
Abstract
Introduction
Mental health problems in Australia are common, with one in five Australians (approximately 4.2 million people) experiencing a mental health condition per year. 1 While prevalence rates are similar for people in different parts of the country, mental health outcomes are notably poorer for those living in rural and remote settings.2,3 For instance, premature mortality that can be attributed to mental illness in rural and remote communities is about twice the rate compared to those in regional and metropolitan areas. 4 There is need for more comprehensive mental health support that is tailored to the unique needs of these communities. This has been recognised by the 2022-2032 Australian mental health workforce strategy, which seeks to address existing disparities, reduce premature mortality and establish a holistic culture of well-being across rural and remote Australia. 5
Implementing successful and sustainable change requires a good understanding of the local context and of barriers and enablers to effective practice. 6 There has been extensive research on the factors shaping access and use of mental health services in rural and remote areas and so inform policy to reduce inequalities. 7 However, there has been limited exploration of this within the context of general practice in Australia. 8 General practitioners (GPs) and other practice staff, such as practice nurses, play an important role in delivering and supporting mental health care within communities. 5 With almost 90% of Australian adults visiting a GP at least once a year and people talking to their GP about mental health more than any other issue, general practice staff will have unique insights into the factors that contribute to inequalities among rural and remote individuals with mental illness. 9 Existing work has tended to focus on physicians’ views on delivering mental health care in rural and remote general practice, 10 and there is a lack of research that has considered the perspective of a wider range of GP practice staff involved in service delivery, such as receptionists and practice managers. 11
This study aimed to contribute to closing this important evidence gap by comprehensively investigating multiple perspectives, including nurses, receptionists, practice managers, and GPs, to better understand the barriers and facilitators of providing mental health care in rural general practices across Australia.
Methods
This phenomenological study was part of a project that sought to develop a lived experience peer support intervention for mental health service users in rural general practices in Australia (trial registration: Australian New Zealand Clinical Trials Registry (ACTRN12623001189617; registered on 17 November 2023). 12 We conducted individual semi-structured interviews with general practice staff involved in the study, using the principles of experience-based co-design. We chose a descriptive qualitative methodology to enable a deeper understanding of the subject under study and provide researchers with insight into participants’ perspectives. 13 We followed the Consolidated Criteria for Reporting Qualitative Research (COREQ). 14
Study setting
Area information for each rural general practice.
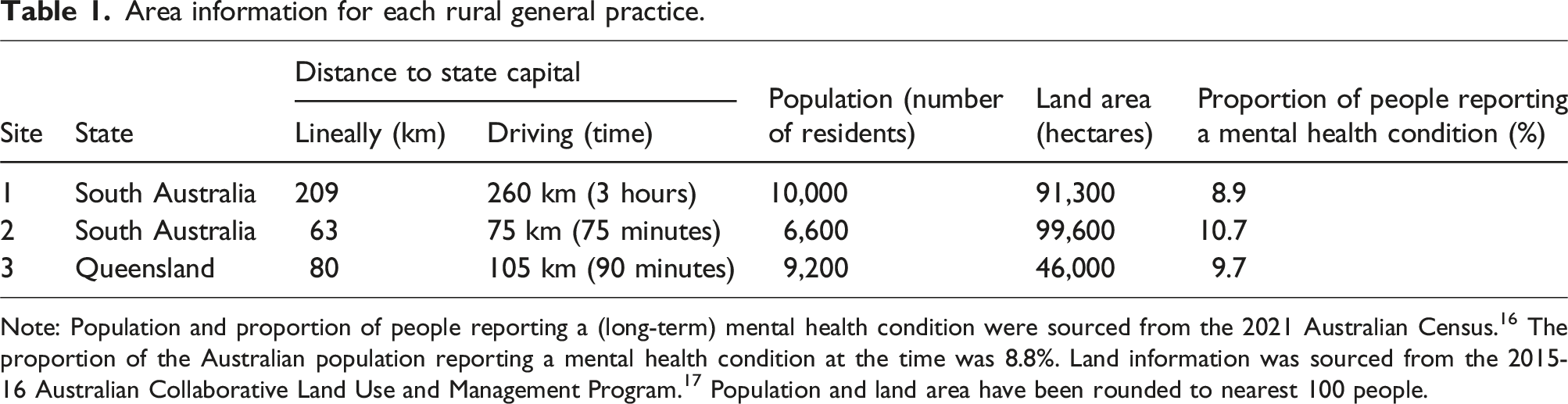
Note: Population and proportion of people reporting a (long-term) mental health condition were sourced from the 2021 Australian Census. 16 The proportion of the Australian population reporting a mental health condition at the time was 8.8%. Land information was sourced from the 2015-16 Australian Collaborative Land Use and Management Program. 17 Population and land area have been rounded to nearest 100 people.
