
Abstract
Background:
The re-emergence of monkeypox (mpox) has triggered a global alert and galvanized efforts toward a scientific reappraisal of the disease.
Aim:
This study aims to provide a review of the use of Artificial Intelligence (AI) and novel vaccines in reducing the burden of mpox.
Methodology:
A narrative review was conducted according to Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines through electronic databases including PubMed, Google Scholar, ResearchGate, and Web of Science (WOS), using keywords such as Mpox, machine learning, deep learning, diagnosis and novel vaccines between the last 5 years (2019-2024). Included studies comprised clinical trials, cross-sectional studies, systematic reviews, meta-analyses, case reports, and case series written in the English language.
Result:
The diagnosis of mpox has been greatly aided by the use of AI, including machine learning (ML), deep learning (DL), artificial neural network (ANN), convolutional neural network (CNN), and transfer learning (TL). AI can help with the development of novel diagnostic tests, increasing the accuracy and speed of mpox detection, which is critical for successful epidemic management. Reported model accuracies for mpox lesion classification and disease trend prediction ranged from 83 to 99.8%, underscoring the high potential of AI-based tools in this field. Vaccines developed against smallpox, such as ACAM2000, LC16m8, and MVA-BN (JYNNEOS), have shown partial efficacy in preventing mpox transmission, providing cross-protection against mpox due to the genetic similarity between the 2 viruses.
Conclusion:
AI has proven to be significant in mpox detection, treatment, and prevention. Future directions should be focused on healthcare professionals to establish the validity and reliability of the models, a measure of the algorithm’s robustness, and the continuous auditing of AI systems.
Introduction
Mpox, formerly known as monkeypox, is a viral zoonotic disease caused by a dsDNA virus, Orthopoxvirus. In recent years, there has been an outbreak of mpox, especially by its IIb strain.1,2 The most affected region was the Democratic Republic of Congo (DRC), but recently, health emergencies have been declared regarding mpox in multiple countries around the world involving both Ib and IIb strains.1,2
Historical Overview
Mpox was first identified in 1958 in Denmark in laboratory animals and later confirmed in humans in 1970 in the Democratic Republic of Congo. The prevalence of mpox began to rise steadily following the eradication of smallpox. 3 As of August 2024, the World Health Organization (WHO) reported that mpox has been confirmed in over 120 countries, with more than 100 000 laboratory‑confirmed cases and over 220 deaths during the 2022 to 2024 global outbreak period. 4
Transmission of Mpox
Mpox is primarily transmitted through direct physical contact with an infected individual or via respiratory droplets during close face-to-face interactions, including speaking, breathing, or coughing. Documented cases have also implicated sexual transmission—particularly through practices such as oral and anal intercourse as a contributing route of spread. 2 In addition, indirect transmission via contaminated fomites and accidental needle-stick injuries has been reported. 5 Vertical transmission from mother to fetus has also been identified as a potential route, posing significant risks to both maternal and fetal health. 6 Following exposure, the incubation period typically ranges from 7 to 21 days, with clinical manifestations persisting for approximately 2 to 4 weeks, although duration may vary based on the host’s immune status. 7
Clinical Presentations of Mpox
The most distinctive, as well as the first to appear feature of this disease, is a rash starting from the face that makes a very evident clinical picture of mpox. 2 The rash is usually present at the site of transmission and then spreads to the whole body, including palms, soles, face, mouth, throat, genital areas, and anus.6 -8 Thus, signs of dysphasia, dysuria, and proctitis might also appear depending on the presence of a rash. Rash has a pattern of eruption from flat sores to itchy blisters to crusting and falling off. The Centre for Disease Control and Prevention (CDC) has classified its stages as macules, papules, and vesicles lasting for 2 days each, respectively. Followed by pustules and scabs, which last for 1 and 2 weeks, respectively. 8
Complications of mpox include superimposed bacterial infection, vision loss, and inflammation in multiple organs like the heart, rectum, organs, and urinary tract.2,6 Mpox should be considered as a differential in case of rash, as it resembles other skin and rash-forming infections.2,9 In light of the diagnostic challenges posed by the clinical similarity of mpox to other dermatological presentations, artificial intelligence (AI)-based diagnostic tools, especially image recognition systems trained on diverse and representative dermatological datasets, present a promising adjunct to traditional clinical methods. 5 AI-driven algorithms are capable of identifying lesion patterns, anatomical distributions, and associated symptom clusters, thereby enhancing early detection and diagnostic accuracy. 7 The integration of these AI tools into frontline healthcare settings has the potential to reduce diagnostic delays, optimize patient triage, and support more timely and effective public health interventions.
