
Abstract
Introduction/objectives:
It is suggested that collaborative mental health models, like those used in pediatric mental health care access (PMHCA) programs, can enhance youth mental health care by boosting physicians’ and other healthcare professionals’ (PHCPs) confidence and skills in treating pediatric psychiatric disorders. This study assessed the impact of a PMHCA program on PHCPs by identifying key themes in semi-structured interviews.
Methods:
Semi-structured telephone interviews were conducted with PHCPs enrolled in KSKidsMAP between July 2019 and March 2022. Three researchers independently reviewed transcripts to identify themes with discrepancies resolved through consensus. Demographic data are presented as frequencies and percentages.
Results:
The 25 participants included physicians (n = 14; 56%), nurse practitioners (n = 8; 32%), and other mental healthcare clinicians (n = 3; 12%). Seven themes were identified: (1) Awareness and Education; (2) Resources and Access to Care; (3) Comfort and Confidence; (4) Visibility; (5) Collaboration; (6) Reimbursement and Financial Barriers; and (7) Holistic Care. Program benefits included enhancing PHCPs’ skills and pediatric access to mental health care. Recommendations for improvement included expanding specialist services and increasing program visibility. Key areas to improve pediatric mental health care included better education, workforce expansion, interprofessional collaboration, and reimbursement reform.
Conclusion:
Data highlight the benefits of PMHCA programs in supporting PHCPs’ provision of pediatric mental health care.
Introduction
In the United States, 1 in 5 youth have a mental health concern, 1 yet few receive treatment from a mental health professional.2,3 This gap in access stems from the severe workforce shortage of mental and behavioral health professionals, with 70% of U.S. counties lacking a child and adolescent psychiatrist (CAP).4,5 In rural states, like Kansas, the ratio of CAPs to youth in need decreased in the decade prior to the COVID-19 pandemic, between 2007 and 2016. 6 Even larger gaps are reported for psychologists, social workers, and other mental health professionals. 4 Youth in rural counties are most affected as they are less likely than their urban counterparts to have access to appropriate mental health services, especially therapy, and have similar or higher rates of mental illness. 7 Children in rural areas also experience a delay in diagnoses and therefore are less likely to receive early interventions; some never receive any treatment. 8 Additionally, parents in rural communities often have lower education levels than urban peers and more often experience poverty—both of which are independent barriers to care. Finally, rural communities are less likely to have expert-level health professionals locally making referral more difficult. Historically, the role of primary care physicians, physicians’ associates, and advanced practitioners has been limited to identification and referral, 9 however, this practice is shifting. As pediatric mental health concerns rose surrounding the COVID-19 Pandemic, the American Academy of Pediatrics (AAP), the American Academy of Child and Adolescent Psychiatry (AACAP), and the Children’s Hospital Association issued a joint declaration of a national emergency in pediatric mental health, and called for the integration of mental healthcare into primary care. 10 This declaration and recommendation was supported by the American Academy of Family Physicians. 11 Despite recognizing the increase in pediatric mental illness following the pandemic, most PCPs lack the confidence, experience, and expertise needed to meet this exigency.12,13
One way to address this need is through Pediatric Mental Health Care Access (PMHCA) Programs, which aim to improve access to mental healthcare for youth by building the confidence and skills of physicians and other healthcare professionals (PHCPs). 12 Kansas Kids Mental Healthcare Access Program (KSKidsMAP), a PMHCA program funded by the Health Resources and Services Administration, is staffed by a Pediatric Mental Health Team (PMHT) comprised of a licensed social worker, 3 child and adolescent psychiatrists (CAPs), 1 child and adolescent psychologist, and 1 pediatrician, all board-certified in their respective specialties. The program offers 3 pillars of support for PHCPs: (1) consultation line: provides case consultations for individual PHCPs with the PMHT, offers community and referral resources, as well as information related to screening, diagnosing, and treating pediatric mental health conditions; (2) Virtual TeleECHO clinics: a statewide network of PHCPs meet twice a month for case-based discussions, interdisciplinary treatment recommendations from the PMHT, and peer-to-peer learning to support knowledge in practice 14 ; and (3) PHCP wellness: supports PHCP wellness through mentorship, resources, and TeleECHO sessions.
