for age group and gender
Mortality from all causes by deprivation quintile at different levels of morbidity. Figures are frequencies except where indicated. Data analysed from the later of 1 January 2007 or start of each participant's record to the earlier of 31 December 2011 or the end of each participant's record.
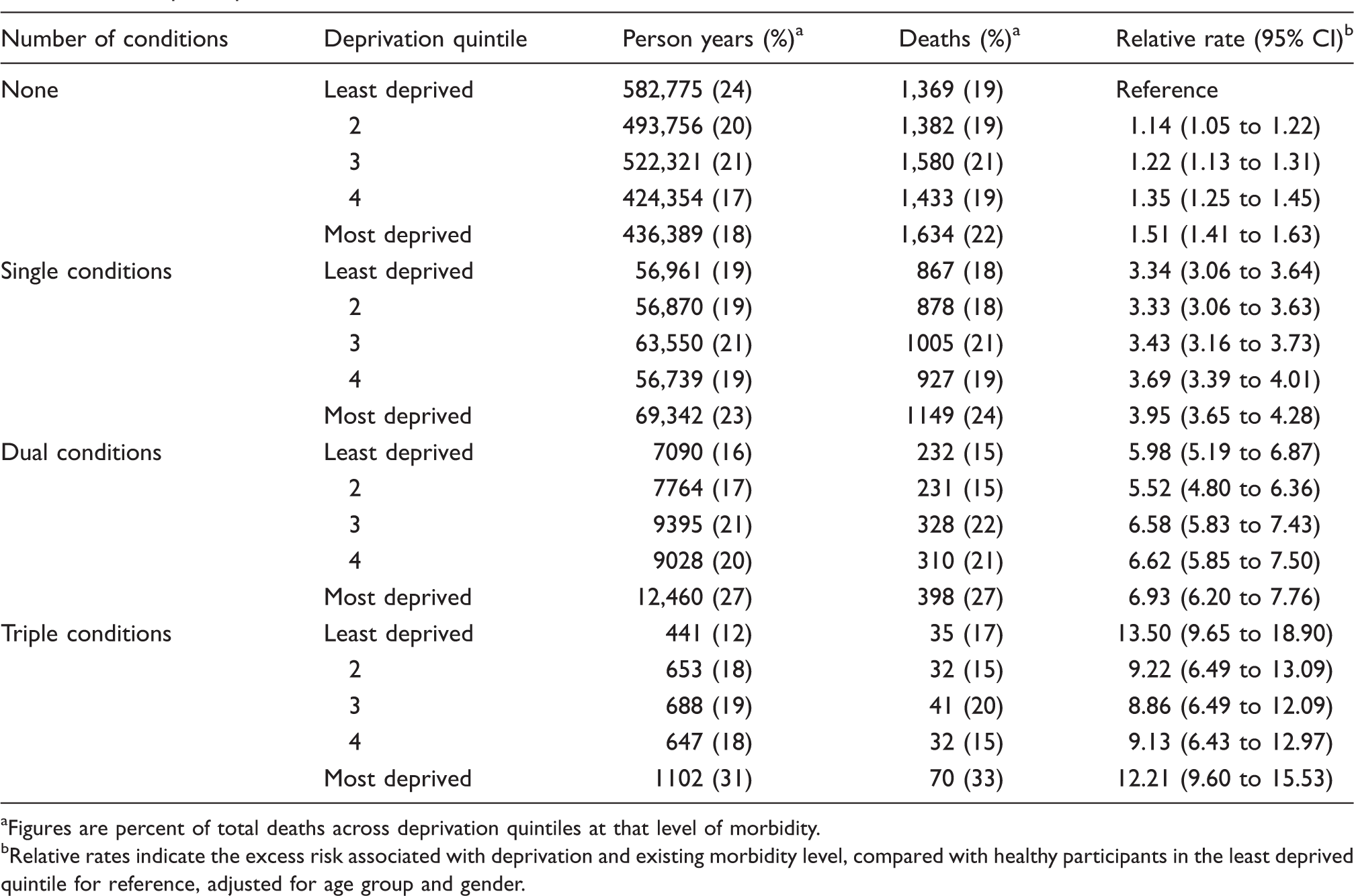
Figures are percent of total deaths across deprivation quintiles at that level of morbidity.
