
Abstract
Background:
Antiretroviral therapy (ART) has increased life expectancy of HIV/AIDS patients, but the quality of life (QOL) still remains the same.
Methods:
In this cross-sectional study, 356 people living with HIV (PLHIV) were interviewed to assess their QOL using WHOQOL-HIV BREF questionnaire. The association between QOL with sociodemographic, clinical and cohabitation status of the participants was tested using ANOVA and Student t-test, and p value < .05 was considered statistically significant.
Results:
Physical domain of QOL showed maximum score of 16.4, while a minimum score of 12.2 was seen in social relationship domain. Participants with higher socioeconomic status (SES) and self-motivated to take ART had shown better scores across all the domains of QOL (p < .05).
Conclusion:
In our study, quality of life was high among males, younger patients, married participants, higher socioeconomic status, longer duration of ART, self-motivation to take ART, absence of opportunistic infection, and with higher CD4 count.
Introduction
With the introduction of highly active antiretroviral therapy (HAART) and scaling up of its availability, life expectancy of the infected persons has increased. 1 In the HAART era, infected individuals might live a longer life; however, they might not lead a well-satisfied life. So determining quality of life (QOL) is considered to be essential to identify the overall well-being of people living with HIV (PLHIV).
As there is no cure for HIV infection and no vaccines are available for its prevention, the infected person has to follow antiretroviral therapy (ART) regimen lifelong, which had led to PLHIV facing increasing health-related challenges pertaining to the disease, managing medication, side effects due to medication and aging. Hence, it is important to determine the factors contributing to better QOL among PLHIV. Studies have shown an inverse relationship between QOL and factors like HIV infection stages, unemployment, perceived health status, stress and medication adverse effects due to ART, 2 and depression, which in turn are associated with social support and self-esteem. 3,4 Factors affecting QOL might be interlinked to many health-related factors. So QOL has become an important indicator for implementing HIV health-related intervention.
World Health Organization (WHO) has defined QOL as “individual’s perception of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards and concerns.” 5(p01) As QOL shows wide variations depending on different sociodemographic and clinical characteristic of the individuals, 6 -8 measuring QOL and determining factors affecting QOL will help us in understanding which domains of the QOL are commonly affected and will also provide regional data for planning intervention strategies to improve the QOL among PLHIV. In this study, we have assessed the QOL and factors influencing it among the PLHIV in coastal South India.
Methodology
Background Information of the Study Area
Mangalore city is the administrative headquarters of the Dakshina Kannada District and the fourth largest city in the state. Mangalore city spans an area of 200 km2 and has a population of 4.9 lakhs, with 94.03% literacy rate. 9 The prevalence of HIV has been showing a declining trend in Dakshina Kannada District during the past 4 year, however, the HIV prevalence rate of 0.75% is higher than the state prevalence of 0.52%. 10
Study Settings and Design
In this cross-sectional study, 356 PLHIV attending Infectious Disease Department of a tertiary care hospital in Mangalore, Karnataka, were interviewed, and QOL was assessed during the period from April 2014 to December 2014.
Sample Size Calculation
Sample size was calculated considering the expected proportion of adherence to ART among PLHIV as 63.7%, 11 and convenient sampling method was used for recruitment of participants.
Ethics Approval
The protocol was approved by the Institutional Ethics Committee (IEC) at Kasturba Medical College, Manipal University, Mangalore prior to the commencement of the study.
Study Population
Study participants included PLHIV aged 18 years and above and those who were on ART. People living with HIV were approached and explained about the objectives of the study in local language (Kannada), and written informed consent was obtained from the PLHIV who were willing to participate in the study.
Data Collection
The data were collected by face-to-face interview. Patient’s confidentiality was maintained by interviewing them in separate room. The average duration of interview was about 30 minutes. Baseline characteristics of the study participants were collected using pretested semistructured questionnaire which included sociodemographic and clinical characteristics (gender, age, marital status, ART availability, duration of ART, distance traveled, motivation to take ART, opportunistic infections, CD4 count, mode of transmission, and cohabitation status), and socioeconomic status (SES) was assessed using modified Kuppuswamy scale, 12 which includes education, occupation, and income of the participants.
Quality of life was assessed using World Health Organization quality of life (WHOQOL) HIV-BREF instrument. 13 The WHOQOL-HIV BREF questionnaire includes 31 items distributed into 6 domains, namely, physical (4 items), psychological (5 items), level of independence (4 items), social relationship (4 items), environment (8 items), and spirituality (4 items), and 2 items about overall general health. The respondents answered each question using a 5-point Likert-type scale. Scores of negatively directed questions were reversed to make scores higher. Higher scores generally indicate better QOL. Average scores of all items in each domains were multiplied by 4 to convert domain scores to the range of 4 to 20 to make it comparable with the scoring pattern of WHOQOL-100.
Data Analysis
The collected data were entered and analyzed using SPSS version 16.0. The association between QOL domain scores with sociodemographic, clinical characteristics, and cohabitation status of the participants was analyzed using one-way analysis of variance and Student t test. A P value < .05 was considered to be statistically significant.
