
Abstract
Introduction:
Type 2 diabetes mellitus (T2DM) is a pressing global health challenge, affecting over 537 million adults in 2021, with projections of 783 million by 2045. In Sri Lanka, approximately 23% of adults are living with diabetes or prediabetes, whilst many undiagnosed, significantly impacting quality of life (QoL).
Objectives:
To evaluate the impact of T2DM on the QoL of patients in Sri Lanka.
Methodology:
This cross-sectional study included 136 patients with T2DM. Data were collected using a structured questionnaire (sociodemographic and clinical variables) and the WHOQOL-BREF, a validated tool assessing 4 QoL domains: Physical, Psychological, Social, and Environmental. Transformed scores were analyzed statistically across all domains.
Results:
The sample was predominantly female (74.3%), with a mean age of 62.1 ± 10.3 years and an average diabetes duration of 12 years (1-38 years). Overall QoL was significantly associated with psychological, social, and environmental domains (P < .05). Of the participants, 50.7% (n = 69) reported fair QoL, while 26.5% (n = 36) and 22.8% (n = 31) reported poor and good QoL, respectively.
Conclusion:
T2DM substantially affects QoL, particularly in psychological, social, and environmental domains. This underscores the need for comprehensive management strategies to address the multifaceted burdens of T2DM and enhance patients’ well-being in developing countries like Sri Lanka.
Study Importance
What Is Already Known About This Topic?
■ High prevalence of T2DM in Sri Lanka (11.3%-23% in adults) is driven by urbanization, obesity, and lifestyle changes, impacting healthcare systems.
■ T2DM globally reduces QoL, especially in physical and psychological domains, due to chronic symptoms, treatment demands, and comorbidities.
■ WHOQOL-BREF is a validated tool for assessing QoL in chronic diseases, including T2DM, with proven reliability, though its application in Sri Lankan T2DM cohorts is limited.
What Does This Study Adds?
■ Sri Lankan-Specific QoL Data: This is one of the first studies to quantify T2DM-related QoL in Sri Lanka using WHOQOL-BREF, revealing that 50.7% of patients have fair QoL, with the Physical domain scoring lowest (59.11 ± 13.15). This provides a baseline for future regional research and policy development.
■ Sex and Sociodemographic Insights: The study identifies significant sex differences (males report higher QoL, P < .05) and links high BMI and longer diabetes duration to poorer QoL, offering targeted intervention points for Sri Lankan clinicians, particularly for female and overweight patients (74.3% female, 40.4% overweight).
■ Health System Implications: By highlighting the interplay of Psychological, Social, and Environmental QoL domains (P < .05 correlations) in a resource-constrained setting, the study advocates for holistic T2DM care models (ie, integrated mental health support and community-based obesity programs) to address Sri Lanka’s escalating T2DM epidemic.
Introduction
The global epidemic of type 2 diabetes mellitus (T2DM) poses a significant challenge to public health in the 21st century. According to the International Diabetes Federation (IDF), approximately 537 million adults were living with diabetes in 2021, with projections estimating a rise to 783 million by 2045 if current trends persist. 1 T2DM accounts for over 90% of diabetes cases worldwide and is particularly prevalent in the Western Pacific region (206 million cases) and the Southeast Asian region (90 million cases). 1 In Sri Lanka, T2DM prevalence (23% of adults in 2019) strains a healthcare system characterized by free public services but limited specialized care and resources for chronic disease management. 2 Public hospitals and diabetes clinics provide essential care, yet challenges like delayed diagnosis and inadequate self-management support persist, particularly in rural areas, exacerbating QoL impacts. Public hospitals and diabetes clinics deliver vital care, but issues like delayed diagnosis and insufficient self-management support, especially in rural areas, continue to worsen quality of life.