Site 1 is in an inland river town, serving a region of 65.5% agricultural land, with the rest being mostly undeveloped or protected land and water (data current to 2016). 16 The site itself is in a concentrated urban area with 54.2% land use, but this rapidly decreases to 2.0% in the surrounding region. Site 2 is located on a southern peninsula of 72.9% agricultural land and 25.8% undeveloped or protected land and water. Site 3 is in an inland region of 51.5% agricultural land and 46.2% undeveloped or protected land and water. Urban intensive land use is minimal in the regions containing both Site 2 (1.1%) and Site 3 (2.1%).
Participants and recruitment
We used snowballing and purposive sampling to recruit practice nurses, practice managers, receptionists, and GPs at participating sites. Initially, the first author (BF) contacted the practice manager at each site who then identified willing and available staff from each of the practice roles. To the authors’ knowledge, no staff member declined participation after being approached by the practice manager. Identified staff were then contacted by BF via email, and provided with study details and a consent form. Practice managers were subsequently emailed to coordinate interview times. Each practice received a payment of $100 per staff member interviewed (up to $500 per practice) to compensate practices for the time staff took from their work hours. We planned to interview at least the practice manager, one GP, one receptionist, and one practice nurse from each practice, with recruitment continuing until data saturation was reached, indicating that no new information could be gathered. 18 We did not conduct pilot or repeat interviews. Informed written consent was obtained from all participants before commencing interviews, and verbal consent to participate and be recorded was obtained immediately before interviews began. While participants were offered the opportunity to review codes, themes and findings, only one opted to do so.
Data collection
We conducted individual semi-structured interviews using an interview guide informed by the Theoretical Domains Framework (TDF). 19 We initially devised one to two questions for each of the 14 TDF domains; in this paper, we primarily focus on data generated by three questions situated within the ‘Environmental context and resources’ domain of the TDF: (1) What gaps, if any, exist in assisting with or providing mental health care in your setting; (2) How do environmental factors, resources, or services either facilitate or impede the provision of mental health care support at your practice; and (3) What factors serve as enablers or barriers in providing mental health support to patients, making it either easier or more challenging.
All interviews were conducted by BF between June and September 2023 using video-conferencing software (Microsoft Teams classic, V1.6) at a mutually agreed time. Interviews used, a conversational tone and adhered generally to the sequence outlined in the interview guide; the interviewer took field notes. Probing and follow-up questions were incorporated as necessary, and additional questions were formulated when required. During the interviews, participants were mainly located at their workplace, choosing either quiet areas or private offices for the interviews to ensure participants would not be overheard.
Some participants were familiar to the interviewer who was also project officer for the broader project within which this study was situated. Interviews lasted from approximately 32 to 57 minutes (mean 45 minutes, standard deviation 7 minutes). Verbatim transcriptions of the audio recordings were generated using Otter.ai which provides real-time transcription using artificial intelligence 20 and subsequently cross-checked for accuracy.