Diagnosis and Management of Mpox
While swab samples (eg, from skin lesions, oropharyngeal sites) can be effective for mpox diagnosis through molecular techniques such as polymerase chain reaction (PCR), serological detection of antibodies has shown limited utility in confirming active infection, particularly in the early stages of the disease. 4
Moreover, HIV testing is routinely advised in suspected mpox cases due to the heightened risk of severe disease progression and atypical clinical manifestations among immunocompromised individuals, particularly those with underlying HIV infection.4,10,11 The treatment goal of mpox involves the management of eruptions and support to prevent superinfection and complications. Moreover, Tecovirimat, also known as TPOXX, is FDA-approved for the treatment of mpox and other orthopoxvirus infections in the United States (U.S.). 12 Globally, it is available under emergency use authorizations in several countries, especially in regions experiencing outbreaks. Its mechanism of action involves inhibiting the p27 protein gene of the orthopoxvirus, which promotes recovery and prevents viral dissemination. 12 However, in December 2024, tecovirimat did not result in a statistically significant reduction in lesion resolution time or pain severity among adults with mild to moderate disease and low risk for severe complications. In light of these results, the clinical trial of this drug has been formally stopped. 12
Post-exposure prophylaxis can be done via vaccination within 4 days.2,6 Multiple trials and research are going on to explore the treatment and vaccination of mpox. Co-infection of mpox and HIV calls for ART on a priority basis. 2 Co-infection of mpox with HIV is relatively prevalent, with approximately 35 to 40% of Clade IIb mpox cases during the 2022 to 2023 global outbreak occurring in individuals living with HIV. 13 This co-infection has been associated with an increased risk of severe disease manifestations. Consequently, the prompt initiation of antiretroviral therapy (ART) is essential to mitigate immunosuppression, enhance host immune response, and reduce the likelihood of complications within this vulnerable population. 13
Where there is an emerging challenge in discovering therapy and prevention of mpox, the effective implementation of vaccination prophylaxis is also important. There is a lag in vaccine production, dissemination, and acceptance as well. In this era of technology, the help of AI can be taken to accelerate this process to eliminate the burden of disease. AI can assist in a better understanding of the cycle of pathogens, their infectivity, and their molecular as well as cellular mechanisms.10,11 Likewise, generative AI can also be used to eliminate vaccine hesitancy. 14 Therefore, keeping the current scenario in view, this study aims to provide a review of the use of AI and novel vaccines in reducing the burden of mpox.
Methodology and Materials
Study Design
A narrative review was conducted following the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) 2020 guidelines. Four electronic databases including PubMed, Google Scholar, ResearchGate, and Web of Science (WOS) to identify relevant studies from January 2019 to May 2024 The search strategy used Boolean operators combining the terms: (“monkeypox” OR “mpox”) AND (“artificial intelligence” OR “AI” OR “machine learning” OR “deep learning” OR “neural networks”) AND (“vaccine” OR “vaccines” OR “novel vaccine” OR “next-generation vaccine”) AND (“diagnosis” OR “detection” OR “identification” OR “diagnostic tools”).
Inclusion Criteria
This study included:
Peer-reviewed articles published in the English language carried out between 2019 and 2024
Eligible study designs included: clinical trials, systematic and narrative reviews, meta-analyses, observational research, case series, and case reports
Studies on the application of AI in the diagnosis, surveillance, or development of vaccines for mpox
Exclusion Criteria
Excluded from this study were
Studies not written in the English language. This is because of the difficulty in translation, which can create a bias, as some findings might be lost in translation.
Publications before 2019 were excluded to avoid outdated information.
Editorials, opinions, short communications, and conference abstracts without full abstracts.
Study Selection
A total of 1875 articles were identified through a literature search from databases, of which 794 articles were from Google Scholar, 545 articles from PubMed, 306 articles from ResearchGate, and 230 articles from Web of Science. See PRISMA Chart (Figure 1).

PRISMA flow chart.