The crisis of T2DM is driven by its associated morbidity and mortality, primarily due to complications affecting multiple organ systems. Early diagnosis and effective management are critical to preventing these complications, yet challenges remain in achieving optimal glycemic control. The American Diabetes Association (ADA) emphasizes comprehensive clinical evaluations and tailored treatment plans to manage T2DM effectively. 3 However, patients face substantial daily challenges, including complex self-management regimens and treatment demands, such as insulin therapy, which can significantly impact their quality of life (QoL) which is defined as individuals’ subjective perceptions of their position in life within cultural, social, and environmental contexts, per WHO. 4 Self-management in T2DM involves daily behaviors (ie, diet, exercise, and medication adherence) to achieve glycemic control, while social determinants (ie, education, income, and healthcare access) 4 shape health outcomes. These constructs, grounded in WHO’s holistic health framework, are critical for understanding T2DM’s burden in Sri Lanka, where data on their interplay remain limited.
Living with T2DM imposes a considerable psychosocial burden, influencing self-care behaviors, long-term glycemic control, and the risk of complications, all of which are associated with QoL. The World Health Organization (WHO) defines health as a state of complete physical, mental, and social well-being, not merely the absence of disease. 4 This perspective has spurred growing interest in health-related QoL as a critical measure in chronic disease management, including T2DM. Despite numerous studies on QoL in diabetes globally, this study explores these associations in a Sri Lankan cohort to address gaps in local data.
This study aims to evaluate the QoL of patients with T2DM in Sri Lanka using the WHOQOL-BREF, a widely validated generic tool with established cross-cultural applicability for chronic conditions. 5 We assessed the sociodemographic profile of patients and explore associations between QoL domains and patient characteristics to inform chronic disease management strategies in resource-constrained settings to leverages its reliability to quantify QoL in a Sri Lankan T2DM cohort.
Methodology
Study Design and Area
This descriptive cross-sectional study was conducted at 3 specialized diabetes centers in Sri Lanka: Sri Jayewardenepura General Hospital, North Central Teaching Hospital Ragama, and Wijaya Kumaratunga Memorial Hospital Seeduwa, from May 1, 2019, to November 30, 2019. These centers were selected to represent diverse urban and semi-urban populations, reflecting varying healthcare access, socioeconomic conditions, and cultural contexts relevant to T2DM management in developing countries.
Sample Size and Sampling
A total of 136 patients with T2DM were systematically sampled. Consecutive patients meeting the inclusion and exclusion criteria were enrolled during routine clinic visits. The sample size was calculated to detect a moderate effect size (Cohen’s d = 0.5) in WHOQOL-BREF domain score differences (ie, between sexes, BMI categories, or diabetes duration groups) with 80% power and a 5% significance level, based on prior QoL studies in chronic diseases. 6
Inclusion Criteria
➢ Willingness to participate and ability to comprehend study information.
➢ Confirmed T2DM diagnosis by a consultant endocrinologist, per ADA criteria (fasting blood glucose ≥126 mg/dL or 2-h oral glucose tolerance test ≥200 mg/dL; 2 values for asymptomatic patients, 1 for symptomatic). 3
➢ Stable disease without hospital admission in the 3 months prior to assessment.
➢ Established T2DM for at least 1 year and receiving treatment at the diabetes clinic for over 6 months.
Exclusion Criteria
➢ Severe comorbidities (ie, stroke and chronic kidney disease).
➢ Pregnancy or other forms of diabetes (ie, gestational diabetes and type 1 diabetes).
➢ Impaired mental function prevents comprehension of study information (ie, severe cardiovascular or neurological disorders unrelated to T2DM)
➢ Concomitant conditions significantly impact QoL (ie, severe cardiovascular or neurological disorders unrelated to diabetes).
Method of Data Collection
Clinical data were extracted from health records by trained doctors who were members of the research team, ensuring consistency and accuracy. Sociodemographic and clinical data were gathered via structured questionnaires, QoL was assessed using a validated tool, and anthropometric measurements were recorded. Double-entry and cross-checking ensured data accuracy.