Since its inception at the start of the pandemic KSKidsMAP has provided almost 900 consultations to PHCPs serving children from all counties within the state. Over 500 PHCPs are enrolled in the program, and because of the rural geography of the state, several PHCPs serve patients in more than 1 county. The purpose of this study is to better understand PHCPs’ perceptions of pediatric mental health care needs at both the state and practice levels, and to gain feedback on strengths and weaknesses of the KSKidsMAP program as it strives to close the care gap in Kansas. The information gathered will help develop strategies to improve not only access to pediatric mental health care but also to services offered by KSKidsMAP and other PMHCA programs.
Methods
Study Design
This prospective observational cohort study used semi-structured interviews from a convenience sample of KSKidsMAP PHCPs to evaluate the impact of this PMHCA program.
Participants
Participants were selected using convenience sampling of the 247 total PHCPs enrolled in KSKidsMAP between July 2019 and March 2022. All semi-structured interviews were conducted on a rolling basis between July 2022 and September 2022 as participants enrolled. Recruitment was through emailed flyers and direct invitations during program activities (e.g., TeleECHO Clinic, consultation line). Responses were reviewed in batches of 5 using a constant comparative method 15 ; recruitment continued until themes reached saturation.
Data Collection
Study personnel conducted the phone interviews after being trained in qualitative interviewing techniques from the team’s evaluation lead, a PhD-level research psychologist with extensive experience in qualitative methods. The evaluation lead also provided oversight throughout the data collection period. Phone interviews were utilized to garner better participation from PHCPs who span the entirety of the large rural state. Participation was voluntary and consent was obtained prior to participation. Interviews were audio recorded, utilized a standardized script, and took on average 45 min. Questions were formulated with study aims in mind and included demographics (e.g., years in practice, PHCP type), practice details, program participation experience and satisfaction, comfort with mental health care, and perceived barriers to providing mental health services to youth.
Analysis
A professional transcriptionist deidentified and transcribed recordings into secure files. Transcripts and interview recordings were independently reviewed for accuracy and clarity by research study personnel before being transferred into REDCap, a secure web-based database application for data storage.16,17 Data were then exported into Microsoft Excel for analysis. Three study team members, including a child and adolescent psychiatrist, general pediatrician, and a researcher with a master’s degree, independently reviewed data and identified emerging themes and subthemes using a grounded theory approach. The study’s evaluation lead also provided oversight and guidance throughout the analytic process. Following independent review, the research team discussed identified themes and subthemes until group consensus was reached. Demographic data are reported as frequencies and percentages. This study was approved by the University of Kansas Medical Center Institutional Review Board.
Results
Participant Demographics
Twenty-five interviews were conducted (10% of total KSKidsMAP enrollment). Participants included physicians (n = 14; 56%), nurse practitioners (n = 8; 32%), and other mental healthcare clinicians (e.g., psychologists, social workers) (n = 3; 12%). Most respondents had been in practice less than 10 years after formal training (n = 14; 56%), in medically underserved areas/populations (n = 21; 84%), in urban counties (n = 14; 56%) and were either hospital affiliated (n = 8; 32%) or worked in private practice (n=8; 32%) (Table 1). Respondents were fairly even in distribution regarding the percentage of patients covered by Medicaid, ranging from 0% to 100%. Ages of patients ranged from 0 to 21 with most respondents seeing less than 20 patients per week for ages 0 to 11, and less than 10 patients per week for ages 12 to 21. The majority of patients spoke English as their primary language, with Spanish as the second most reported. The top mental health conditions observed within their practices were anxiety (n = 25; 100%), depression (n = 25; 100%), and attention deficit hyperactivity disorder (ADHD; n = 21; 84%).