Data Extraction and Analysis
Data extraction was performed independently by 2 reviewers using a structured and standardized template. Extracted variables included: first author, year of publication, study design, type of AI model utilized, primary diagnostic or predictive task, performance metrics (eg, accuracy, sensitivity, specificity), and noted methodological limitations.
Due to substantial heterogeneity in study designs, AI applications, and outcome measures, meta-analysis was not feasible. Therefore, a narrative synthesis was conducted to systematically present and compare the key findings across included studies.
Results
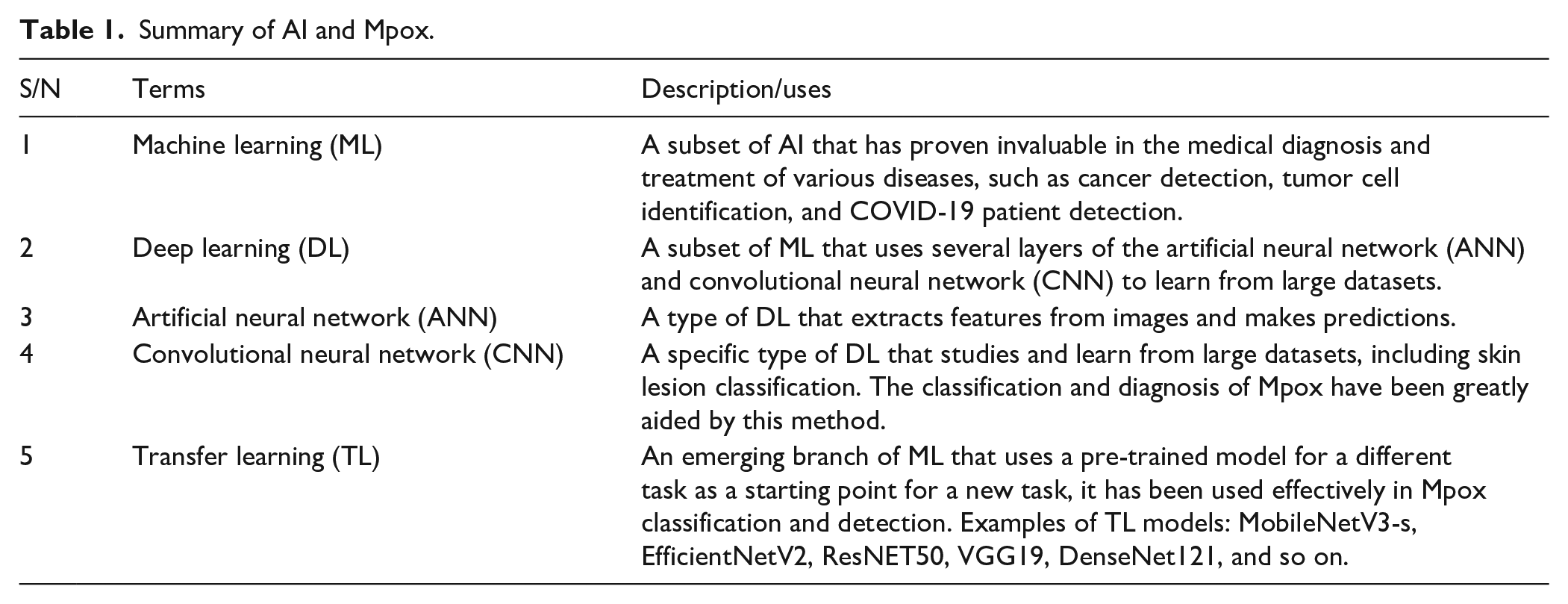
This study identified a total of 55 eligible studies that investigated the application of AI in the domains of mpox diagnosis, disease surveillance, and vaccine development. A majority of these studies utilized deep learning (DL) approaches, particularly convolutional neural networks (CNNs), with additional models incorporating transfer learning (TL) and ensemble techniques. Reported model accuracies for mpox lesion classification and disease trend prediction ranged from 83 to 99.8%, underscoring the high potential of AI-based tools in this field. For readers’ understanding, DL is a subset of ML that uses several layers of the artificial neural network (ANN) to extract features from images and make predictions. DL also employs convolutional neural networks (CNNs) to study and learn from large datasets. 2 CNNs have been successfully applied in various medical imaging applications, including skin lesion classification, breast cancer detection, and lung nodule detection. Transfer learning (TL) is an emerging branch of ML domains with demonstrated potential in various medical imaging and diagnostic fields. It uses a pre-trained model for a different task as a starting point for a new task.3,4
A recurrent limitation across the literature was the scarcity of real-world clinical datasets, which prompted many researchers to rely on publicly available image databases and social media-sourced data. These datasets were frequently augmented to enhance training robustness. However, despite the promising outcomes, critical challenges such as limited generalizability, lack of real-time clinical validation, interpretability of models, and dataset heterogeneity were consistently highlighted.