Sociodemographic and Clinical Questionnaire
A pre-structured questionnaire captured sociodemographic details (age, sex, education level, employment status, and household income) and T2DM-related information (duration since diagnosis, glycated hemoglobin [HbA1c], body mass index [BMI], treatment modalities [ie, oral hypoglycemics and insulin], and comorbidities [ie, hypertension and dyslipidemia]). Clinical data were extracted from health records by trained doctors.
Quality of Life Assessment
The WHOQOL-BREF (Generic English Version), a 26-item short-form of the WHOQOL-100 validated tool, assessed health-related QoL across 4 domains: Physical, Psychological, Social, and Environmental, has established reliability and validity across diverse populations, including South Asian cohorts with chronic disease. 5 Its cross-cultural applicability was confirmed in prior studies, with Cronbach’s alpha ≥.70 in similar settings. 6 In this study, internal consistency was verified (Cronbach’s alpha = 0.815 overall, .708-.775 per domain). Two items evaluated overall QoL and general health satisfaction. Using a 5-point Likert scale, higher scores indicated better QoL. Three negatively phrased items (Q3, Q4, Q26) were reverse coded as per WHO guidelines to ensure consistent scoring. Raw domain scores were transformed to a 0 to 100 scale (100 = highest QoL, 0 = lowest) and categorized as good (>60), fair (40-60), or poor (<40) based on the study population’s mean ± SD, as no universal WHOQOL-BREF cutoffs exist. These categories facilitated comparisons across sociodemographic and clinical variables. Assessments with >20% missing data were discarded; for 1 missing item per domain, the mean of the remaining items was substituted; domains with ≥2 missing items (except Social, where ≥1 was allowed due to its 3-item structure) were not scored per WHO guidelines. All 136 enrolled participants had complete WHOQOL-BREF data after applying this protocol. Interviewer-administered questionnaires were completed during clinic visits.
Anthropometric Measurements
Height and weight were measured over light clothing using calibrated stadiometers and digital scales, following WHO guidelines. 7 Quality control was maintained through standardized training of personnel, weekly equipment calibration, and duplicate measurements by 2 independent observers, with discrepancies resolved by a third measurement.
Statistical Analysis
Data was analyzed using SPSS version 23. Descriptive statistics (means ± SD, frequencies, and percentages) summarized sociodemographic, clinical, and QoL data. WHOQOL-BREF scores were transformed (0-100) and categorized (good: >60, fair: 40-60, and poor: <40) based on mean ± SD, excluding patients with missing domain values. Categories were cross-tabulated against age, sex, education, BMI, diabetes duration, treatment modality, and comorbidities, with chi-squared tests comparing proportions.
Cronbach’s alpha (≥.70 acceptable) assessed the internal consistency of the WHOQOL-BREF, a standard measure of reliability for multi-item scales, consistent with its use in chronic disease populations. Other psychometric properties (ie, test-retest reliability) were not evaluated, as the tool’s validity is well-established. Independent t-tests examined differences in mean WHOQOL-BREF domain scores across binary participant characteristics to assess associations with QoL. Transformed WHOQOL-BREF scores were assumed to approximate normality based on prior studies with similar sample sizes. Normality was verified using Shapiro-Wilk tests (P > .05 for all domains). Multiple linear regression (backward method) modeled the association between WHOQOL-BREF domain scores (dependent variables) and patient characteristics (independent variables: age, sex, BMI, diabetes duration, and treatment modality), adjusting for potential confounders (ie, education level, household income, and comorbidities: hypertension or dyslipidemia). A P-value <.05 indicated significance.
Ethical Considerations
Ethical clearance was obtained prior to the study. Participation was voluntary, with written informed consent obtained. Participants could withdraw at any time without consequence, and confidentiality was ensured.
Baseline Data Definitions
Type 2 Diabetes
T2DM was diagnosed with ADA criteria: fasting blood glucose ≥126 mg/dL or 2-h oral glucose tolerance test ≥200 mg/dL. 3
Quality of Life
QoL was defined as individuals’ subjective perceptions of their position in life within cultural, social, and environmental contexts. 5 WHOQOL-BREF mean domain scores were categorized: >60 (good), 40 to 60 (fair), and <40 (poor).