Data analysis and rigour
The transcripts were thematically analysed using an inductive approach, following Braun and Clark’s six-step guide. 18 Initially, two authors (MR, BF) independently listened to the recordings and independently coded each interview. Codes were derived directly from the verbatim statements. One author (MR) then verified the generated codes for consistency, compiling them into a single master document. A coding tree is available upon request. Subsequently, both coders (MR and BF) independently analysed the data, consistently referring to the raw data to support identified ideas and themes. The labelling of themes and subthemes was deliberated between the two coders until mutual agreement was reached.
To enhance the rigour and trustworthiness of data analysis, we used comparative analysis between two researchers and ensured dependability by maintaining memos throughout data analysis to document analytical decisions and using direct quotes from participants to substantiate findings. 18 Investigator bias was mitigated by involving two researchers with different backgrounds (psychology and health) in data analysis. The draft themes were also discussed by the wider research team for the overarching project.
Ethics approval
Ethics approval for the study was granted by the Flinders University Human Research Ethics (HREC no. 6034).
Results
We interviewed 14 participants (four nurses, four GPs, three reception staff, and three practice managers). Practice managers, nurses, and reception staff were all female, while three of four GPs interviewed were male. This gender distribution is reflective of the typical staff composition within these rural general practices.
Identified themes and subthemes.
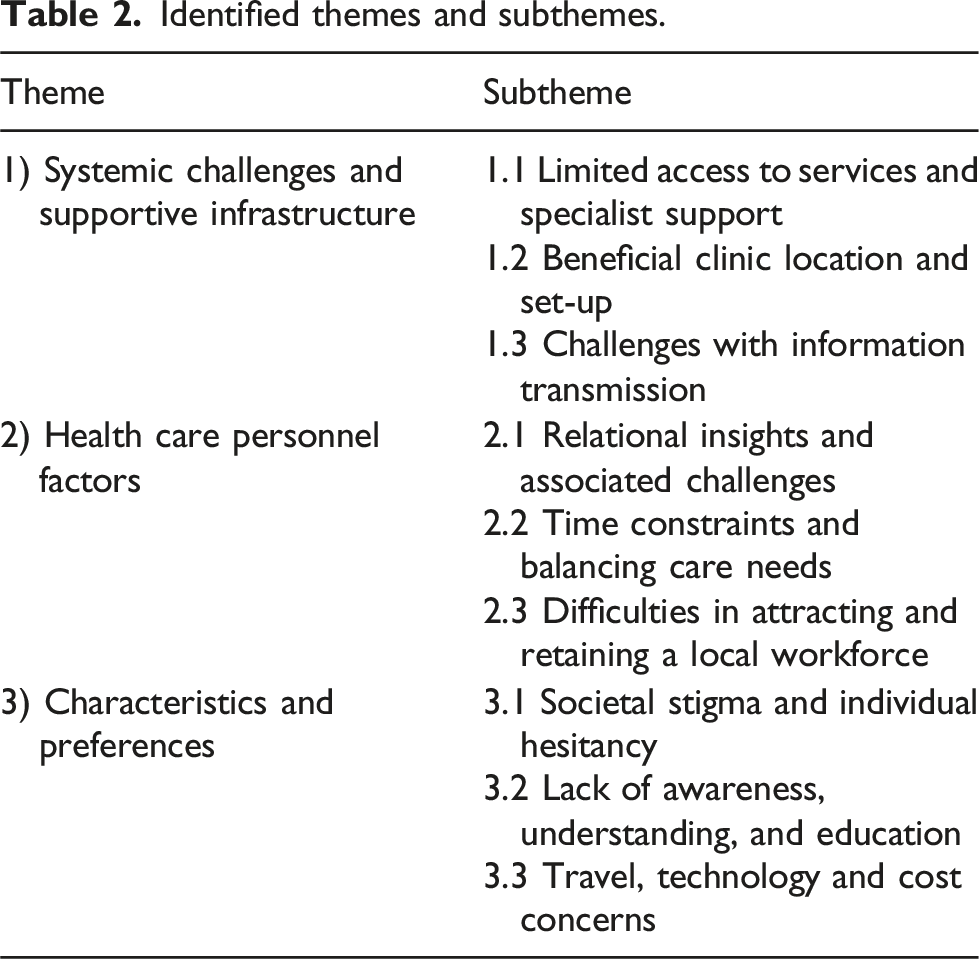
Systemic challenges and supportive infrastructure
Systemic and community enablers and barriers included limited access to services and specialist support; beneficial practice location and set-up; and challenges with information transmission.
