
Abstract
Background:
While biopsychosocial interventions are recommended for treatment of patients with chronic pain, outcome measurement frequently does not take a multifaceted approach to assessing patient outcomes. As primary care settings increasingly implement chronic pain approaches such as Integrative Group Medical Visits (IGMV), a comprehensive yet pragmatic measurement approach is needed to capture biopsychosocial outcomes.
Methods:
We recruited 21 clinicians, administrators, and staff with direct experience implementing IGMV in safety-net settings to participate in semi-structured qualitative interviews. Participants were recruited from 6 Federally-Qualified Health Centers and 4 Safety-Net Hospital outpatient clinics representing 6 states across the U.S. We first analyzed interview transcripts using the Consolidated Framework of Implementation Research, then used inductive thematic content analysis to identify themes related to what participants currently measure and the outcomes they view as important to be measuring.
Results:
Thematic content analysis revealed 3 themes: variability of measures chosen, rationale for measures chosen, and desire for biopsychosocial outcome measurement tailored to IGMV for chronic pain. Thirteen different measures were used across 9 sites. The choice of measures was driven by clinical utility and/or administrative incentives. Interviewees described that as patients progressed through IGMV they demonstrated improved health through improvements in social support, self-efficacy in pain management, self-management behaviors, and improved physical function. The measures currently used address most but not all these outcomes.
Conclusion:
We recommend developing and refining a biopsychosocial outcome measurement tool that addresses unique aspects of IGMV. These findings contribute to a growing consensus on how to measure actionable, patient-centered data on biopsychosocial interventions for chronic pain.
Introduction
Chronic pain affects approximately 1 quarter of U.S. adults1,2 and is among the most common reasons patients seek primary care. 3 It impacts physical, mental, and social health and is linked to a decline in overall quality of life and personal and economic burdens.1,4 Clinical guidelines 5 and the National Academies 6 recommend an integrative, evidence-based non-pharmacological treatment approach to chronic pain management. One increasingly common model for delivering integrative chronic pain management in primary care is through Integrative Group Medical Visits (IGMV). 7 IGMV provides conventional primary care alongside complementary health approaches (such as mindfulness skills, chair yoga, and nutrition) and peer support in a shared medical appointment format.4,6 IGMVs have been linked to improvement in overall and mental health-related quality of life, 8 social connection, and ability to self-manage symptoms.3,6,8 This complex clinical care model acts on biopsychosocial factors at the individual, group, and community levels that are challenging to assess in busy primary care settings. 8
As researchers, clinicians, and clinical systems strive to measure the benefits, adverse events, costs, and mechanisms of the growing use of IGMV and biopsychosocial approaches for chronic pain care, 9 they do so in a field where there is no standardized approach to outcome measurement reflecting the multidimensional model of this approach. In the absence of consensus on existing outcome measures, our team sought to determine what measures IGMV care teams are currently using in clinical practice and assess their perspectives on what should be measured to assess IGMV for chronic pain.
Methods
For this qualitative study we recruited individuals with experience implementing IGMV in safety-net settings that provide care regardless of insurance coverage (Federally Qualified Health Centers [FQHC] and Safety-Net Hospitals [SNH]). The purpose of the parent study was to investigate barriers and facilitators to implementing IGMVs for patients with chronic pain in safety-net settings to develop implementation strategies to improve access to guideline-concordant chronic pain management in primary care. Interviews primarily focused on factors that impacted implementation of IGMVs for chronic pain, and the interview guide was informed by the updated Consolidated Framework for Implementation Research (CFIR). 10 A semi-structured interview guide informed by CFIR was developed for a previous pilot study 11 and refined for the present study. This protocol was reviewed and approved by the primary author’s Institutional Review Board (21-3380). Additional details of the methodology of the parent study and results of related analyses are reported elsewhere.12,13
Using listservs and snowball sampling, 14 IR invited individuals to participate in virtual, semi-structured, qualitative interviews about their experiences implementing IGMV implementation for chronic pain care. All interviews were conducted by IR, a female Doctor of Public Health whose work focuses on implementation of IGMVs and was previously known to some of the interviewees. Snowball sampling was utilized because experience with implementing IGMVs for chronic pain remains relatively rare and poorly documented. 15 However, some professional networks do exist where clinicians exchange information on best practices. 16 Potential participants were eligible if they had direct experience implementing IGMVs for chronic pain in a safety-net setting. Eligible participants completed a verbal informed consent process via Zoom teleconference.