Pediatric Mental Healthcare Access Program (PMHCA) Interview Participant Demographics.

Medically underserved areas or populations.
Almost all participants (n = 24; 96%) identified mental health disorders they were not comfortable screening, diagnosing, and/or treating in youth. The top reported were bipolar disorder (n = 14; 56%), psychosis (n = 13; 52%), and schizophrenia (n = 10, 40%). However, discomfort was still prevalent for more common mental health disorders with 20% (n = 5) reporting some discomfort with ADHD, 16% (n = 4) for autism, 12% (n = 3) for anxiety, and 12% (n = 3) for depression.
Program Utilization
Of participants who utilized the consultation line (n = 14; 56%), all (100%) had a positive experience, would recommend it to colleagues, and would use it again. The majority (n = 9; 64%) implemented practice changes after receiving case consultation recommendations.
More than half (n = 14; 56%) of participants attended at least 1 TeleECHO session (average: 15 sessions; range: 1-40). Most (n = 17; 68%) planned to participate in TeleECHO within the next 6 months, regardless of previous attendance. Of those not planning to participate (n = 8; 32%), scheduling conflicts were the principal barrier. Most participants (n = 22; 88%) stated the program had a positive impact on their overall clinical practice.
Themes
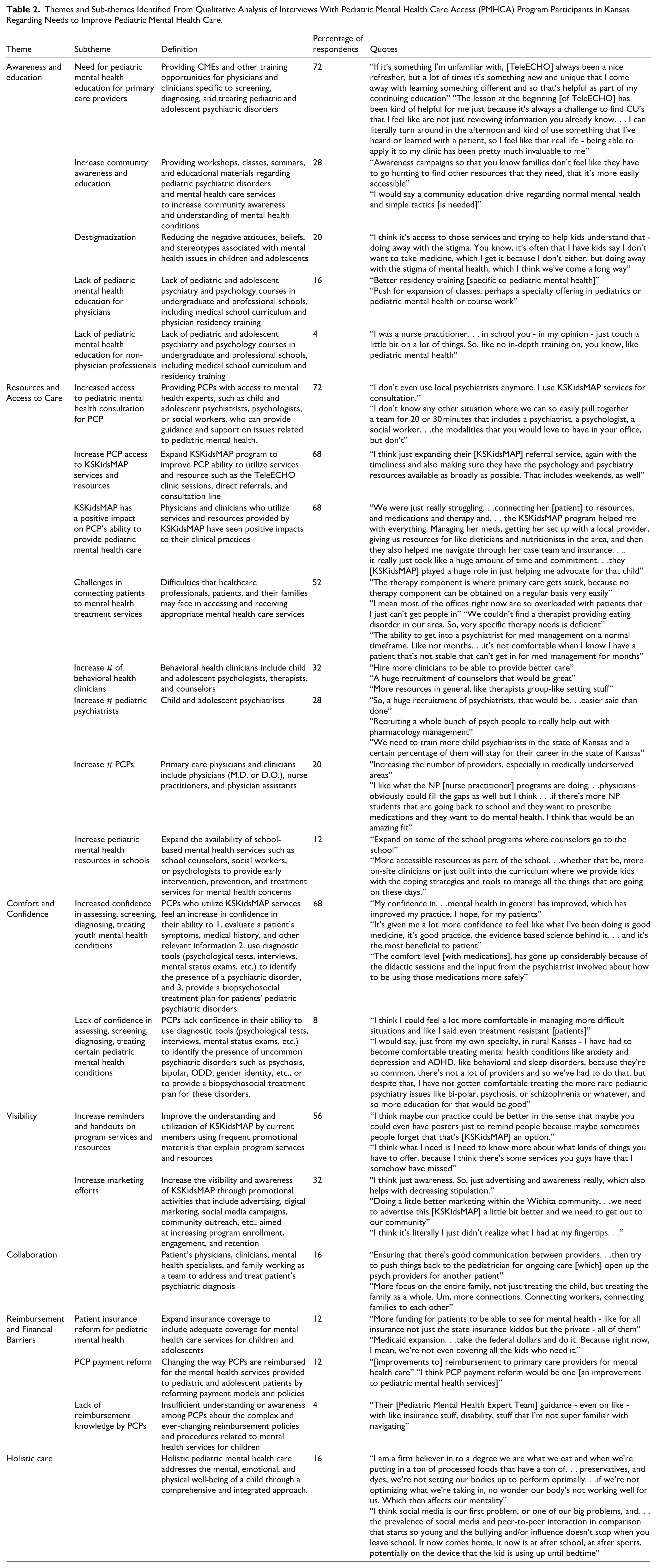
Seven themes emerged from transcription analysis: (1) Awareness and Education; (2) Resources and Access to Care; (3) Comfort and Confidence; (4) Visibility; (5) Collaboration; (6) Reimbursement and Financial Barriers; and (7) Holistic Care.