Limited access to services and specialist support
All participants consistently emphasised the significant challenges with accessing mental health services in rural areas. They highlighted a scarcity of local resources, including a shortage of mental health-trained staff such as psychologists and psychiatrists, as well as specialised mental health teams and GPs trained in mental health. There was recognition of the value of visiting mental health specialists to address mental health service gaps, but visits tended to be infrequent (e.g., once a month or week), and participants highlighted difficulties in accommodating emergency cases due to scheduling constraints. This meant that patients had to wait to receive local care, required telehealth services, or were required to travel long distances (i.e., into cities) to access care, making these services untenable for those needing urgent care. The main gaps, in my experience is just access to psychological services, essentially. The waiting time always seems to be quite an issue... So, the patients come in [and] had to have a GP mental health plan, referred to a local psychologist or mental health facility, and then there’s, you know, quite a lengthy delay for an appointment… [It’s an issue because] quite often, you know, a lot of presentations to the GP are usually when they’re in quite a, not critical, but very vulnerable state, and they need that access to care quite urgently. (S05: Practice Manager)
Beneficial practice location and set-up
The proximity of the three study sites to the town centre was seen as advantageous, enabling easy access for patients who could walk to the facility, considering the limited public transport options in a country town. Most participants noted the practice setup and available resources as important enablers of mental health care delivery. The ability to provide private spaces, such as having a back entrance or access to a veranda or garden, was seen to be especially beneficial for people dealing with anxiety or seeking anonymity. Several staff also spoke about the value of having separate consultation rooms available to be used by mental health specialists to provide care, as private waiting rooms, or as space for urgent use if a patient needed to speak with a staff member. We have quite a few rooms here as well. So, I know we've got one patient, she suffers from anxiety quite a lot… she gets very overwhelmed in the waiting room. So, we offer her to sit in another room, and she really appreciates that. (S13: Receptionist)
Challenges with information transmission
Referral and communication processes within mental health care were frequently cited as challenging. Participants expressed frustration about poor communication from third-party providers, such as delays in receiving information about a patient or only receiving generic information. This was noted to be especially concerning where GP practices might not receive information about a patient’s emergency presentation for weeks, which was seen to undermine the continuity of care for both patients and staff. We don’t actually find out patient information from a lot of third parties… you send the referral, and often you don’t even get anything back to say, ‘we’ve received the referral there is this much of a waitlist’. Or sometimes we just get generic information from the third parties to say, ‘we’re accepting new patients, but it’ll be a six month wait’. (S01: Practice Manager)
One participant noted the positive experience of their practice’s referral relationship with local schools, which prioritise early intervention for mental health concerns, highlighting a valuable aspect of the community connection.
Health care personnel factors
Health care personnel factors included relational insights and the associated challenges; time constraints and balancing care needs; and difficulties in attracting and retaining a local workforce.
Relational insights and the associated challenges
Participants spoke about the advantages and drawbacks of providing care to patients in a small community. This was primarily viewed positively, emphasising the benefits of familiarity that come with seeing patients in the community, which can contribute to building strong rapport between health care staff and patients. This familiarity can also provide staff with observational insights, such as noticing subtle signs of patient distress. The close-knit community dynamics were also seen to enable a form of monitoring, where the pharmacist or police would be able to flag concerns for early intervention. At the same time, this intimate connection can pose challenges, as the emotional strain of knowing patients well and wanting the best for them can lead to burnout and fatigue among staff, particularly GPs seeing numerous cases daily. In the country, we know our patients, we know their families, we see them in the streets, I see them at supermarkets, you know, you do community activities with a bunch of them half the time, you know, you genuinely care, you genuinely want the best for them… And there's a whole other emotional burden to that, you know, because you do know them so well, you do see them so much, and so when they go downhill, it affects you. (S10: GP)
Having people living in close proximity to each other can also be seen as a hindrance, as noted by one practice nurse: “I live 40 km away – I would not like to work in my hometown, so patients probably feel the same” (S07).