Relative rates indicate the excess risk associated with deprivation and existing morbidity level, compared with healthy participants in the least deprived quintile for reference, adjusted for age group and gender.
Depression prevalence by deprivation quintile at different levels of morbidity. Figures are frequencies except where indicated. Data for 2007 to 2011.
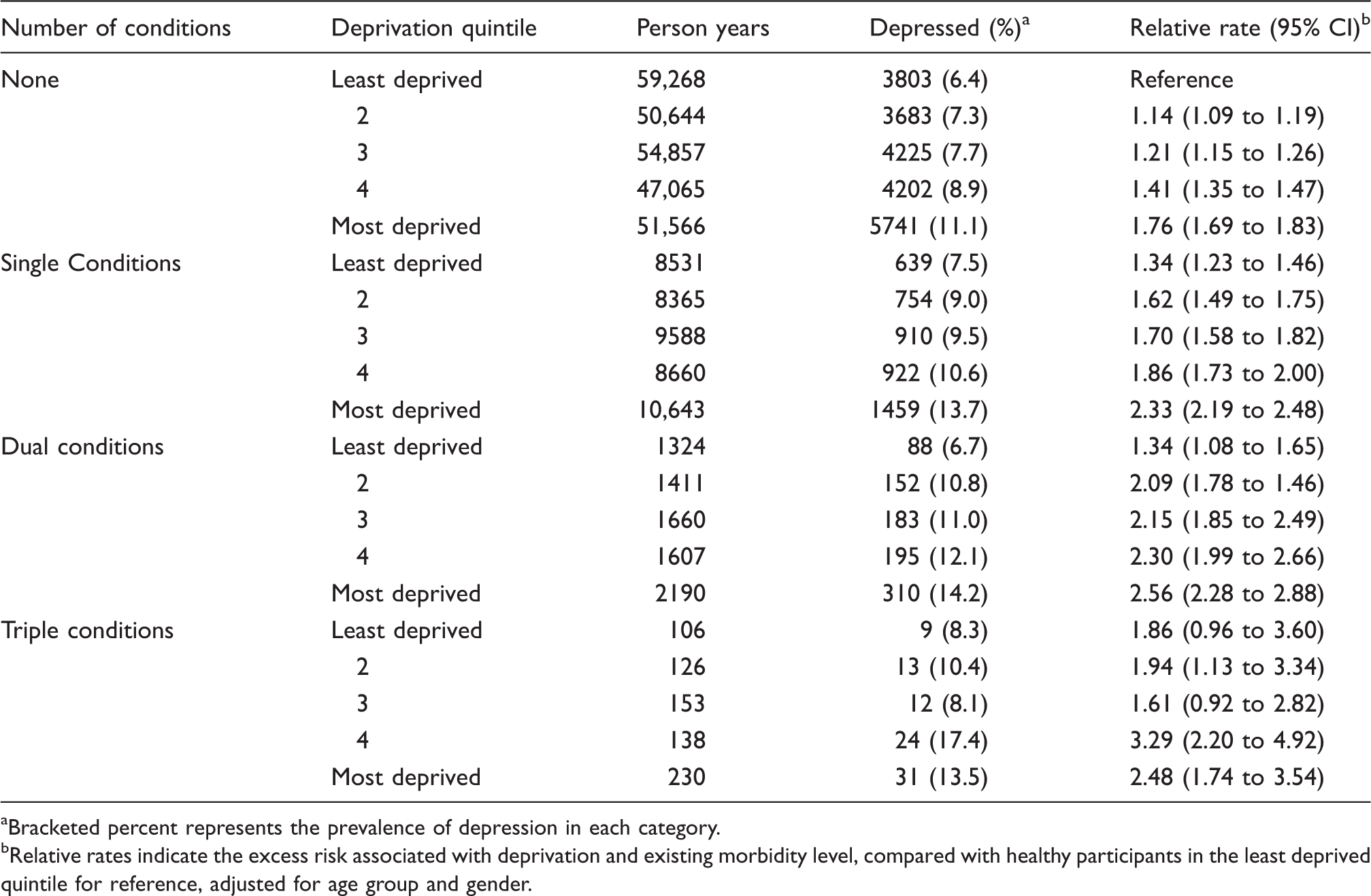
Bracketed percent represents the prevalence of depression in each category.