1. The theme of Awareness and Education highlights the needs expressed by PHCPs not only for pediatric mental health education for PHCPs, but also for communities and includes destigmatization of mental illness. Comments related to this topic include:
I was a nurse practitioner. . . in school you just touch a little bit on a lot of things. So, no in-depth training on pediatric mental health and I think it’s access to those services and trying to help kids understand that - doing away with the stigma. You know, it's often that I have kids say I don't want to take medicine, which I get it because I don't either, but doing away with the stigma of mental health, which I think we've come a long way.
2. The theme of Resources and Access to Care voices the need for PHCPs to increase access to pediatric mental health consultations, resources, and services, including those provided by schools. Interviewees also described challenges in connecting patients to mental health treatment services which they attribute to a shortage of behavioral health clinicians, including child and adolescent psychiatrists and psychologists. Examples of the limited resources experienced by PHCPs was articulated: “The therapy component is where primary care gets stuck, because no therapy component can be obtained on a regular basis very easily.”
The ability to get into a psychiatrist for med management on a normal timeframe. Like not months. . .it’s not comfortable when I know I have a patient that’s not stable that can’t get in for med management for months.
An example of how KSKidsMAP is helping to alleviate resource gaps is described: “I don’t know any other situation where we can so easily pull together a team for 20 or 30 minutes that includes a psychiatrist, a psychologist, a social worker. . .the modalities that you would love to have in your office, but don’t.”
3. The theme of Comfort and Confidence includes PHCPs’ perceived boosted confidence in assessing, screening, diagnosing, and treating youth with common mental health conditions (e.g., anxiety, depression, ADHD), because of support from KSKidsMAP. It also underscores the lack of comfort of PHCPs in addressing more complex psychopathology, such as bipolar disorder or psychosis, which are usually the purview of CAPs. Examples of responses include:
It’s given me a lot more confidence to feel like what I've been doing is good medicine, it’s good practice, the evidence-based science behind it. . . and it's the most beneficial to patient. The comfort level [with medications], has gone up considerably because of the didactic sessions and the input from the psychiatrist involved about how to be using those medications more safely. . . .I have not gotten comfortable treating the more rare pediatric psychiatry issues like bipolar, psychosis, or schizophrenia, and so more education for that would be good.
4. The theme of Visibility addresses the need for the program to improve visibility by sending reminders and handouts on program services and resources as well as by increasing marketing efforts. Voiced suggestions were:
I think it’s literally I just didn’t realize what I had at my fingertips. . . and I think maybe our practice could be better in the sense that maybe you could even have posters just to remind people because maybe sometimes people forget that that’s [KSKidsMAP] an option.