Results
Sociodemographic and Clinical Characteristics
Of the 356 study participants, 224 (62.9%) were males. Majority of them (41.3%, n = 147) were aged between 41 and 50 years and 65.7% (n = 234) were married. Majority of them (44.1%, n = 157) had been receiving ART for more than 3 years and 48.6% (n = 173) of the participants belonged to middle/lower middle class of SES.
Opportunistic infections were present among 6.2% (n = 22) of the participants. CD4 count ranged from 201 to 600 cells/mm3 among 59.6% (n = 212) participants, and 53.4% (n = 190) of the participants cohabitated with their spouse and children. The sociodemographic and clinical characteristics of the participants are shown in Table 1.
Sociodemographic and Clinical Characteristics of the Participants.a

Abbreviation: ART, antiretroviral therapy.
aN = 356.
bMultiple responses.
Quality-of-Life Scores
The mean (standard deviation) of transformed scores ranging from 4 to 20 across the 6 domains of QOL is shown in Table 2. Physical domain of QOL showed a maximum score of 16.4 (2.2) and social relationship domain showed a minimum score of 12.2 (1.7) among our study participants.
Transformed Scores of the 6 Domains of QOL.a
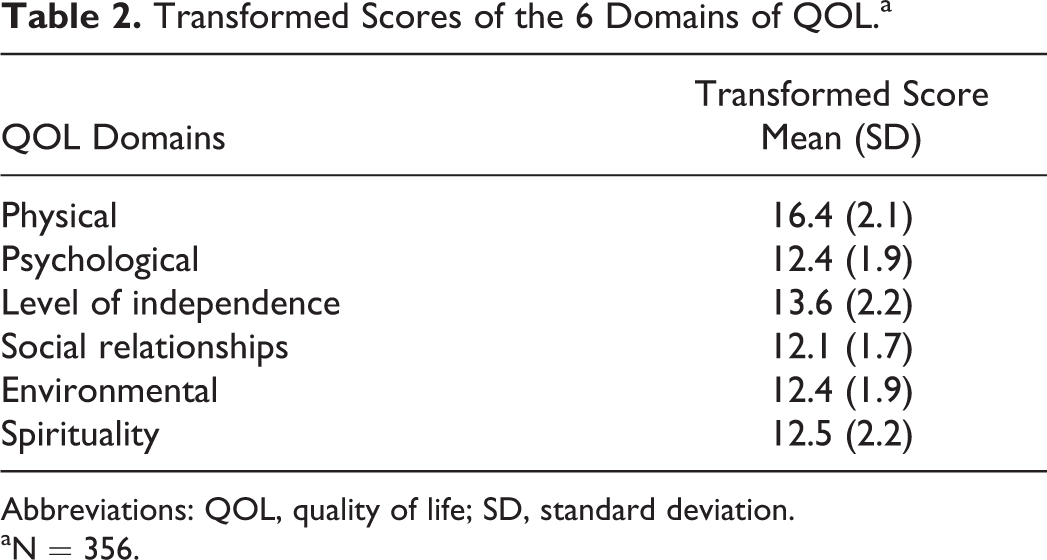
Abbreviations: QOL, quality of life; SD, standard deviation.
aN = 356.
Association between QOL Scores with Sociodemographic and Clinical Characteristics
Association between QOL domain scores with sociodemographic and clinical characteristics of the participants is shown in Table 3. We observed that participants with a higher SES had higher scores in all the 6 domains of QOL, and this association was found to be statistically significant (P < .05). Participants who were self-motivated to take ART also have showed higher scores across all the 6 domains of QOL with statistically significant association (P < .05).
Association between the Quality of Life and Sociodemographic and Clinical Characteristics of the Participants.a

Abbreviations: ANOVA, analysis of variance; WHOQOL, World Health Organization quality of life; SD, standard deviation; SES, socioeconomic status; ART, antiretroviral therapy.
aN = 356.
bStudent t test.
cANOVA test.
A statistically significant association (P < .05) was observed with the marital status and age of the participants in physical, psychological, level of independence, and social relationship domains of QOL, and participants who are married had shown higher QOL domain scores than those who are unmarried and widowed.
People living with HIV having opportunistic infections had lower domain scores and statistically significant (P < .05) association was found with respect to physical, psychological, and level of independence and environmental domains of QOL. CD4 count of the participants showed significant association in all the domains except social relationship and environmental domains of QOL. Participants with higher CD4 counts had shown higher QOL domain scores.
Participants who were receiving ART for longer duration (>36 months) were having higher scores in all the domains of QOL with statistically significant association (P < .05) in physical, psychological, level of independence, and environmental domains of QOL. With respect to gender, males have shown higher scores compared to females across all the domains, and there is a significant association with psychological and level of independence domains of QOL.
Association between the QOL with Cohabitation Status
In relation to the patient’s cohabitation status, participants living with spouse and those living with spouse and children showed higher QOL scores in all the domains, whereas participants living with their children showed lower scores in all domains of QOL than those who are not living with their children. Statistically significant association was found in physical, psychological, and level of independence domains of QOL. Associations between the QOL with cohabitation status of the participants are shown in Table 4.
