
Abstract
Introduction
About half of all lifetime cases of mood, anxiety, impulse control, and substance use disorders occur by age 14 years. 1 Thus, the age of onset for lifetime mental health (MH) disorders is concentrated in a relatively narrow age range in adolescence.2,3 Because the signs and symptoms of mental illness may be present 2 to 4 years before the onset of a full-blown disorder, early to middle adolescence is a window of opportunity for screening, detection, and intervention. 4 Early identification of mental illness has been linked to earlier treatment leading to better outcomes, particularly for adolescent depression.3-5 However, detection rates remain low. 6 It is widely assumed that MH screening in primary care settings will promote recognition of underdiagnosed conditions and reduce unmet need for treatment. However, it is not currently known whether routine comprehensive screening increases the proportion of youth diagnosed or shortens time to MH diagnosis, which in turn may lead to earlier treatment. Thus, the primary care provider (PCP) may be the gateway provider who provides or refers youth for MH treatment. 7
The Guidelines for Adolescent Preventive Services (GAPS) is a clinical service tool for the provision of comprehensive adolescent health care. 8 Although not diagnostic, the GAPS questionnaires are used to elicit areas of adolescent risk, which in turn can guide PCP discussion, follow-up, and management. As such, it may be the first step in identifying an MH problem, particularly depression. The GAPS includes questions about depressed mood and anhedonia that are almost identical to the 2 questions included in the Patient Health Questionnaire–2 (PHQ-2), a brief depression screen that has good sensitivity and specificity for detecting major depression among adolescents. 9 In addition, the GAPS includes a question about suicidal thoughts, intention, or plan, thus further increasing its potential for detecting adolescent depression. That said, the psychometrics of the GAPS questionnaire overall have not been formally studied.
Evaluating the GAPS is important because this tool is comprehensive, preventive, and incorporates PHQ-2 depression screening questions that have been validated. GAPS are listed as a primary care resource by the Centers for Disease Control and Prevention 10 and the American Academy of Pediatrics. 11 During implementation of GAPS in our clinic from 1998 to 2000, we found that its use led to increased discussion of risk behaviors during the annual visit, including psychosocial issues. 12 The objective of this study was to determine whether long-term use of the GAPS in our primary care setting led to increased detection and/or earlier MH diagnosis among youth.
Methods
Clinical Setting
Our Pediatric Clinic serves patients aged 0 to 21 years and is located in the hub of an integrated health care system that provides care and services to people living in an 8-county largely rural region covering 5600 square miles in upstate New York.
Intervention Implementation
Three clinic staff attended a training April 17-19, 1998, in Lisle, Illinois hosted by Arthur Elster, MD, who developed the GAPS model. Trained staff, in turn, trained the clinic PCP using the GAPS training materials. By May 1999, the Pediatric Clinic routinely administered the GAPS as a pre-visit screening questionnaire for all adolescent annual visits with a 94% GAPS completion rate 12 .The intermediate outcomes, such as change in PCP discussion and referral rates pre- and post-GAPS, are described in detail in a prior study 12 .
Study Design
A deidentified administrative database was analyzed using 2 analytic strategies: (a) time series analysis of the rate of MH diagnoses from 1994 to 2010, including 8112 adolescents aged 13 to 15 years and (b) a historical cohort pre- and post-GAPS comparison of time to MH diagnoses for 1531 adolescents aged 13 to 15 years. The database included service location, dates of service, date of birth, gender, International Classification of Diseases, Ninth Revision–Clinical Modification (ICD-9-CM) diagnoses, Current Procedural Terminology (CPT) codes and medical record numbers for all visits in the network. Given that half of all lifetime MH disorders start by age 14 years, this study focuses on age range of 13 to 15 years. During the study period, 440 to 568 adolescents aged 13 to 15 years were seen per year.
This study was judged exempt from continuing review by the Bassett Hospital Institutional Review Committee.