5. The theme of Collaboration which scaffolds KSKidsMAP was highlighted by interviewed PHCPs who find that communication and partnership among the patient’s physicians, mental health specialists, and the whole family represents the best way to achieve optimal results in terms of addressing and treating mental health concerns. Two responses are noted:
Ensuring that there’s good communication between providers. . .then try to push things back to the pediatrician for ongoing care [which] open up the psych providers for another patient. More focus on the entire family, not just treating the child, but treating the family as a whole. More connections. Connecting workers, connecting families to each other.
6. The theme of Reimbursement and Financial Barriers calls attention to the need for reforms regarding not only pediatric mental health insurance coverage but also PHCP payments. It also stresses the need to educate PHCPs about reimbursement practices. Examples include:
Medicaid expansion. . .take the federal dollars and do it. Because right now, I mean, we’re not even covering all the kids who need it and More funding for patients to be able to see for mental health - like for all insurance not just the state insurance kiddos but the private - all of them.
7. Finally, the theme of Holistic Care addresses the desire of PHCPs to target mental, emotional, and physical wellbeing of children with a comprehensive and integrated approach including a focus on proper nutrition as well as limits on social media access. PHCPs voiced the following thoughts:
I am a firm believer in to a degree we are what we eat and when we’re putting in a ton of processed foods that have a ton of. . . preservatives, and dyes, we’re not setting our bodies up to perform optimally. . .if we’re not optimizing what we’re taking in, no wonder our body’s not working well for us. Which then affects our mentality. I think social media is our first problem, or one of our big problems, and. . . the prevalence of social media and peer-to-peer interaction in comparison that starts so young and the bullying and/or influence doesn’t stop when you leave school. It now comes home, it now is at after school, at after sports, potentially on the device that the kid is using up until bedtime.
Each theme was further delineated into subthemes (Table 2).
Themes and Sub-themes Identified From Qualitative Analysis of Interviews With Pediatric Mental Health Care Access (PMHCA) Program Participants in Kansas Regarding Needs to Improve Pediatric Mental Health Care.
Discussion
This study explored PHCPs’ current perception of mental health care provision for youth in primary care practices across the state of Kansas. Additionally, PHCPs reflected on their experience with the state’s PMHCA program, KSKidsMAP, and offered recommendations to improve mental health care for Kansas youth.
Need for Mental Health Awareness/Education and Benefits Experienced by Respondents
The overarching goal of PMHCA programs is to build capacity of PHCPs through training consultation, resources, and referrals. 18 Continuing education is built into each PMHCA program. Even so, the majority (92%) of respondents in this study advocated for additional mental health training. Specifically, 20% advocated for undergraduate pediatric mental health education for physician and non-physician professionals, and 72% voiced the need for continuing education for PHCPs.
One of the greatest benefits from participating in the KSKidsMAP program was increased confidence in evaluating youths’ mental health symptoms using screening and diagnostic interviewing tools and the ability to provide multi-faceted treatment for common psychiatric conditions. Most participants reported a positive impact on their ability to provide quality mental health care and advocate for their patients.
Improved knowledge and mental health competence could give PHCPs the ability to manage care for common mental health problems (e.g., ADHD, anxiety, depression), freeing time for difficult cases that require a CAP’s or child psychologist’s expertise. This concept is foundational to the TeleECHO and PMHCA program models12,13,19 and is of the utmost importance in a rural state like Kansas.
Though all states face shortages of CAPs, rural states like Kansas bear the brunt of the burden. When compared to their urban peers, youth living in rural communities are less likely to receive appropriate mental health care and more likely to die by suicide. 20 With only 15% of the recommended number of CAPs to care for youth most severely affected by mental illness, 21 Kansas must be highly efficient with limited resources. KSKidsMAP utilizes the most highly trained experts in pediatric mental health to train the PHCP workforce so that more children can receive mental health care. Indeed, an important benefit noted by participants was increased access to pediatric mental health expertise.
As PHCPs gain knowledge and confidence in managing common mental health conditions and with improved access to mental health expertise and resources through KSKidsMAP and other PMHCA programs, new venues can be accessed by youth seeking mental health care.