Relative rates indicate the excess risk associated with deprivation and existing morbidity level, compared with healthy participants in the least deprived quintile for reference, adjusted for age group and gender.
Two-part regression model for patient health care costs. Figures are coefficients (95% confidence intervals). Data for 2007 to 2011.
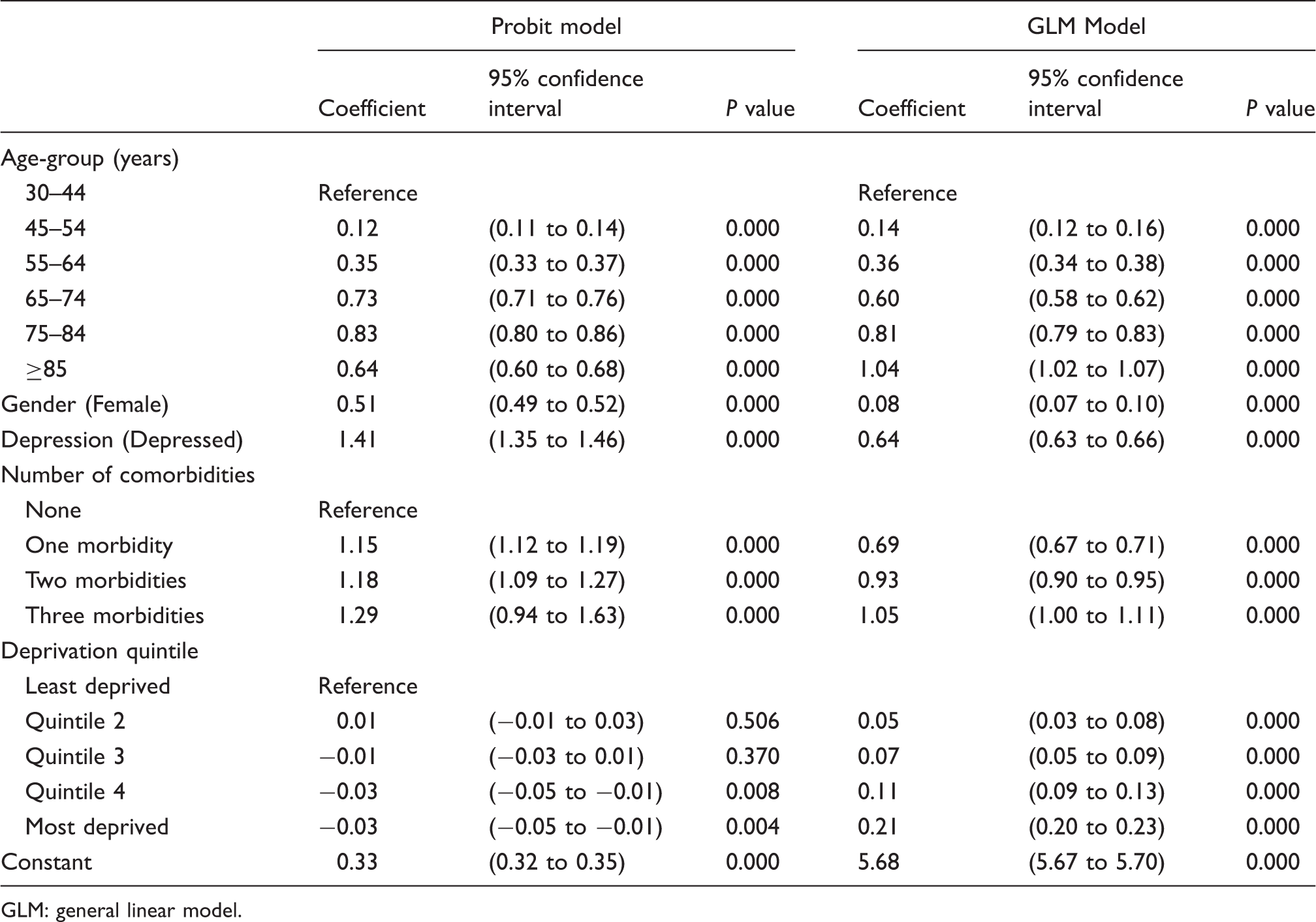
GLM: general linear model.