Furthermore, several studies5 -53 were reviewed to report the potential of AI in epidemic forecasting, enhancement of surveillance infrastructure, and streamlining vaccine candidate identification. Frequently referenced models included ResNet, MobileNet, Xception, and various customized CNN architectures, noted for their strong performance metrics and adaptability in image-based diagnostic tasks.
Discussion
AI in Mpox Diagnosis
In Murat et al. 6 TL models such as MobileNetV3-s, EfficientNetV2, ResNET50, VGG19, and DenseNet121 with CNN customized with hyperparameters were used to differentiate mpox skin lesions from similar skin disease lesions. The highest accuracy rate, with an F1-score of 97.8%, was achieved with the MobileNetV3 model. Sitaula and Shahi 7 also compared 13 different pre-trained DL models with the help of TL on the mpox dataset. With the aid of such a comparison using well-established evaluation measures, they identified the best-performing DL models to ensemble them for overall performance improvement. The evaluation result shows that the ensemble approach provides the highest performance with a precision of 85.44%, a recall of 85.47%, an F1-score of 85.40%, and an accuracy of 87.13% during the detection of the Mpox virus. Xception DL model provides the second-best performance with a precision of 85.01%, a recall of 85.14%, an F1-score of 85.02%, and an accuracy of 86.51%. 6
A study by Ahsan et al. 5 found a proposed modified Xception model that can distinguish patients with Mpox symptoms from others with accuracy ranging from 75 to 88%. On the other hand, ResNet101 demonstrated the best performance for multiclass classification, with accuracy ranging from 84 to 99%. 4 A study by Shrimali and Shrimali 8 concluded that ResNet50 is more accurate than VGG-19 and MobileNetV2, with an overall accuracy of 95%. Jaradat et al. 3 found the training accuracy of 99.9% at epoch 9 for VGG16, 65.2% at epoch 13 for EfficientNetB3, 98.4% at epoch 12 for VGG19, 99.8% at epoch 14 for MobileNetV2, and 91.8% at epoch 14 for ResNet5. Moreover, Sahin et al. 10 presented a mobile system to automatically detect human Mpox skin lesions, where they trained a deep TL-based system using Mpox skin lesion database (MSLD) images. MobileNetv2 showed one of the best performances in terms of accuracy (91.11%), and it was then adapted into an Android mobile application that can easily detect Mpox lesions. 8
Ali et al. 11 achieved an accuracy of 83.59% with DenseNet121. Eliwa et al. 14 used the Grey Wolf Optimizer (GWO) strategy to enhance the performance of CNN models on similar tasks, achieving an accuracy of 95.3%, indicating the model’s ability to discriminate between positive and negative classes. Idroes et al. 15 integrated Xplainable DL and Grad-CAM with ResNet50v2, achieving an accuracy of 99.33%, precision of 99.34%, sensitivity of 99.33%, and F1-score of 99.32%. Soe et al. 16 found ResNet-18 and DenseNet-121 with the highest performance. ResNet-18 achieved 99% accuracy of Area Under Curve (AUC) and accuracy of 94.7%, while DenseNet-121 achieved an AUC of 98.2% and accuracy of 92.6%. Yue et al. 17 proposed an AI-mediated “Super Monitoring” (Mpox-AISM) model with precision, recall, specificity, and F1-score in diagnosing mpox reaching 99.3, 94.1, 99.9, and 96.6% respectively, while it achieved 94.51% accuracy in diagnosing mpox, 6 mpox-like skin disorders, and normal skin. In another study, Yue et al. 18 developed a second version of the Mpox-AISM, producing the highest accuracy of 98.40% and recall of 93.65% with Fast-MpoxNet.