We recruited 21 interview participants from 10 safety-net settings across 6 states (Table 1). Interviewees included clinicians (n = 15), staff (n = 5), and 1 evaluator (n = 1). Nine of the clinicians included in this sample held an administrative role (such as Medical Director) as well as providing direct patient care. Six of the sites represented were FQHCs, and 4 were SNH outpatient clinics. Each site was represented by between 1 and 3 participants to capture a variety of perspectives from each setting. Interviews were conducted in early 2023, with each interview ranging from 20 to 90 min in length. Recruitment continued until thematic saturation was reached.
Participant Site Description.

Clinicians acting as IGMV co-facilitators and/or administrative oversight.
Staff providing IGMV coordination support.
Interviews were recorded via Zoom teleconference, transcribed by an encrypted transcription service, verified by a team of research assistants, and uploaded to the qualitative analysis data management software ATLAS.ti version 23.2.1 for Windows. 17 No field notes were taken. Data were initially double coded by 2 experienced qualitative researchers (IR and KFB) using a codebook informed by the updated CFIR, 10 and analyzed using directed content analysis. 18
In the sub-analysis presented here, 2 team members, IR who conducted all interviews and led the primary analysis, and ZZ, a public health researcher with expertise in patient reported outcome measurement, conducted a second round of inductive coding. Second-round coding utilized applied thematic content analysis 19 to data previously coded as ‘Implementation Process’, ‘Reflecting and Evaluating’, and ‘Health outcomes’ to examine measures currently being used, current assessment practices, and preferred approaches to assess IGMV patient health outcomes.
Results
Thematic content analysis revealed 3 themes: types of measures used, rationale for measures used, and desire for a set of biopsychosocial outcomes measures tailored to IGMV for chronic pain.
Types of Measures Used
To measure IGMV outcomes, 9 of the 10 sites used validated patient reported outcome measurement tools to assess specific health outcomes (Table 2). Three sites used patient surveys or individual interviews to capture qualitative data.
Validated Patient Reported Outcome Measure Tools Participants Used to Evaluate Health Benefits of IGMV.

Thirteen different tools were used across 9 sites (Table 2). Three sites (2, 3, and 8) used 1 tool and 4 sites (1, 5, 7, and 9) used 2 or more. Interviewees from Sites 6 and 10 didn’t identify a specific tool, but measured the domains of pain intensity, pain interference, physical function, anxiety, overall quality of life, and pain self-efficacy, and discussed the importance of measuring loneliness and ‘group inclusion’, respectively.
Outcome measurement tools varied according to assessment method and number of domains assessed. Most tools (n = 11) used Likert scales, although 2 (the Measure Yourself Medical Outcome Profile [MYMOP] and the Defense and Veteran’s Pain Rating Scale) included open-ended questions or descriptors. Most tools measured just 1 domain: pain (n = 3); depression symptoms (n = 1); anxiety symptoms (n = 1); perceived health (n = 2); perceived loneliness (n = 1); self-compassion actions (n = 1); and self-confidence in health management and information (n = 1). One tool (PROMIS-29) assessed pain and several related health domains, and 1 (Harvard Flourishing Measure) assessed a variety of psychosocial variables.
Rationale for Measurement Tool Choice
Choice of measurement tools was driven by clinical utility and/or administrative incentives.
Clinical Utility
Participants described taking an approach to outcome measurement that recognized and acknowledged the complexity of patient’s symptoms and experiences. Clinicians from both FQHCs (1, 2, and 4) and SNHs (3, 7, 8, and 9) assessed chronic pain-related symptoms, but spoke about the challenge of wanting to acknowledge patient’s pain without reinforcing it.