Coding for Mental Health Diagnosis
An MH diagnosis was defined as the first ICD-9-CM code in the 291-314 range that occurred on or after the annual visit. Not otherwise specified (NOS) codes, adjustment disorder (309.0-309.9), and alternate or symptom-related codes for behavioral and emotional problems were included.13,14 PCP may use symptom-related codes for MH disorders because of diagnostic uncertainty or subthreshold symptoms, or to avoid denial of service.13,14 Because the GAPS questionnaire includes 3 specific questions for depressed mood, anhedonia, and suicidiality, ICD-9-CM codes for mood disorders (depression 296.xx, depression NOS 311, and anxiety 300.xx) were analyzed separately.
Time Series
Time series analysis was used to trend MH diagnoses for ages 13 to 15 years seen for any outpatient visit from 1994 to 2010. Among these youth, MH diagnoses defined by billed ICD-9-CM codes were enumerated that were concurrent with the annual visit, or occurred at subsequent outpatient visits at any site in the network. MH visits were then restricted to 5 zip codes that included most youths seen in clinic. Because our network includes all primary care sources in this area, we took a population-based approach. School enrollment data for grades 8, 9, and 10 in those 5 zip codes were used as denominators to derive population-based prevalence rates. Annually, 84% (range 76% to 91%) of adolescents from the 5 zip codes had any type of visit in the network. Each adolescent could be included only once per year. The rate of MH diagnosis from May 1, 1994 to April 1, 1998 (pre-GAPS) was compared with May 1, 1998 to April 1, 2010 (post-GAPS) and tested for significance using the Chow test.
Historical Cohorts
Cohorts of adolescents aged 13 to 15 years who had an annual visit pre- or post-GAPS were constructed in order to compare the time to diagnosis over 2 study periods. The index visit was defined using well visit codes for all new (99384) and established (99394) patients and occurring either in pre-GAPS (May 1994 to April 1998) or post-GAPS (May 1999 to April 2003). To include MH diagnoses made at the index visit, the follow-up period began 1 day prior to the index visit. Youth with preexisting MH diagnoses in the 5 months preceding their index visit were excluded. Because of the possible development of MH diagnoses after 5 years, the pre-GAPS cohort was excluded from the post-GAPS cohort. The follow-up time was calculated as the time between the day before the index visit and the day of the last annual visit in the time period (no event), or time between the day before the index visit and the day of the MH diagnosis (event). Using survival analysis, the time to MH diagnoses was compared pre- and post-GAPS for the 2 cohorts.
Results
The time series analysis included 8112 subjects from 1994 to 2010.The most common MH diagnoses were depression, other mood disorders, adjustment disorders, and attention deficit/hyperactivity disorder (ADHD). The trend in MH diagnoses pre-GAPS was significant compared to the trend post-GAPS (P = .01, Chow test), attributable to an increasing rate of MH diagnoses occurring before GAPS was introduced (Figure 1). There was no significant trend in MH diagnosis over the entire pre- and post-GAPS period (P = .13). There was also no significant positive trend in the rate of diagnosis of depression or other mood disorders (P = .14).