Predicted mean costs of health care utilization by deprivation quintile, comorbidity and depression for men and women. Figures are UK£ per year, weighted mean of age-specific means. Data for 2007 to 2011.
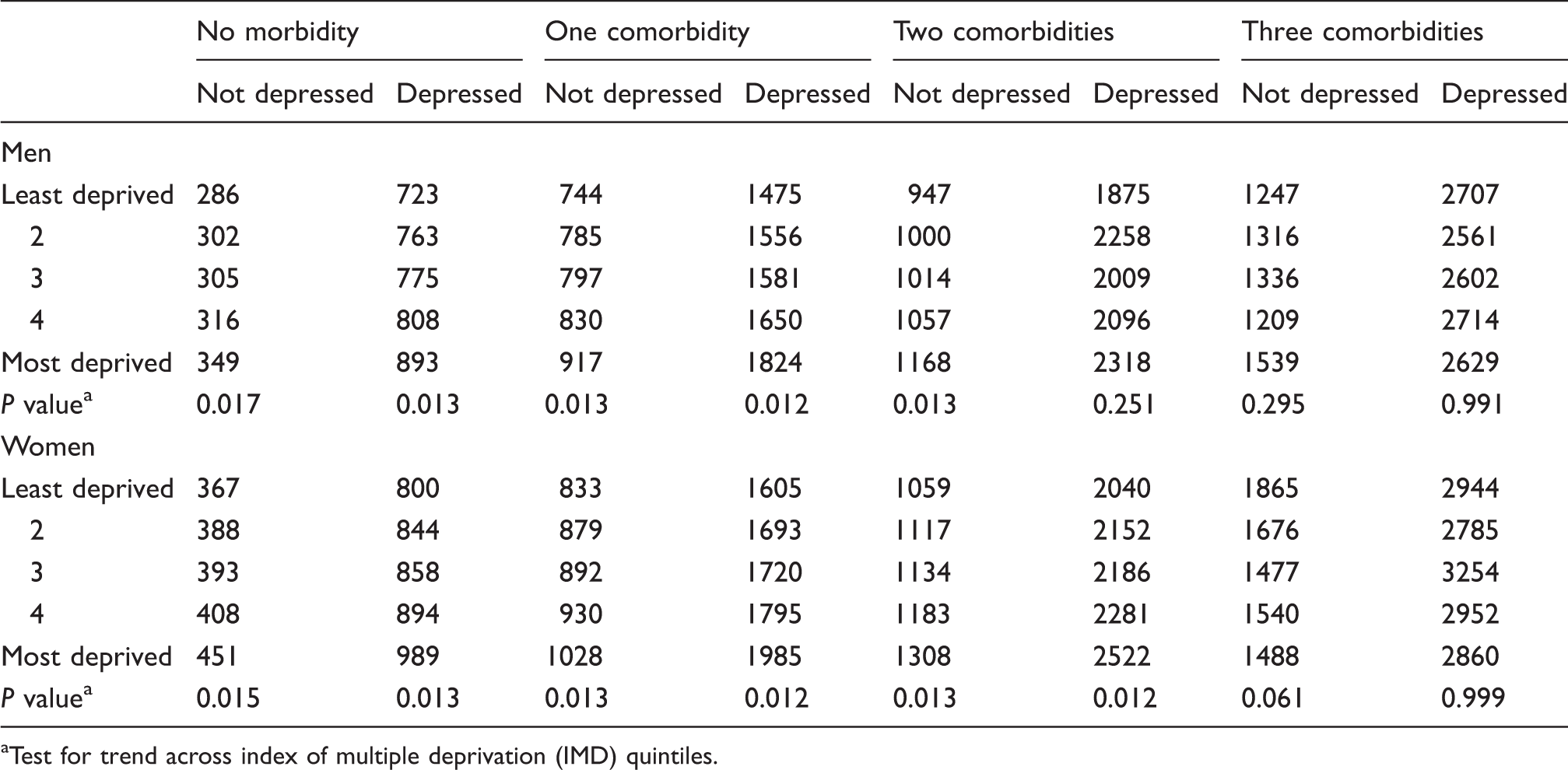
Test for trend across index of multiple deprivation (IMD) quintiles.