“. . . I don’t like the idea of continually reminding people about their pain and asking them to put numbers on it. I think what we’re learning is that we’ve been asking people too much about their pain and we’ve been emphasizing it in the medical community.” -Site7_Clin1 “. . . one time [patients] just universally said, ‘We’re not going to fill this out. We don’t think that what you’re asking gets at why we’re here’.” -Site5_Clin/Admin
To address this challenge, one interviewee chose the MYMOP because it was patient-driven, allowing patients to define their symptoms for themselves: “It’s interesting because you can use the patient’s own words. They identify what is most intrusive and bothersome to them, their primary and their secondary symptom, and then you’re tracking pre and post. But it takes that patient reported outcome measure to another level, where you have a patient-identified outcome.” - Site7_Clin1
Administrative Incentives
Interviewees across settings noted that sometimes administrative incentives, such as appealing to funders or insurers, dictated measurement tool choice, explaining, We use the [PHQ-9] across the clinic for everything. That’s what funders like, so we use [it]. - Site 1_Clin/Admin1 “What the insurer did was say, look, let’s agree on certain domains of outcomes: function, social, sleep, stress, psychological issues.” - Site9_Clin/Admin1
However, this could lead to conflicting incentives between administrators, payors, and clinicians: “The data and outcomes that are important to the facilitators and co-facilitators are different than the data and outcomes important to administrators. I think that understanding and learning about the patient’s experiences in the group is more impactful for the people actually providing the care whereas . . . administrators care more about [mental health metrics] . . . they’re looking for objective data that participants’ conditions are improving.”- Site7_Staff2
Desiring Biopsychosocial Outcome Measurement
Interviewees from 7 of the 10 sites spoke about trying to measure complex outcomes such as healing, mindset, reduced suffering, and empowerment, advocating for a nuanced evaluation approach of IGMV for chronic pain.
“Getting to the more qualitative reduction of suffering we can look at this through a non-Western, perhaps an Eastern lens and looking at stigma as well. There’s the actual pain of the injury, then there’s all that stuff that gets heaped upon it because of our medical system, because of our culture, because of our own beliefs about ourselves. I think what a group medical visit can do is significantly reduce the suffering around chronic pain.” - Site6_Clin/Admin2
Interviewees described that as patients progressed through IGMV they expressed feelings of healing through social support, improved self-efficacy in pain management, more effective self-management behaviors, and improved physical function due to continued application of learned skills. Interviewees felt that measuring these outcomes would be useful in evaluating IGMV programs. To reflect this, participant feedback was categorized according to 4 biopsychosocial20 categories that could be used to evaluate the holistic experience of IGMV participation: (1) healing through social support, (2) perceived self-efficacy, (3) self-management behaviors, and (4) physical function (see Figure 1).
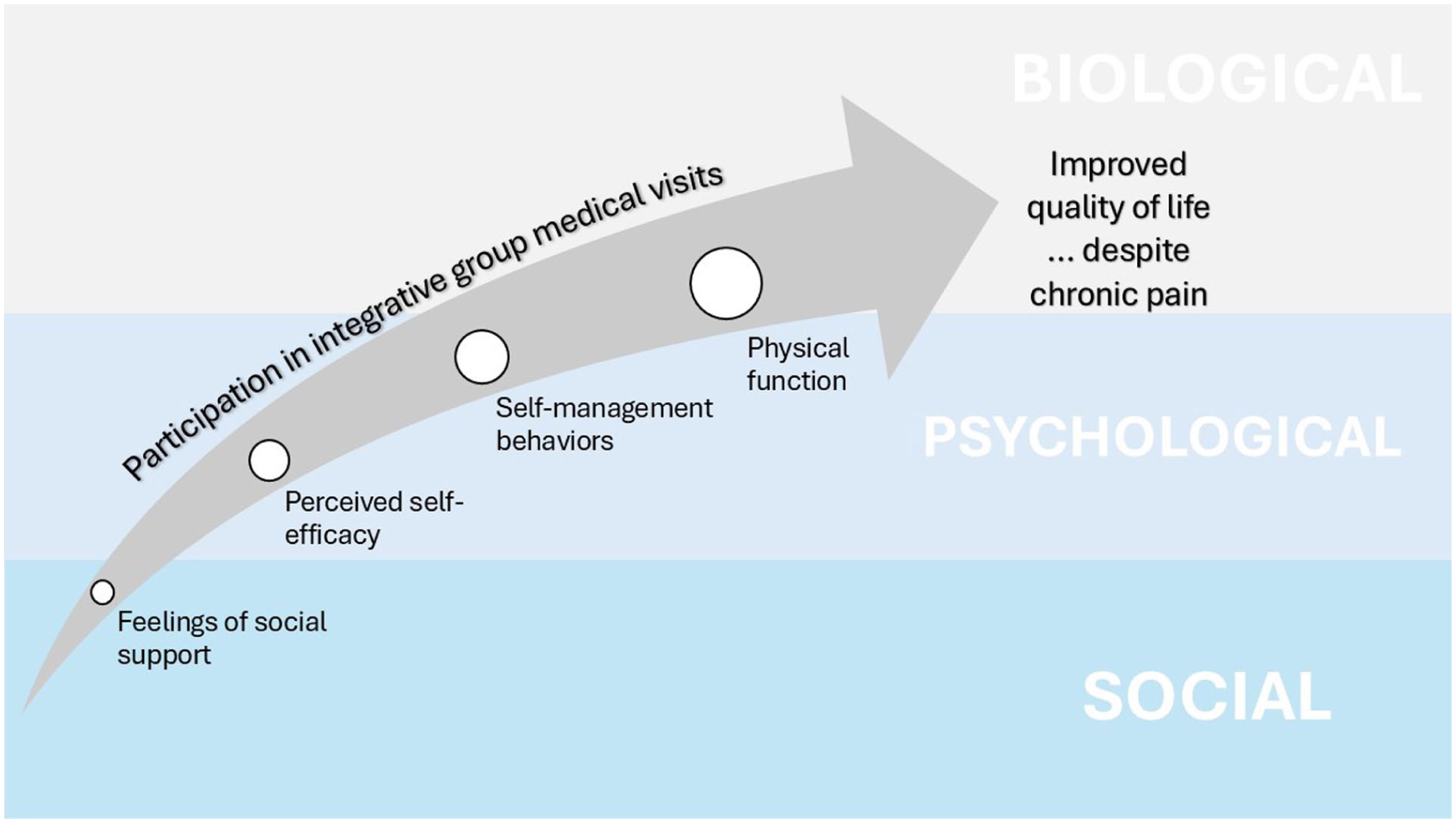
A proposed model of measuring the biopsychosocial impacts of IGMV.
Healing Through Social Support
A majority of interviewees (4 from FQHCs and 3 from SNHs) found loneliness and a lack of social support to be common experiences for many patients with chronic pain, and that IGMV participation provided them with a unique opportunity to realize they were not alone in their struggles: “[patients] say things like, I thought I was all alone, or it’s so powerful to hear somebody else who’s going through something that’s similar to what I’ve been going through.” - Site6_Eval1