Association between the Quality of Life and Cohabitation Status of the Participants.a

Abbreviations: WHOQOL, World Health Organization quality of life; SD, standard deviation.
aN = 356.
bStudent t test.
Discussion
Mean QOL domain score was maximum for physical domain followed by level of independence, psychological, environmental, and spirituality domain of QOL. Social relationship domain showed the minimum score. Physical, psychological, and level of independence domains of QOL have shown a significant difference between gender, that is, males were having better QOL scores compared to females. These findings are consistent with other study findings, 14 -16 however, some studies have also shown no significant difference with respect to gender. 17,18 Higher QOL scores in our study among males could be due to better social environment and job opportunity compared to females, which helps to deal with HIV disease and cope with treatment.
Marital status was significantly associated with physical, psychological, level of independence, and social relationship domains of QOL. Married PLHIV showed better QOL mean scores compared to widowers. Similar findings are observed in other studies. 19,20 Physical, emotional, and psychological support of a spouse are more important when compared to support from rest of the family, and this could be a reason for better QOL scores of married participants in our study.
It was observed that participants with higher SES showed better QOL domain scores. Majority (49.3%) of the participants belong to middle/lower middle class SES, and a significant difference was observed in all the 6 domains of QOL across all the SES. These findings can be explained by high literacy rate and better awareness about HIV disease in costal South India. Educated patients have a better understanding about the disease, treatment availability, prevention, and spread of HIV infection. They will also be able to comprehend instructions regarding ART and possible side effects and adhere better to the treatment with a good understanding of the whole treatment process. This will in turn lead to better coping attitudes toward disease and improved QOL. Similarly, occupation and income also lead to better health and QOL. In our study, many of the participants were engaged in unskilled work, craft and trade, fisheries, transport and driving, and so on. These activities help them earn money for their livelihood and keep them healthy both physically and mentally, which in turn is responsible for better QOL. Other study findings also suggest higher SES with better QOL. 21 -25
Our study demonstrated that PLHIV who have received ART for longer duration have a significant difference in physical, psychological, and level of independence domains of QOL. Patients who are on ART for more than 36 months have shown better QOL mean scores than patients receiving ART for lesser duration in our study. These findings could be due to side effects and other discomfort at the initiation of ART. Patients may take some time to get adjusted for the particular dosage regimen and also pill burden could be another problem if the patient is having any opportunistic infection. Similar results were reported in different studies and it was found that patients who understand and follow the dosage schedules of ART including dietary restriction and maintenance of good health, higher scores have been observed over period in domains of QOL. 26 -29 Better QOL domain scores were achieved among PLHIV receiving ART for longer duration in other study findings. 30 -32 In contrast, shorter duration of ART and patients who have not followed the ART regimen were observed to have lower QOL scores. 33,34,35
In our study, PLHIV who are self-motivated to take ART showed better QOL scores in all 6 domains of QOL than those who take medication on compulsion. These findings suggest patient’s dedication and obedience toward their treatment, health, and understanding of importance of adherence to ART. Only 6.2% of the participants had opportunistic infections with lower QOL scores in all the domains compared to participants with the absence of opportunistic infection.
Significant difference was observed between CD4 count of the participants and physical, psychological, level of independence, and spirituality domains of QOL. These findings are similar to other studies. 36,15,18,19,23,27,31 This could be explained based on patient’s knowledge regarding the adherence to ART and improvement in CD4 count. As the CD4 count is regularly monitored in our settings, improvement in CD4 counts might encourage participants in the betterment of immunity and to build confidence within them to take good care of their health and thereby providing better QOL, which resembles with other study findings. 20
Patient’s cohabitation status has also affected QOL domain score in our study. As in our study, majority of the participants were married (65.7%), participants living with spouse have shown higher QOL scores with significant difference in psychological, level of independence, social relationship, and spirituality domains of QOL. This could be due to the reason that living with spouse is often helpful financially and also provides social security and safety. Participants living with only children also had shown significant difference in all domains except environmental and spirituality domains of QOL. Patients who are not living with their children had shown better QOL domain mean scores, and this explains the avoidance of disclosure of HIV status to their children and they worry about the spread of HIV infection through blood due to which they are unable to stay longer like others with their children. Participants living with their spouse and children had shown significant difference in physical and social relationship and environmental domain mean scores of QOL, which is mainly due to their good family bonding and better social environment. In contrast, participants living with others and those living alone have not shown any significant difference in QOL domains. These findings may be due to stigma and discrimination faced by PLHIV from the society and family members and also show patients who are unmarried tend to live alone or with other person.
However, as the study participants’ recruitment was done by convenient sampling method among PLHIV attending an infectious disease department of a tertiary care hospital, study results might not represent the general population. In conclusion, the QOL domain scores are high among males, in those of younger age, participants who are married, participants with higher SES, participants receiving ART for longer duration, participants who are self-motivated to take ART, participants with no opportunistic infection, and those with a higher CD4 count.
Participants living with spouse and those living with spouse and children had shown higher QOL domain scores compared to participants living alone and those living with others. Participants living with their children also had shown lower QOL domain scores.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.