Time constraints and balancing care needs
Time constraints in the context of mental health service provision was a recurring theme discussed by participants, especially GPs and receptionists. There was recognition of the time needed to listen effectively to patients and understand their mental health issues, and GPs highlighted the difficulty of achieving this in an environment where appointments of an appropriate length may not be available in the short-term. They … tell you all about these things in their life and how stressed they are, and it cannot be sorted out in the 15-minute appointment… [but] if the patients don't feel like you’re listening then they feel their doctor doesn't care… I find it very difficult to balance this. Normally, if they come in with mental health… I listen [to] them, because, you know, if I don't listen, I might lose the opportunity for them to come back and talk to me again. So, I'd rather spend the time [with them and then]… apologise to the next patient [and say] “I'm sorry I'm running late”. (S03: GP)
Some GPs spoke about attempting to address the mental health concern within the 15-minute time slot, with the trade-off being that the patient might feel that the doctor is rushing them or does not care, which can critically undermine the doctor-patient relationship. Receptionists additionally spoke about prioritising quick responses to phone calls and ensuring patients feel that their needs were a priority for staff members, whether that be over the phone or in person at the clinic. However, these staff also acknowledged the struggle of finding time to adequately achieve this in general practice.
Difficulties in attracting and retaining a local workforce
The challenge of attracting and retaining specialised mental health professionals, such as social workers, psychologists and psychiatrists, was a recurring concern. This was, in part, attributed to the less appealing rural lifestyle compared to urban settings, with participants specifically highlighting limited resources and entertainment options in rural areas as preventing health care staff settling in rural and remote settings. Several participants pointed to the need for a long-standing GP presence to enable continuity and the effective delivery of primary mental health services, which patients often preferred over “a revolving door of junior doctors” (S06: GP). One GP described how not having this continuity could potentially cause a patient to discontinue care: “the person has to tell their story again … and again and again and again, like- this might be the jumping off point” (S03).
However, this also means that senior doctors who remain in the community will have assumed significant responsibility for mental health patients to maintain continuity of care. While these GPs welcomed this responsibility, it meant that patients requiring urgent care might not always see their primary GP, as they could be fully booked months in advance. I think the hard thing is and is probably the way it works in the country, at least up here, is there's probably a couple of GPs in each practice that are booked out. I think I'm booked out for four months and so is another colleague, and then we’ve got other doctors that you could see next week, it’s not because they are not good doctors, it's just they're newer to the area. So, everyone's sort of, well, if this doctor stays, I'm going to see them… they tend to want to see someone that they know is going to stay. (S06: GP)
Patient characteristics and preferences
We identified three subthemes relating to factors at the patient level that were seen to shape the provision of primary mental health care in rural areas: societal stigma and individual hesitancy; lack of awareness, understanding, and education; and travel, technology, and cost concerns.
Societal stigma and individual hesitancy
Many participants highlighted mental health being seen as a ‘taboo’ subject in small communities, increasing vulnerability and, ultimately, affecting patient engagement. One participant noted that residing in a close-knit community may exacerbate a fear of being recognised, particularly due to the stigma associated with mental health. Yet, despite potential concerns, practice managers and nurses found that most patients were comfortable disclosing their mental health appointments, with one receptionist noting a perceived shift towards greater openness within the community towards mental health in recent years. Like, people are quite happy to tell you that they need to see him for mental health … I’ve noticed a huge difference, like probably in the last five years, … where prior to that they would never say to you “I need the appointment for mental health.” Or even speak to you about it at the desk … I think it’s what with society now it’s way more accepted and out there in the general public. (S14: Receptionist)
It was also noted that some patients may avoid seeking help due to perceived fears around involuntary hospitalisation and psychiatric treatment. Participants highlighted that older patients tended to be reluctant to seek mental health care, relating this to perceived stigma of mental health and potentially not even recognising their own struggles. Farmers and men were highlighted as specific groups reluctant to seek mental health support, which was commonly attributed to being “…stubborn and … ashamed” (S13: Receptionist).