Several interviewees stated that IGMV participation fosters a therapeutic milieu, increasing feelings of unity: “I think it works by giving people an outlet. . . to share their feelings, their struggles and connect with other people who have the same issues that they’re having. I think that component of connection and support is really critical in developing a healing environment.” - Site7_Staff2
Interviewees also noticed that patients would develop feelings of accountability and rediscover meaning and purpose and as they realized their unique contributions supported their peers: “. . . to feel connected to a group, you have to, on some level, feel important. Like ‘if I’m not there, people will miss me . . . you’re an active part of the community and that’s where value comes from . . . their ability to feel important and special allows them to want to take care of themselves.” - Site10_Clin/Admin
Healing as a health outcome was identified by several interviewees, particularly after negative or traumatic healthcare experiences: “For some people, there’s a healing component. They’ve maybe even been traumatized or have medical PTSD [post-traumatic stress disorder] and a lot of negative interactions with healthcare. And so having a space that’s a little more equal. . . they really do get this experience of being a whole person within a medical setting.” - Site7_Clin1
Perceived Self-Efficacy
Many interviewees in both FQHCs and SNHs suspected that feelings of purpose and social responsibility contributed to healing, leading patients to shift their mindset about their ability to manage chronic pain. Rather than viewing pain as an insurmountable obstacle, patients began to see an opportunity for resilience. One interviewee noted: “You see story after story . . . it’s that empowered hope. It’s a self-efficacious hope. It’s a sense of yes, there’s tremendous struggle, and I am totally awesome . . . I’m resourceful and capable and I’ve got this tool and that tool, and I learned how to use it this way and that way . . . you see changed behavior when nobody’s watching and pride in a sense, a shifted identity that ‘I’ve got it in me to actually modify in alignment with where I want to be.’” - Site3_Clin2
Interviewees also explained that part of their responsibility as IGMV providers is to improve patients’ self-efficacy in managing chronic pain: “Part of the heavy lift is changing that paradigm to ‘I’m going to do everything I can to manage this myself and avoid doctors’ in so many words. That the hope is that we optimize people’s agency and sense of confidence and competence and working with the pain.” -Site9_Clin/Admin2
Self-Management Behaviors
Interviewees in both settings described that healing through social support and increasing self-efficacy led to patients feeling empowered to apply their newly learned self-management techniques: “. . . I’ve witnessed patients respond differently to their pain condition throughout the group. So initially, maybe they might respond to their pain in a very sort of wincing manner or start complaining about it whereas at the end of the group, they might be, I know this pain is there. Let’s think about something that I can do to . . . help adjust this pain or make this a little bit more comfortable.” - Site7_Staff2
Physical Function