Results
Patients’ Profile
Of approximately 200 patients screened at the 3 diabetes clinics, 136 met the inclusion criteria and were enrolled, reflecting a systematic sampling approach during routine clinic visits from May to November 2019. Of the 136 patients with T2DM, 101 (74.3%) were female and 35 (25.7%) were male (Table 1). The mean age was 62.1 ± 10.3 years, with 60.3% aged >60 years and only 0.7% <30 years. Nearly all participants (99.3%) were literate. Regarding BMI, 40.4% were overweight (23-27.5 kg/m²), with females exhibiting higher BMI than males. The mean duration of T2DM was 12 years (1-38 years), with 39.7% having a disease duration of 5 to 10 years. Treatment modalities included oral hypoglycemic agents alone (59.6%, n = 81), insulin alone (2.9%, n = 4), or both (37.5%, n = 51). Comorbidities such as hypertension and dyslipidemia were common, with 23.5% having at least one macrovascular complication (ie, coronary artery disease) based on clinical records.
Characteristics of Study Participants (n = 136).

Quality of Life Assessment
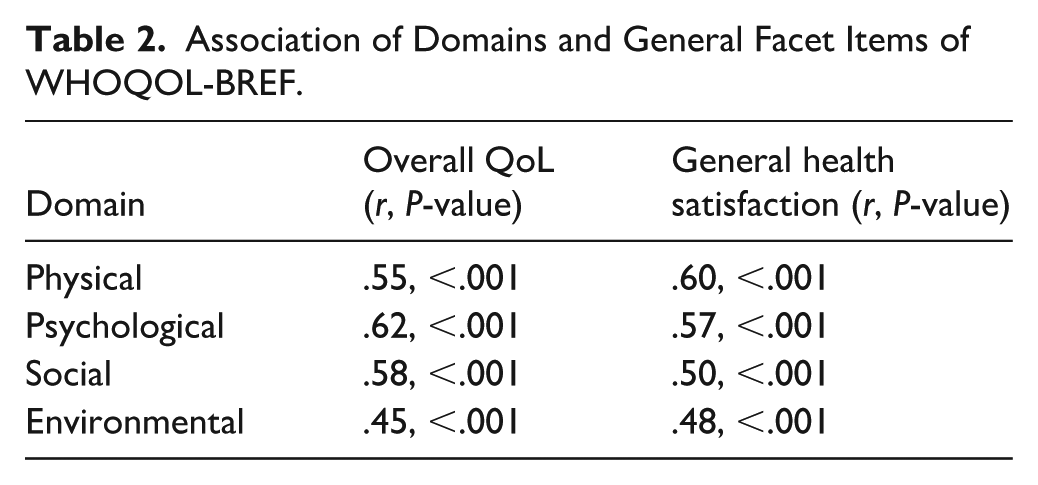
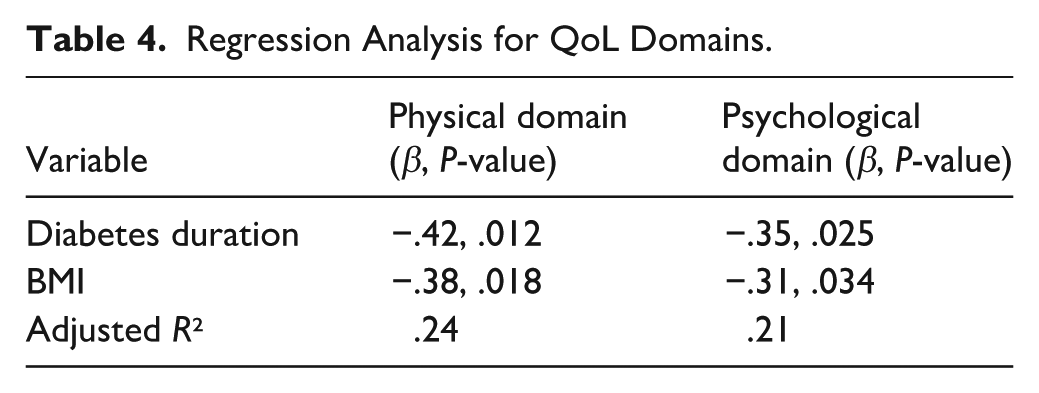
Using the WHOQOL-BREF, 50.7% (n = 69) of participants reported fair QoL (mean domain score = 40-60), 26.5% (n = 36) poor QoL (<40), and 22.8% (n = 31) good QoL (>60). The Physical domain had the lowest mean score (59.11 ± 13.15), while the Environmental domain scored highest, potentially due to adequate healthcare access and socioeconomic support. Mean QoL domain scores were significantly higher in males than in females (P < .05). Significant correlations were observed between all 4 domains (Physical, Psychological, Social, and Environmental; P < .05). Table 2 presents Pearson’s correlation coefficients between WHOQOL-BREF domains and overall QoL/health satisfaction. Significant correlations were observed between all domains (Physical, Psychological, Social, and Environmental; r = .45-.68, P < .05), with Psychological (r = .62, P < .001) and Social (r = .58, P < .001) domains strongly associated with overall QoL perception. Independent t-tests revealed significant associations between QoL domains and participant characteristics (Table 3). Males had higher mean Physical domain scores (62.5 ± 12.8) than females (57.8 ± 13.2; t = 2.34, P = .021). Higher BMI (≥23 kg/m²) was associated with lower psychological domain scores (55.1 ± 11.9 vs 60.3 ± 12.4; t = 2.67, P = .008). Multiple linear regression (Table 4) confirmed that longer diabetes duration (β = −.42, P = .012) and higher BMI (β = −.38, P = .018) were associated with lower physical domain scores, adjusting for education, income, and comorbidities. Multiple linear regression confirmed that longer diabetes duration and higher BMI were associated with lower QoL scores, adjusting for confounders (P < .05). The WHOQOL-BREF demonstrated adequate reliability, with a Cronbach’s alpha of .815 for all 26 items and domain-specific values ranging from .708 (psychological) to .775 (physical).