Discussion
What this paper shows
This epidemiological study evaluated the impact of deprivation on incidence, mortality, prevalence of depression and health care costs associated with multiple morbidity in a large population. The results show that deprivation is overall strongly associated with the incidence of the study conditions. Participants in higher categories of deprivation are differentially filtered into higher categories of multiple morbidity. Therefore, people living in deprived circumstances represent a much higher proportion of the population with multiple morbidity than of those with single or no morbidity. In the same way, deaths in people with multiple morbidity are more highly concentrated into the most deprived quintile. Paradoxically, relative inequalities in incidence and mortality tend to be smaller as the level of morbidity increases, because the denominator of people at risk, as well as the numerator of incident events or mortality, is influenced by deprivation category. However, depression is more frequent in the most deprived quintile at each level of multiple morbidity. Per capita health care costs are determined by the extent of physical morbidity and, while multiple morbidity is more frequent in deprived populations, per capita costs tend not to be associated with deprivation in patients with multiple morbidity.
Strengths and limitations of this paper
The paper was based on analysis of a very large sample of nearly 300,000 participants drawn from primary care registers in the UK. The CPRD population has been shown to be representative of the UK population in terms of age, sex and deprivation. Clinical diagnoses recorded in CPRD have been shown to have very high predictive values. 15 However, we acknowledge that coding in CPRD is often imprecise 18,19 and each of the conditions identified may encompass a range of presentations and degrees of severity. Problems of misclassification might be greater in deprived areas. We also know that the gap between estimated and reported prevalence for conditions such as coronary heart disease, stroke or hypertension is greater for general practices in areas of higher deprivation. 22 Results are thus likely to underestimate the impact of deprivation on the incidence of single morbidities and related health care costs.
The study only included four types of physical morbidity and one mental health condition, depression. We acknowledge that there are other forms of morbidity including musculoskeletal, respiratory and gastrointestinal disease, as well as other mental disorders, which were not included in these analyses. Future studies should include a wider range of morbidities. There were necessarily smaller numbers of participants with multiple comorbidities and there was more limited power to detect associations with deprivation in participants with three comorbidities. Socioeconomic status was evaluated in terms of social and material deprivation at the small area level. The use of individual-level socioeconomic measures would be preferable. We also recognize that different socioeconomic indicators, such as educational attainment, income and wealth, may show varying patterns of association with health measures, especially in older adults in whom multiple morbidity is frequent. 23 We analysed deprivation in quintiles, as the number of participants with higher levels of multiple morbidity was low, but greater effects might have been observed at more extreme categories of deprivation.
Depression has been defined in different ways even in the context of CPRD research studies. The present definition was the same as used in our previous paper, 14 but the prevalence of depression was somewhat lower here, in data for a later period, in England, and in a more highly selected group of family practices. We caution that it may be difficult to obtain precise estimates for mental disorders from clinical diagnoses and prescriptions in electronic health records.
What other research shows
The association of deprivation with greater morbidity and mortality and higher health care costs is well recognized. Our previous analyses reported on the association of depression with multiple morbidity but did not evaluate associations with deprivation. 14 Brilleman et al. 24 reported on comorbidity and primary care costs and found that while most comorbidities, especially depression, were associated with increased costs, some comorbidities might be associated with more limited costs if items of care were overlapping or if the condition was associated with less intensive intervention. Fewer studies have evaluated the importance of deprivation for people with established morbidity, and little attention has been paid to the impact of deprivation on multiple morbidity, especially in relation to health care costs. Wong et al. 25 reported a crosssectional analysis of an elderly sample in Hong Kong. Their results confirmed an association between depression and both number of comorbidities and socioeconomic status. Droomers et al. 26 found an association between lower socioeconomic status, use of health care services and comorbidities over 9 years in a Dutch sample of respondents 25 years and older. Barnett et al. 13 investigated incidence of one or more morbidities in a crosssectional study of people registered at 314 general practices in Scotland to find that those of lower socioeconomic status were more likely to have multiple morbidities than those who were not and that socioeconomic status was particularly related to mental health disorders. Payne et al. 27 observed an association of unplanned hospital utilization with multiple morbidity, depression and depression, consistent with the findings of the present study.