Several interviewees from SNHs recognized that 1 goal of chronic pain management is to return to baseline physical function. An interview from an FQHC setting also expressed wanting to use progress toward physical function goals to measure IGMV effectiveness: “I like patient-directed goals. What would you like to do? ‘I’d like to be able to sit on the floor and play with my grandchildren for 30 minutes.’ Let’s gear everything that you do towards getting you on the floor to play with your grandchildren for 30 minutes.” - Site5_Clin/Admin
Discussion
Our analysis describes the current and potential use of tools to assess health outcomes of patients receiving IGMV for chronic pain. Three themes emerged from our thematic analysis of semi-structured interviews with clinicians, staff, and administrators with experience implementing IGMVs: the type of health outcomes tools currently used, the rationale for tool choice, and desiring biopsychosocial outcome measurement. Nine of the 10 sites reported using at least 1 Patient Reported Outcome Measure (PROM) tool to assess outcomes falling under the broad categories of mental, social, and physical health, employing a mix of single-and multi-dimensional scales consisting of discrete and open-ended items. This use of self-reporting for a variety of health outcomes, including several pain domains, aligns with recommendations for chronic pain assessment20,21 in both clinical 22 and research settings. 23 However, the potential burden of using a variety of tools to capture a more holistic patient picture may make this approach unfeasible in clinical practice. 24 Furthermore, these findings mirror the current literature showing that studies of group medical visits for chronic pain use a wide variety of health assessment tools,9,11,25 highlighting the need for consensus in this area.
The rationale for tool choice also emerged as a theme, with IGMV implementers typically choosing tools according to clinical utility or administrative incentives. The relatively frequent use of the PHQ-9 by respondents highlights the recognition that symptoms of depression commonly co-occur with chronic pain26,27 and may also underscore the top-down influence of clinical recommendations and reimbursement mechanisms on practice. 28 The use of PROMIS tools by 3 sites also underscores both their utility for measuring clinically-relevant outcomes and their widespread recommendation by consensus panels. 29 As a relatively comprehensive tool with demonstrated reliability and validity in the general population, 30 PROMIS measures generate scores for both individual condition-specific domains and overall physical and mental health. 31 However, the fact that PROMIS measures weren’t more widely used to measure health outcomes in IGMVs for chronic pain, even if they may be the best available tool for the job, 32 may indicate that barriers to their use still exist. 33
Developing a Core Outcome Set for IGMVs for Chronic Pain
The final theme to emerge was the desire to measure several biopsychosocial outcomes that are difficult to measure with existing tools. Participants indicated that perceived healing through social support, increased agency over pain management, behavioral changes due to shifting mindset, and progress toward functional goals could all serve as promising health outcome measures of IGMVs for chronic pain. Interviewees also identified that patients in IGMVs advance along a continuum toward improved health, self-management, and physical function, which is highly aligned with guidance on assessment of pain through a biopsychosocial lens. 34 These observations led respondents to advocate for a tool able to assess the health effects of social isolation, perceived self-efficacy, self-management behaviors, and physical function goals. Notably, discrete pain and other condition-specific assessments were excluded due to widespread feelings of resentment by patients for having their life experiences reduced to symptom ratings.