Lack of awareness and understanding
Study participants also noted a lack of awareness, understanding, and education within rural communities around accessing mental health care. A significant issue that was highlighted was perceived confusion and misunderstanding around appointment times, with patients booking standard appointment slots for discussing their mental health concerns, creating challenges for GPs as discussed above. People do not understand the difference between a 15-minute appointment and a mental health appointment that might take an hour. (S02: Practice Nurse)
Additionally, interviewed staff cited uncertainty among the public about the pathways to accessing mental health care, including limited awareness of additional support beyond GP appointments. GPs emphasised the importance of educating the public in how to navigate the health care system, and how critical mental health plans are in improving access to mental health care.
Travel, technology and cost concerns
There was discussion of how travel, technology, and costs influenced patients to seek support. It was noted that many patients strongly preferred local services and were less willing to journey outside their area. While telehealth was seen to be an option, reluctance of patients to engage, technological barriers, and costs were cited as common barriers to access. However, as explained by one participant, even patients willing to travel to the city may struggle to find someone “who doesn’t have their books closed” (S06: GP). People don’t really want to travel but also don’t really want to do telehealth, which makes it all very hard… the telehealth services may be really good, but… often the actual telehealth is a barrier, either from a user's point of view and not being a tech savvy or just not wanting to do it. (S06: GP)
Costs associated with travel, along with service costs were frequently cited as additional barriers. While GP appointments are usually completely or at least partially covered by public health insurance, specialist services often incur out-of-pocket costs, although (some) patients may be happy to pay the fee to get the help they need.
Discussion
This study investigated the barriers and enablers to delivering mental health care at three rural general practices in Australia from the perspective of multiple clinic staff. We identified a range of factors shaping access and utilisation of mental health services in these areas, including individual, health care, and system/infrastructure factors. We discuss these factors alongside our proposed recommendations to improve the delivery of mental health care in rural regions.
At the system/infrastructure level, significant barriers to providing mental health care in rural primary care included limited access to services and challenges with information transmission, a finding that aligns with previous work on barriers and facilitators to accessing and utilising mental health services across regional, rural, and remote Australia. 7 Other studies involving GPs have also highlighted the critical role of consistent information sharing and collaborative care in improving access to mental health services. 8 However, our study identified additional challenges attributable to the compartmentalised nature of health systems and professionals, indicating a need for improved communication infrastructure between care providers. 21 This need was recognised by Australia’s national mental health workforce strategy, calling for integration of the workforce and care pathways across multiple settings. 5 Having visiting mental health specialists may be one potential solution, offering timely access to services and potentially alleviating information transmission challenges if general practice clinics adopt a one-stop-shop model for comprehensive care. Yet, as we also show, logistical challenges persist as highlighted by infrequent mental health specialist visits despite GP practices’ structural capacity to accommodate them. This may point to potential difficulties in attracting a mental health specialist, contributing to the systemic issue of limited services. While several government-supported programmes have sought to incentivise trainees to work in rural areas such as through the National Rural Generalist Pathway, these rotations typically last between 8 and 12 weeks, at which point the trainee moves on. 22 To support more sustainable retention in those areas, funding has recently been introduced for Australian universities 23 to offer medical degrees conducted solely in rural areas.5,21
The dynamics of general practice in rural settings offer opportunities and challenges for delivering mental health support. We show that familiarity and tight-knit community connections can facilitate rapport-building and early intervention; yet, they can also lead to emotional burnout and fatigue among staff. This creates unique relational dynamics and workload pressures for health care professionals working in rural areas. 24 Time has previously been identified as an important factor in mental health consultations, 25 and our findings point to the challenges faced by general practices to allocate sufficient time for mental health appointments, highlighting the need for better scheduling of appointments. Better integration of mental health services into primary care as envisaged by the Mental Health Workforce Strategy could help relieve pressures on general practice. 5 Involving workers with lived experience (peers) has been shown to be beneficial in secondary and tertiary mental health care, 26 and although promising models do exist, 12 this approach has yet to be strategically integrated into primary care in Australia.