Need for Holistic/Collaborative Care and Improved Reimbursement Policies
Two interrelated themes were the need for holistic care (e.g., exercise, nutrition, sleep, screen time) and collaboration among PHCPs, mental health specialists, and families as members of a child’s mental health treatment team.
Collaborative work in primary care settings appears to benefit not only professionals in terms of improved relations, time saving, and continuing education, but also patients with regard to satisfaction, education, medication adherence, hospital service use, and readmission rates.22,23 Additionally, it is suggested that interprofessional collaboration, which is the fabric of PMHCAs like KSKidsMAP, can reduce the global health workforce crisis, reinforce health systems, and improve health outcomes. 24
Another example of interprofessional collaboration is represented by school-based health clinics (SBHCs) which have been shown to increase mental health care usage by up to 300%, especially for high-risk adolescents. 25 SBHC models were suggested by 12% of participants as a means to increase access to care. Unfortunately, in Kansas, these comprehensive collaborative school-based health clinics are essentially non-existent, with fewer than 12 located in the state. 26 This may be partially due to inadequate reimbursement for pediatric mental health or collaborative care.
As such, participants also called for system changes including simplifying mental health reimbursement policies, expanding insurance coverage for mental healthcare, and implementing payment reform for mental healthcare delivery. Options for reform include standardizing reimbursement rates across population densities and reimbursing adequately for mental illness screening. 27 Despite the 2008 passage of the Mental Health Parity and Addiction Equity Act (MHPAEA), disparities still exist between mental health and non-mental health medical care. Children are 10 times more likely to be seen out-of-network for behavioral health concerns than for primary care, leading to increased costs. Furthermore, in-network provider reimbursement rates are about 20% higher for primary care and medical/surgical visits than for behavioral health visits and children are more likely than adults to be seen out-of-network for behavioral healthcare. 28 Such disparities further inhibit access to mental healthcare for youth.
Need for Improved Access to Mental Health Care and Expansion of Workforce
PMHCAs have been shown to increase PHCPs’ access to psychiatric consultations and behavioral health resources 8 and are uniquely positioned to advocate for reimbursement policies. This may directly impact access to care, as children living in states with similar programs use mental health services more than children in states without them. 29 This aligns with our findings, as 72% of respondents felt the program increased their access to pediatric mental health experts. Nonetheless, half of respondents (52%) continued to experience challenges in connecting patients to mental healthcare (e.g., shortages of specialty appointments, long wait times). These respondents advocated for workforce expansion, specifically behavioral health clinicians (e.g., child and adolescent psychologists, therapists, and counselors), CAPs, PHCPs, and, as reported above, increased school-based mental health services.
Recommendations for Program Improvement
Recommendations for program improvement were noted as the final theme. These include expansion of services and resources, such as recording TeleECHO sessions and increasing program interaction with participants. Participants suggested offering direct referrals and more readily available consultations. Participants advocated for increased visibility of program services, suggesting frequent reminders, handouts, and increasing marketing efforts.
Study Limitations
This study had several limitations. Small sample size (n = 25) limits generalizability; participation was voluntary and may have led to selection bias; and responses were subjective and based on personal experience potentially leading to social desirability response bias. Finally, respondents were participants in the Kansas PMHCA program and results may not be representative of programs in other states.
Future research should engage additional PMHCA sites and focus on program perceptions, patient outcomes and caregiver satisfaction. 30
Conclusion
This study provides an overview of PHCP perceptions regarding a PMHCA program in a rural state. Program benefits include increased PHCP comfort and confidence in the provision of pediatric mental healthcare and improved access to care. The consultation line and TeleECHO Clinics were both highly valued components of KSKidsMAP. Suggested program improvements included expanding access to program services and increasing program visibility. In addition, participants highlighted systemic needs to improve pediatric mental healthcare overall, including increased and widespread education, workforce expansion, improved interprofessional collaboration, and reimbursement reform for mental healthcare.