These suggested domains loosely align with recommendations that Core Outcome Sets (COS) for chronic pain include measures of pain intensity and interference, activities of daily living, and quality of life, with optional additional measures of physical function, psychological functioning, and physical quality of life. 34 While these COS recommendations include biopsychosocial elements as they relate to chronic pain as a condition, our study identifies the desire to assess outcomes affected by unique components of IGMV as a care delivery model – social integration and support, participatory medical care, and non-pharmacological chronic pain self-management education and skills-building.7,15 Ultimately, participants agreed on which constructs should be measured to meaningfully evaluate health outcomes in IGMVs, but no single tool currently exists to measure those outcomes and there was no evidence of a sanctioned COS of validated tools able to capture desired outcomes that could be feasibly and pragmatically administered.
These findings suggest that further work is needed to identify an ‘ideal tool’ for pragmatic measurement of IGMVs for chronic pain in primary care that assesses the biopsychosocial nature of the intervention. These recommendations suggest that existing tools measuring constructs such as satisfaction with social participation 35 or emotional support, 36 self-efficacy for managing chronic conditions, 37 pain self-efficacy, 38 and physical function, 39 could be assessed for their utility and feasibility for use in primary care. Existing tools may need to be shortened for ease of administration and evaluated for reliability, validity, and clinical utility in real-world primary settings before widespread adoption is recommended.
Strengths and Limitations
This qualitative study had several strengths, including representation from individuals with direct knowledge and experience in IGMV implementation from sites across the U.S. These findings are particularly compelling because the recommendations were consistent across participants and aligned with similar studies.9,25,40
The generalizability of our findings is limited by the qualitative nature of the study, small sample size, and potential bias from practicing clinicians. Conducting interviews virtually allowed for greater recruitment with limited resources and allowed us to reach busy clinicians during times that were convenient for them. However, other methods such as site visits may provide additional useful context but are more resource-intensive and may be more burdensome for participants. While snowball sampling is useful for reaching rare populations, it is inherently limited by connecting researchers to pre-existing social networks and may represent some ethical challenges when individuals ask others in their social network if they are amenable to being contacted by a research team. 41 Additionally, some of the sites used the tools described here as part of research studies to evaluate their programs. We did not clarify in interviews whether tools were used for research purposes or for routine assessment, nor did we clarify whether tools were embedded into electronic health records for ease of administration. These findings are therefore limited in applicability to routine practice.
This study was specifically focused on participants with experience working in safety-net primary care settings, in preparation for a clinical trial to be conducted in FQHCs. However, other large healthcare systems such as the Veteran’s Administration and other capitated systems have experience utilizing IGMV across a larger number of settings and may be able to provide additional insights on best practices for assessing IGMVs. Further, this study did not include the perspective of patients with chronic pain, who could provide valuable insight on preferences for how they would like their lived experiences to be assessed. Future research on assessing biopsychosocial chronic pain measurement could incorporate a wider range of perspectives across a range of healthcare settings.
Significance
Several studies have demonstrated the beneficial effects of IGMV participation on discrete chronic illness symptoms42,43 and participant 44 and provider satisfaction. 44 In the absence of a perfect measurement tool, the feedback from this study supports the use of multi-dimensional tools to assess IGMV-related health outcomes. Patient-reported outcome measures are fundamental in clinical care and research where there is both a recognition of patient-centered approaches to assess health care outcomes, and an attempt to address conditions lacking objective measures, like chronic pain. Ultimately, these findings contribute to the growing body of research and clinical implementation of biopsychosocial interventions for chronic pain and may contribute to an emerging consensus on measurement to produce actionable, patient-centered data to influence policy.
Footnotes
Acknowledgements
We acknowledge Kate Ferriola-Bruckenstein for her contributions to the first round of analysis of findings presented here.
Ethical Considerations
This protocol was reviewed and approved by the University of North Carolina’s Institutional Review Board (21-3380).
Consent to Participate
All interview participants completed a verbal informed consent process and consented to participation.
Consent for Publication
Not applicable.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: IR’s contributions were supported by grant number K01AT011578 from the National Center for Complementary and Integrative Health.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Deidentified individual data that supports the results will be shared beginning 9 to 36 months following publication provided the investigator who proposes to use the data has approval from an Institutional Review Board (IRB), Independent Ethics Committee (IEC), or Research Ethics Board (REB), as applicable, and executes a data use/sharing agreement with UNC.