Policy implications
The findings of this study have implications both for resource allocation and for intervention strategies to attenuate morbidity differences related to socioeconomic status. In England, a weighted capitation formula is used to allocate health care resources to authorities in local areas. In addition to weighting for age and gender and utilization-based estimates of need, the formula currently includes an additional weighting for DFLE. 11 DFLE is strongly associated with deprivation 28 and is included in the formula as a potential measure of unmet need for health care. The present results provide empirical support for this approach, but also provide evidence of greater costs for health service users in deprived areas, through generally greater levels of multiple morbidity, as well as more frequent depression as an important driver of costs. 24 Recent changes in the English NHS may require a reexamination of resource allocation formulae. 29 While these results do not point to specific lessons for how need should be calculated, they highlight the importance of considering the cost implications of deprivation and multiple morbidity and the importance of funding interventions that might prevent these costs. Predictive risk modelling would be likely to pick up these drivers of resource use to inform better allocation decisions. 30 Reducing the impact of deprivation-associated multiple morbidity on health and health care costs requires action related to treatment decisions, as well as resource allocation.
In considering the tasks of the new local commissioners of services, a number of studies have demonstrated that employing effective treatments not only helps patients across the socioeconomic spectrum but can also reduce socioeconomic inequalities in outcomes. For example, increased uptake of specific medical technologies to prevent heart failure was found to reduce absolute differences in heart failure rates by socioeconomic status among patients in the English General Practice Research Database (GPRD) from 1999 to 2007. 31
Conclusions
This study provides new evidence of the impact of deprivation on the occurrence of multiple morbidity. People living in social and material deprivation are channelled, through the higher incidence of disease, into higher categories of multiple morbidity. People living in deprived circumstances live longer with multiple morbidity, and more of those who die have multiple morbidity. Depression is associated with morbidity, but deprivation is associated with a higher prevalence of depression at any level of morbidity. In multiple morbidity, the costs of health care use tend to be more strongly determined by the level of morbidity than the deprivation level. The data emphasize the importance of disease prevention and health promotion to reduce inequalities in health. The findings demonstrate the impact of deprivation on needs for services for patients with multiple morbidity. These needs include not only disease management pathways but also needs for mental health care, social care for attendant disabilities and end-of-life care.
Footnotes
Acknowledgements
The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health. This study is based in part on data from the Full Feature General Practice Research Database obtained under licence from the UK Medicines and Healthcare Products Regulatory Agency. However, the interpretation and conclusions contained in this study are those of the authors alone.
Funding
This study was supported by the UK National Prevention Research Initiative (![]() ) whose funding partners include the Alzheimer’s Research Trust; Alzheimer’s Society; Biotechnology and Biological Sciences Research Council; British Heart Foundation; Cancer Research UK; Chief Scientist Office, Scottish Government Health Directorate; Department of Health; Diabetes UK; Economic and Social Research Council; Engineering and Physical Sciences Research Council; Health & Social Care Research & Development Office for Northern Ireland; Medical Research Council; The Stroke Association; Welsh Assembly Government and World Cancer Research Fund. This research was also supported by the National Institute for Health Research (NIHR) Biomedical Research Centre at Guy's and St Thomas' NHS Foundation Trust and King's College London.
) whose funding partners include the Alzheimer’s Research Trust; Alzheimer’s Society; Biotechnology and Biological Sciences Research Council; British Heart Foundation; Cancer Research UK; Chief Scientist Office, Scottish Government Health Directorate; Department of Health; Diabetes UK; Economic and Social Research Council; Engineering and Physical Sciences Research Council; Health & Social Care Research & Development Office for Northern Ireland; Medical Research Council; The Stroke Association; Welsh Assembly Government and World Cancer Research Fund. This research was also supported by the National Institute for Health Research (NIHR) Biomedical Research Centre at Guy's and St Thomas' NHS Foundation Trust and King's College London.