Through these interviews with Kansas PHCPs, the climate of mental healthcare in a rural state was illustrated. This includes calling out the extreme barriers PHCPs and their patients face when seeking mental healthcare in a state with a critically low workforce. As PHCPs are called to fill this care gap, PMHCAs provide scaffolding through continuing education, specialist consultation, interprofessional collaboration, and advocacy for healthcare reform. Ultimately, in Kansas, KSKidsMAP is expanding the mental health workforce as PHCPs gain comfort and confidence in pediatric care provision. While significant barriers remain—especially regarding direct referral to CAPs and child and adolescent psychologists—this study adds to the growing body of evidence supporting PMHCA programs as foundational in addressing the current pediatric mental health crisis.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319251372514 – Supplemental material for Primary Care Perspectives on a Pediatric Mental Healthcare Access (PMHCA) Program
Supplemental material, sj-docx-1-jpc-10.1177_21501319251372514 for Primary Care Perspectives on a Pediatric Mental Healthcare Access (PMHCA) Program by Susanna Ciccolari Micaldi, Rachel Brown, Sarah Krogman, Carolyn R. Ahlers-Schmidt, Nicole Klaus, Polly Freeman, Ashley Hervey and Kari Harris in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
We wish to acknowledge additional staff within the Departments of Pediatrics and Psychiatry and Behavioral Sciences at the University of Kansas School of Medicine – Wichita, including Evelyn English, BS, and Jenna Wellman, MSW, for manuscript coordination and editing.
Abbreviations
PMHCA Pediatric Mental Health Care Access
PCPs primary care physicians and clinicians
KSKidsMAP Kansas Kids Mental Health Care Access Program
AAP American Academy of Pediatrics
AACAP American Academy of Child and Adolescent Psychiatry
HRSA Health Resources and Services Administration
PMHT Pediatric Mental Health Team
CAPs child and adolescent psychiatrists
MHPAEA Mental Health Parity and Addiction Equity Act
Ethical Considerations
This study was approved by the University of Kansas School of Medicine Institutional Review Board (STUDY00147915) on 11/01/2021.
Consent to Participate
Informed consent was obtained verbally before starting interviews. The consent was audio-recorded in the presence of an independent witness.
Author Contributions
Dr. Susanna Ciccolari Micaldi drafted the initial manuscript; reviewed and revised the manuscript; and approved the final manuscript as submitted.
Drs. Ahlers-Schmidt, Harris, Brown, Klaus conceptualized and designed the study. Led data analysis, and interpretation; drafted the initial manuscript; reviewed and revised the manuscript; and approved the final manuscript as submitted.
Sarah Krogman recruited participants; led data collection, analysis, and interpretation; drafted the initial manuscript; reviewed and revised the manuscript; and approved the final manuscript as submitted.
Ashley Hervey and Polly Freeman reviewed and revised the manuscript; and approved the final manuscript as submitted.
All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Drs. Ciccolari Micaldi, Brown, Ahlers-Schmidt, Klaus, and Harris in addition to Sarah Krogman and Polly Freeman are supported by the Health Resources and Services Administration (HRSA) (U4CMC32911-05-00). KSKidsMAP is a cooperative agreement between KDHE and other state and local partners. The KSKidsMAP program is supported by the Health Resources and Services Administration (HRSA) of the U.S. Department of Health and Human Services (HHS) as part of an award totaling $2 356 944 with 20% financed with non-governmental sources.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Original digital audio recordings and transcripts which underpin all qualitative analyses in this manuscript, are unavailable to protect participant confidentiality as stipulated in the consent process and study protocol.
Role of Funder
The contents are those of the authors and do not necessarily represent the official views of, nor an endorsement, by HRSA, HHS, or the U.S. Government. The funding organizations had no role in the design, preparation, review, or approval of this paper.
Clinical Trial Registry Name and Registration Number
N/A
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.