Association of Domains and General Facet Items of WHOQOL-BREF.
T-Test Analysis for QoL Domains by Characteristics.

Regression Analysis for QoL Domains.
Discussion
Sri Lanka is experiencing a sharp rise in T2DM prevalence, driven by rapid urbanization, globalization, and cultural, behavioral, and environmental shifts. The epidemiological transition, where declining infectious diseases allow longer lifespans and increased chronic disease burden, further contributes to this trend. 8 Sri Lanka’s T2DM prevalence (23% of adults) reflects urbanization and lifestyle changes, posing a public health challenge.1,2 This study of 136 patients at 3 diabetes centers found fair QoL in 50.7%, with the Physical domain scoring lowest (59.11 ± 13.15), highlighting T2DM’s burden on physical functioning in this urban/semi-urban cohort.
The study population was predominantly female (74.3%), consistent with global trends showing higher T2DM prevalence among women due to factors like obesity and gestational diabetes history. 1 The mean age of 62.1 years aligns with evidence that T2DM risk increases after age 45, particularly among the young elderly (60-74 years). 3 High literacy (99.3%) likely facilitated better health knowledge and self-management, positively influencing QoL, as educated patients often report improved glycemic control and self-efficacy. 6 However, 40.4% of participants were overweight (BMI = 23-27.5 kg/m²), with females showing higher BMI, underscoring obesity as a key T2DM risk factor. Excess weight can exacerbate insulin resistance and complicate management, negatively affecting QoL. 9
The WHOQOL-BREF demonstrated strong reliability (Cronbach’s alpha = .815 overall, .708-.775 per domain), consistent with its validated use in chronic disease populations.5,6 The finding that 50.7% of participants had fair QoL, with 26.5% poor and 22.8% good, indicates a moderate QoL burden, aligning with studies showing T2DM’s multifaceted impact on physical, psychological, and social well-being. 10 The Physical domain scored lowest (mean = 59.11 ± 13.15), reflecting challenges like fatigue, medication dependence, and reduced mobility, while the Environmental domain scored highest, possibly due to adequate healthcare access and socioeconomic support in the study setting. Males reported higher QoL scores than females, potentially due to lower BMI and fewer psychosocial stressors. 6 Significant correlations between all QoL domains (P < .05) and associations with Psychological, Social, and Environmental domains for overall QoL perception highlight the interplay of mental health, social support, and living conditions in T2DM management.