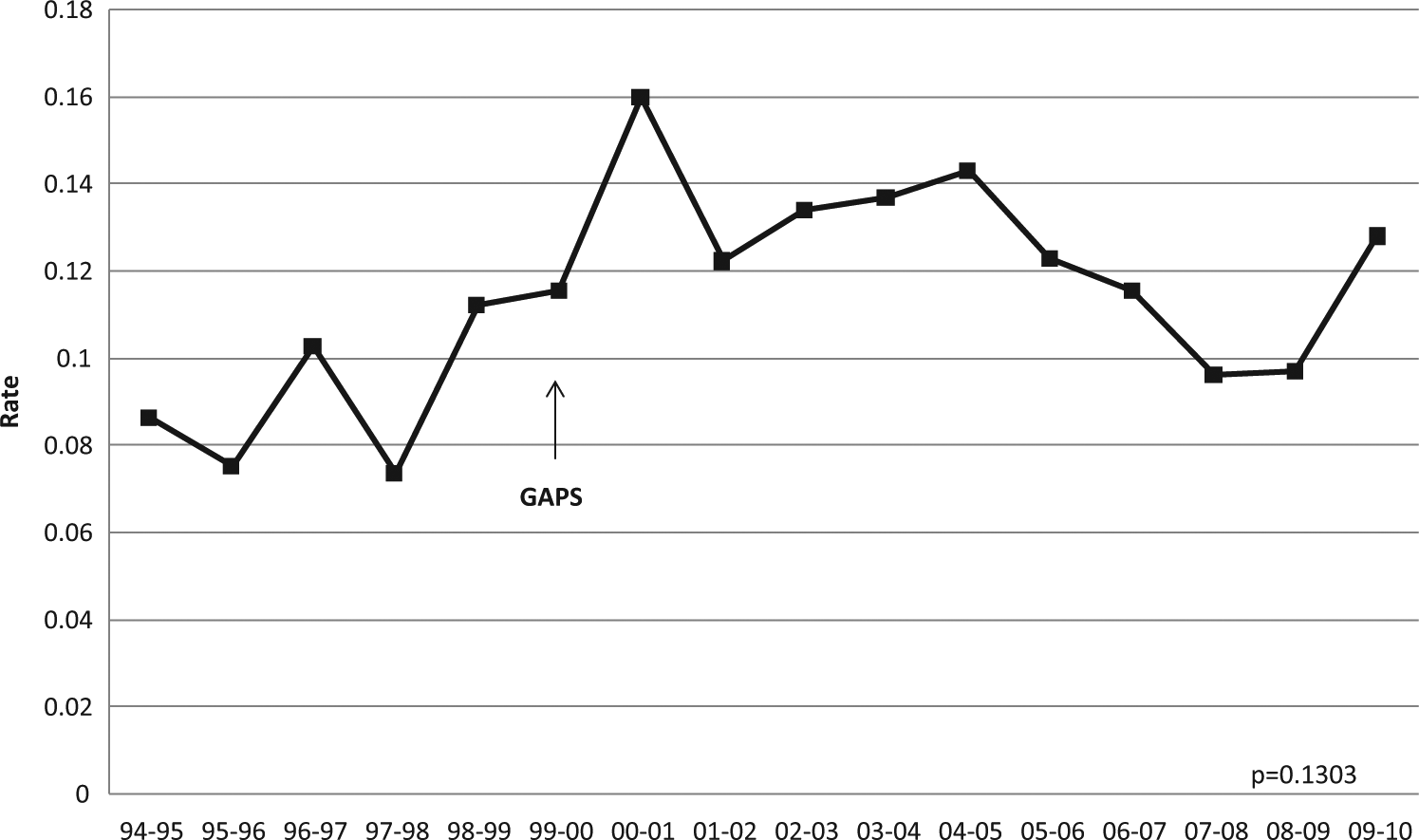
Rate of mental health (MH) diagnosis (ICD-9 CM 291-314, NOS or alternate code) among adolescents aged 13 to 15 years over a 16-year period (n = 8112). Guidelines for Adolescent Preventive Services (GAPS) was introduced in May 1998 and was scaled up to universal screening in April 1999 (arrow). There was no significant change in rate of MH diagnosis over the entire pre- and post-GAPS period (P = .13, Chow test).
Historical cohort analysis included 1531 subjects seen May 1994 through April 1998 (pre-GAPS) or May 1999 to April 2003 (post-GAPS). Sixty-six adolescents (30 pre-GAPS, 36 post-GAPS) with preexisting MH diagnosis were excluded. The leading diagnoses for the 201 adolescents diagnosed during follow-up were depression and other mood disorders (27%), adjustment disorders (19%), and ADHD (15%). Survival analysis showed no difference in time to any MH diagnosis post-GAPS (7.0 months) versus pre-GAPS (9.0 months, log rank P = .30; Figure 2). There was also no significant difference in time to diagnosis of depression or any mood disorder post-GAPS (12.2 months) versus pre-GAPS (11.0 months, log rank P = .34; figure not shown).