Setegn and Dejene 19 recorded their best accuracy of 89.3% with LGBMClassifier. The proposed ensemble Mpox-XDE model by Saha et al. 20 outperformed all other DL models employed in their study, achieving a test accuracy, precision, recall, and F1-score of 98.7, 98.9, 98.8, and 98.8% respectively. Thieme et al. 21 in their study found 91% sensitivity, 89.8% specificity, and 96.6% AUC with the MPXV-CNN model. Tan et al. 22 adapted a digital symptom checker, which showed a specificity of 87% and sensitivity of 90% for symptomatic mpox.
A common similarity noted across all studies reported above was the utilization of publicly available data from various websites and social media apps due to the absence of clinical data. Augmentation of data was also common, including but not limited to flipping, zooming and color enhancement. One study reported a struggle with misclassifications between visually similar diseases, such as chickenpox and Mpox. 11 Tan et al. 18 also identified numerous hurdles with their symptom checker tool, including issues of data privacy and security for app users, initial lack of data to train the AI tool, and the potential generalizability of input data. Despite the excellent performances and the model’s potential to provide reliable and interpretable support for clinicians, particularly in settings with limited access to specialized diagnostics reported across the studies, further evaluation and validation of the models with larger and more diverse datasets to represent overall population and improve the model’s capacity to distinguish between similar conditions in real-world scenarios would be valuable to determine its capabilities and limitations. Such evaluations could assist in determining whether the model is suitable for use as a real-time diagnostic tool for Mpox in clinical settings or not (Table 1).
Summary of AI and Mpox.
AI in Mpox Surveillance
Hutchinson et al. 23 leveraged the EPIWATCH system to detect early trends in the 2022 Mpox outbreak in the United Kingdom (UK). 19 Their analysis found a spike in rash-like illness reports in May 2022, coinciding with the emergence of Mpox cases. Interestingly, most EPIWATCH reports came from Asia rather than Europe or North America, where widespread transmission was observed. EPIWATCH uses AI to continuously monitor open-source data across 52 languages, a task too large for manual review. While the public-facing dashboard is real-time, the open-source data remains unvalidated and intended to prompt further investigation, not replace conventional surveillance. 19 The study by Cuba et al. 24 utilized a time ensemble forecasting approach to accurately predict the cumulative confirmed mpox cases for the top 4 countries and globally. The 28-day forecasts provided insights into the disease’s spread and associated risks. While Brazil exhibited a gradual increase in cumulative cases, France and Spain saw only a temporary rise in the first 2 days, with no evidence of further spread within 26 days. In contrast, the cumulative cases in the USA gradually increased from 30 156 to 30 228 during the forecasted period.
Jena et al. 25 Please revise accordingly.]presented comprehensive and dynamic data on the mpox outbreak in Africa, revealing significant disparities in case numbers across different regions, with the DRC and Nigeria experiencing the highest rates of infection. Using autoregressive integrated moving average (ARIMA), the analysis of confirmed cases showed that DRC had the highest Root Mean Square Error (RMSE) and Mean Absolute Error (MAE), indicating more substantial deviations in forecast accuracy compared to other regions.