When discussing challenges, societal stigma and lack of awareness were identified as significant barriers to seeking mental health care in rural and remote settings.7,8 Stigma and social embarrassment were particularly prominent, with staff further highlighting issues around self-reliance and stoicism, which they described as ‘stubbornness’. Although efforts are being invested in reducing stigma around mental health in Australia, 27 it remains a substantial barrier to accessing mental health services in rural areas. Study participants also noted that patients often find it challenging to navigate the health care system, which may be due to lack of understanding of and familiarity with available services. 7 There is a need for better community education on system navigation, mental health awareness initiatives to reduce stigma, and improved access to digital resources. Several reforms are currently being planned and implemented within the Australian health care system, including mental health centres that are specifically tasked with helping people to navigate the mental health system and provide free mental health services. 28
Perhaps not surprisingly, geographical distance was noted as a further barrier to mental health services in rural settings. Telehealth was seen as one potential solution, and while this was embraced by some patients, there was a perception among study participants that many more patients expressed discomfort or dislike for using telehealth. Previous research has found that some people struggle to build trust and rapport through telehealth, impacting the therapeutic value of the encounter. 29 GP educators have also raised concerns that prioritising and wider access through telehealth may compromise the relationship-centred care that is a fundamental part of primary care. 30 Additional concerns relate to limited access to digital technology and infrastructure, which makes telehealth either unsuitable or inaccessible for some patients, particularly in rural and remote regions. 31 Telehealth with service providers located in metropolitan areas is also limited by the lack of local knowledge and context, meaning some advice and supports may not be relevant or available to those in regional and rural areas. Flexible combination of in-person and telehealth mental health services depending on availability may most appropriately meet these diverse needs. While the recruitment and retention of primary care and mental health professionals in rural regions should remain a priority, mental telehealth care should also be made more accessible, without losing sight of service user preferences. 5
Strengths and limitations
Our study included diverse settings and perspectives from people working in rural and remote general practice. The consistency of findings across participants with various roles and three clinics spanning two Australian states highlights the robustness of the results. We did not use a specific framework to inform this work. While the interview guide was guided by the Theoretical Domains Framework, topics to be discussed were designed to more broadly explore staff members’ professional roles in delivering mental health care, alongside the barriers and enablers they perceived.
Conclusion
This study offers valuable insights into the multifaceted barriers to and enablers of delivering mental health care in rural general practice in Australia. We identified individual challenges such as societal stigma, lack of awareness, travel, technology, and cost concerns, as well as health care-related issues including relational dynamics, time constraints, and difficulties in attracting and retaining a local workforce. System and infrastructure elements included limited access to services and specialist support, clinic location and set-up, and challenges with information transmission. Addressing these barriers will require a comprehensive, multi-sectoral approach that addresses workforce shortages, improves infrastructure and resource allocation, addresses stigma and awareness gaps, and enhances access to care through innovative service delivery models.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Authors SM and PW are members of the Project Reference Group for the overarching project for which data for this article was produced, and are also part-time GPs at two of the general practice clinics involved in this article. Author SM was interviewed as part of this study in the process of co-design. SM's authorship relates to the substantial combined efforts of designing/executing the research study and writing of this manuscript. SM had no involvement in the analysis of data but was invited to review the de-identified result section of the paper, leading to the correction of a quote’s wording.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by a peer-reviewed grant from the Australian National Health and Medical Research Council, Medical Research Future Fund—Consumer-Led Round (2022527). Investigators report progress to the funding body, which has no significant role in the design of the study and collection, analysis, or interpretation of data nor in writing the manuscript.