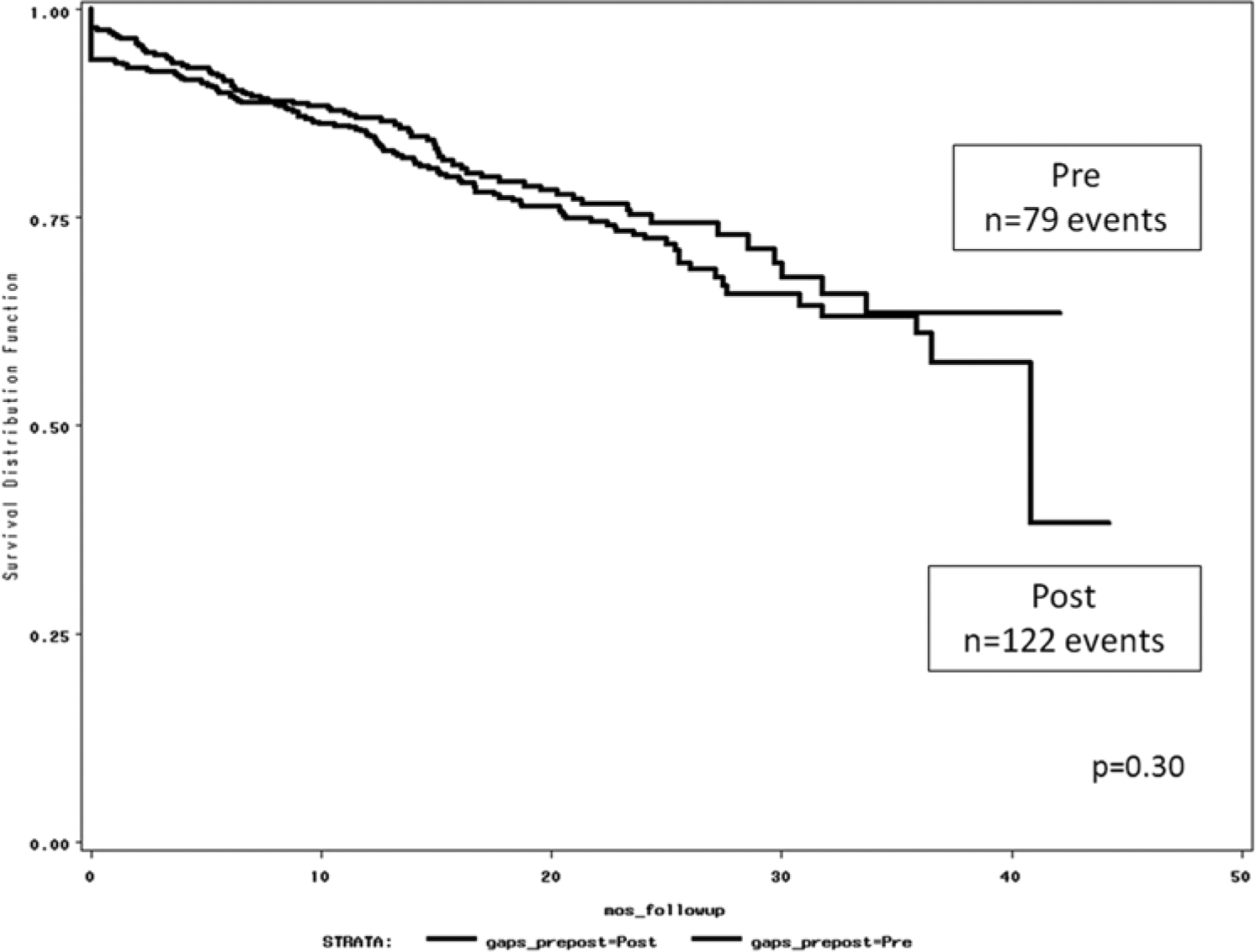
Historic cohort survival analysis: Kaplan–Meier curves for time to any mental health diagnosis during an outpatient visit pre-GAPS and post-GAPS (GAPS, Guidelines for Adolescent Preventive Services).