Conversely, Nigeria and South Africa exhibited lower errors across these metrics. For cumulative cases, the African continent demonstrated an RMSE of 1.60 and MAE of 0.921, while the DRC again exhibited higher error rates, with an RMSE of 26.78 and MAE of 17.24. These performance metrics reflect the varying levels of forecast accuracy for Mpox case predictions across different regions. 21 Charniga et al. 26 compared the predictive performance of the EpiNow2 model and a naïve Bayesian generalized linear model (GLM). Their results suggest that the EpiNow2 method exhibited lower probabilistic error compared to the GLM across all stages of the outbreak, except for the initial phase. 22
Ou et al. 27 developed an automated system for tracking diseases through sewage virus detection and an AI model to estimate mpox cases. Their findings showed a significant correlation between mpox levels in wastewater and reported mpox cases, validated by the AI model’s performance. The model’s predictions deviate by about 16.94% from actual values on average, demonstrating its robustness. The high R-squared value (0.87) indicates that the model captured a significant proportion of the data’s variance, and the low MAE and RMSE suggest the predictions closely align with actual values. 23 Another study by Iftikhar et al. 28 proposed a combination model using a Support Vector Machine (SVM) with a spline kernel that achieved lower mean errors compared to time series and other ML models. The final model, regression spline filter (RSF12), demonstrated high accuracy and efficiency in predicting daily cumulative confirmed cases of Mpox. 24
Additionally, in a separate study, Iftikhar et al. 29 reported that the Hodrick-Prescott filter (HPF11) model had the lowest errors among the models evaluated for forecasting cumulative new cases. 25 Specifically, the HPF11 model yielded MAPE, MAE, and RMSE values of 0.0547, 44.8904, and 63.3184, respectively. Furthermore, the HPF43 model was found to have the least model error compared to other existing models for predicting the cumulative death count, with MAPE, MAE, and RMSE values of 0.8538, 0.5427, and 0.8244, respectively. 25
Forecasting methods face limitations in accuracy and timeliness as outbreaks evolve and require substantial computational resources. Reporting biases and variable data quality across regions impact the reliability of forecasts.21 -23 Future research can optimize predictive models by incorporating more variables and enhancing parameters. AI-driven approaches offer new avenues, such as using hospital sewage monitoring to predict infections, which could enhance the efficiency and objectivity of epidemic surveillance and early warning systems.21 -23
AI in Mpox Vaccine Development
The utilization of artificial intelligence for early warning systems as an adjunct to conventional surveillance can significantly augment and facilitate the early development of biomedical solutions, thus meriting further research. 26 A study by Olawade et al. 31 delineated diverse AI techniques that facilitate vaccine development. These encompass ML algorithms, such as decision trees (DT) and random forests (RF), which assist in predicting antigenic epitopes, evaluating immunogenicity, and prioritizing antigens based on multifarious features. 27 Conversely, DL techniques are employed for sequence-based epitope prediction, protein folding prediction, and vaccine candidate identification. The Hidden Markov Models, which are probabilistic, are utilized to forecast B-cell and T-cell epitopes by capturing sequence motifs and structural patterns. 27
Neural networks (NN), including feedforward and recurrent neural networks (RNNs), are leveraged for epitope prediction, protein-protein interaction prediction and structure-based vaccine design. Generative models, such as variational autoencoders and generative adversarial networks, are employed for de novo immunogen design and generation of novel vaccine candidates. 27 Molecular dynamics examines immunogen conformational changes and predicts antigen-antibody interactions. Virtual screening sorts compound libraries for adjuvants and predicts interactions between adjuvants and immune receptors. Finally, structure-activity relationship models analyze the structure-function relationships of adjuvant molecules, guiding the rational design and optimization of adjuvant formulations. 27
A study by Martinez et al. 32 evaluated multiple ML approaches for 3 distinct tasks: predicting antigens, identifying T-cell epitopes, and classifying the reactivity of poxvirus epitopes. While various algorithms were scrutinized, the non-DL models did not surpass 70% accuracy. In contrast, DL models exhibited remarkable performance following hyperparameter optimization, achieving an impressive 95.95% accuracy in antigen prediction. Furthermore, the DL model was capable of distinguishing epitopes from non-epitopes with 93.14% accuracy. 28 An external validation process further corroborated the model’s capabilities, correctly classifying 73.75% of unseen epitope data. Additionally, the XGBoost classifier, after tuning, attained an accuracy of 82%. The researchers also reported the F1-score (87%) and AUC (91%) to assess the performance across different validation tasks. 28
Adel et al. 33 identified traditional ML methods, such as RF, SVM, gradient boosting, and logistic regression, as foundational approaches for tasks involving candidate ranking, epitope scoring, and logistic optimization. 29 Concurrently, advanced DL architectures, including CNN and RNN, demonstrate exceptional capabilities in pattern recognition and large-scale data mining, facilitating high-throughput (HTP) epitope discovery and the generation of novel immunogens using generative adversarial networks and variation autoencoders. 29 It is also important to note that numerous AI-based solutions for Mpox vaccine development remain in the pilot stage, and their real-world applicability is yet to be validated through comprehensive, large-scale clinical trials. 29
Advances in the Mpox Vaccine
While no vaccines have been specifically developed for mpox, those created for smallpox, such as ACAM2000, LC16m8, and MVA-BN (JYNNEOS), have shown partial efficacy in preventing mpox transmission, providing cross-protection against mpox due to the genetic similarity between the 2 viruses. 30 However, the effectiveness of this partial protection is incomplete, leading to continued human-to-human transmission during the 2022 to 2023 Mpox outbreak. 30 A summary of vaccine options and their details is shown in Table 2. The MVA-BN is an effective vaccine, considered safer than other options.31,32 Moreover, its 1 dose has been shown to produce similar effects as 2 doses, yet more research is needed to prove the hypothesis. 33 This vaccine is also indicated in children, pregnant and lactating women, as post-exposure prophylaxis. 34 Though it has been approved, definitive literature on the use of ACAM2000 as a prevention of mpox is scarce, which highlights a huge gap in mpox prevention research. 35 Moreover, it has been shown to have a range of side effects, ranging from mild to severe, especially having cardiac effects as well. 36 This limits the wide range of use of this vaccine in the prevention of mpox in high-risk areas. LC16m8 was administered among children infected with Mpox during the state of emergency in Congo, though more research is required to explore its safety, adverse effects and efficacy. 37
Comparison of Mpox Vaccines: Efficacy, Safety, and Recommended Dosage.