Longer diabetes duration and higher BMI were associated with lower QoL (P < .05), consistent with evidence linking prolonged disease burden and obesity to reduced physical and psychological functioning. 9 Age (>60 years, 60.3% of sample) correlated with poorer Physical QoL, likely due to reduced mobility and comorbidities, though older patients may exhibit better psychological resilience. 10 These findings underscore the need for targeted interventions addressing modifiable risk factors like obesity and prolonged hyperglycemia to enhance QoL.
T2DM’s chronic nature and high management costs pose a major challenge to Sri Lanka’s health system. The 23.5% prevalence of macrovascular complications (ie, coronary artery disease) in this study highlights the need for early detection and comprehensive care. Effective screening, lifestyle interventions, and intensified medical therapy can mitigate complications and improve QoL, particularly in resource-constrained settings. 3
The cross-sectional design precludes causal inferences about T2DM’s effect on QoL, and the lack of a non-T2DM comparator limits conclusions about disease-specific impacts. Interviewer-administered WHOQOL-BREF questionnaires may introduce social desirability bias, where participants overreport positive QoL due to perceived expectations, despite standardized training. The study’s focus on Western Province diabetes centers and convenience sampling (n = 136) limits generalizability to rural or less specialized settings. Self-reported clinical data may be subject to recall bias. Nevertheless, these findings have practical implications for Sri Lanka’s healthcare system. Integrating mental health support (ie, counseling for psychological QoL) and community-based obesity programs (targeting high BMI, especially in females) can enhance T2DM self-management. Routine QoL screening using WHOQOL-BREF in diabetes clinics could identify at-risk patients, enabling tailored interventions to improve glycemic control and well-being.
Conclusion
This study highlights T2DM’s significant impact on QoL among Sri Lankan patients, with 50.7% reporting fair QoL, driven by physical limitations and prolonged disease burden. The WHOQOL-BREF proved reliable (Cronbach’s alpha = .815) in assessing QoL, revealing lower Physical domain scores and higher Environmental scores, with sex, BMI, and diabetes duration as key determinants. These findings emphasize the need for early screening, obesity management, and holistic care to enhance QoL in T2DM patients. Sri Lanka’s health system must prioritize cost-effective interventions and routine monitoring to address T2DM’s rising prevalence and macrovascular complications. Future research should employ longitudinal designs and broader sampling to understand QoL dynamics in diverse settings. This study highlights that 50.7% of Sri Lankan T2DM patients report fair QoL, with lower Physical domain scores (59.11 ± 13.15) and higher Environmental scores, associated with sex, BMI, and diabetes duration (P < .05). The WHOQOL-BREF was reliable (Cronbach’s alpha = .815) in this cohort. These findings underscore the need for early screening, obesity management, and holistic care to enhance QoL in T2DM patients. Sri Lanka’s health system should prioritize cost-effective interventions to address T2DM’s rising prevalence and complications. Future research with longitudinal designs and non-T2DM comparators is needed to explore QoL dynamics and causal factors.
Footnotes
Acknowledgements
The authors thank all study participants for their willingness and efforts devoted to this study.
Ethical Considerations
Ethical clearance was obtained from the Ethics Review Committee of the Faculty of Medicine, University of Kelaniya, Sri Lanka, and administrative approval was secured from hospital representatives.
Author Contributions
S.S., I.E., and D.K., collection and/or analysis of data and manuscript revision; D.G., conceptualization and design of the study, analysis of data, and manuscript drafting.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.