Discussion
This long-term analysis of the GAPS follows a prior implementation study that showed positive intermediate outcomes such as increased PCP discussion of risk behaviors. 12 While GAPS questionnaires elicit areas of adolescent risk and strength and help the PCP decide about follow-up, they did not increase detection or lead to earlier diagnosis of MH in this setting.
This study is unique in that it tests what we thought the GAPS should be doing in our primary care setting. As a surveillance tool, we expected the GAPS to be the first step in a process that detects risk behaviors and thereby facilitates detection of MH disorders. This is especially true for depression because of the 3 GAPS questions that specifically relate to depressed mood, anhedonia, and suicidality. While the comprehensive nature of the GAPS is appealing to PCP, its use was not associated with a significant change in trend or time to any MH diagnosis. More specific screening tools for MH may be needed for earlier identification and diagnosis. 11 While the GAPS may increase recognition, PCP recognition may be a necessary, but not sufficient step, in shortening the time to diagnosis and therefore treatment. So the problem may not reside with the GAPS questionnaire itself or its administration, but rather with the subsequent steps needed to make an MH diagnosis in this setting
The finding that the time to any MH or mood disorder diagnosis was similar pre- and post-GAPS, suggests that the mechanisms for acquiring an MH diagnosis may depend on subsequent steps of referral and accessing MH services. The paucity of MH professionals in rural areas may also limit diagnosis.
Psychiatric hospitalization and MH diagnoses or treatment delivered outside our rural network, are not captured in this study’s databases. However, if diagnosed elsewhere, an adolescent’s MH diagnosis is likely to be listed in subsequent primary care visits because follow-up usually takes place in primary care. This is particularly true if medication is required because in the study area, the PCP is often asked to continue prescribing psychiatric medications.
Adolescents with serious and/or acute MH problems may be less likely to come to clinic for annual visits and may be more likely to present acutely. Our study included MH diagnoses made in all our network’s outpatient facilities as well as its 3 emergency departments because these are included in our administrative database. However, this database does not capture ED visits made outside of the network.
The lack of increase in MH diagnoses raises several questions. Could the GAPS be facilitating discussion, early prevention or treatment of MH issues by the PCP? 15 If not, what comprehensive screening tools or MH-specific screeners trigger the steps needed to facilitate MH diagnosis? What steps are needed to shorten the time to diagnosis of MH disorders in primary care settings? These questions require more in-depth study.
Although screening tools specific to depression have been validated in terms of their psychometric properties, like the PHQ-2, 9 it is unknown whether use of such depression screeners in primary care settings shortens time to diagnosis or leads to more timely treatment of adolescent depression long term. While screening has been shown to increase detection in high-risk populations, for example, children in foster care, 16 the long-term outcomes of screening in primary care settings have not been clearly defined in the current literature. In some studies, screening increases MH referral and receipt of care, whereas in other studies, it does not. 17 The screening process may not improve patient outcomes in terms of receipt of services and access to MH care. Other factors, such as patient confidentiality, engagement, disclosure, and PCP use of screening results, may thwart the translation of the screening process into effective MH management. A recent systematic review of universal mental health screening in pediatric primary care provides an in-depth discussion of these factors operative in primary care settings 17 that may affect outcomes. The future evaluation of tools for mental health screening in primary care practice should stem from findings of recent reviews that highlight key areas for research.5,17
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was partially funded as a pilot study by the Center for Mental Health Services in Pediatric Primary Care (L. Wissow, NIMH grant P20 MH086048).