Though the current smallpox vaccines have demonstrated about 85% efficacy in preventing mpox in general, their long-term effectiveness and safety need further validation in diverse populations. 44 This calls for the need for targeted vaccine technologies that can more effectively address mpox-specific challenges, which include advancements in viral vector-based vaccines, recombinant protein vaccines, and nucleic acid-based vaccines, nanoparticle-based platforms, which are being actively researched. 30 Despite the progress in developing vaccines against mpox, hurdles including limited efficacy, safety concerns, and the need for further optimization to ensure widespread protection are still faced. The complexity of viral mutations and the need for more targeted vaccine responses also pose significant challenges. Thus, while AI offers promising tools to enhance mpox vaccine development and management, addressing these technological and data-related challenges remains crucial for advancing vaccine efficacy and accessibility. 45
Integration of AI and Vaccination of Mpox
The incorporation of AI into the current vaccination environment, particularly in the context of mpox, is a unique opportunity to improve vaccination tactics, increase effectiveness monitoring, and strengthen surveillance systems. AI’s skills can considerably improve the public health response to several infectious illnesses, including mpox, by improving different components of vaccination programs. It has the potential to dramatically improve the effectiveness and efficiency of vaccination efforts for infectious illnesses such as mpox.
Enhancing Vaccination Strategies With AI
AI may help with a variety of vaccination-related tasks, including enhancing vaccine access and optimizing distribution techniques. By integrating AI technology, public health professionals may analyze massive quantities of data to identify at-risk individuals, anticipate vaccine uptake, and customize communication campaigns to increase immunization rates. For example, AI-driven models may examine demographic data and historical vaccination trends to identify populations that may require focused outreach efforts, therefore increasing global vaccine coverage. 46
AI can also be used to improve the design and development of vaccinations themselves. Advanced ML algorithms may be used to predict immune responses to various vaccine formulations, speeding up the vaccine development process. This is especially important in the case of mpox, when the quick reaction to outbreaks is vital. AI approaches, such as DL, can help find prospective vaccine candidates by evaluating genetic sequences and predicting which antigens would elicit a robust immune response, as seen in the development of hypoallergenic vaccines.47,48 The use of AI in vaccine design not only reduces development time but also enhances the chance of developing effective vaccinations customized to specific virus strains.
Evaluating Vaccine Efficacy and Monitoring Through AI
Vaccine effectiveness can be considerably improved using AI-driven monitoring and assessment systems. AI technology may be used to track vaccination rates in real time, allowing health officials to immediately identify areas of poor uptake and undertake targeted treatments. For example, AI may scan data from a variety of sources, including electronic health records and social media, to assess public sentiment toward vaccination and uncover misinformation that may impede vaccine adoption. 46 This proactive strategy allows health professionals to swiftly address concerns and misconceptions, resulting in increased vaccination uptake.
Furthermore, AI can play an important role in post-vaccination monitoring. By evaluating health data, AI systems can detect adverse outcomes following vaccination more effectively than traditional techniques. This expertise is critical for guaranteeing vaccine safety and preserving public faith in immunization programs. AI algorithms may examine trends in health data and social media attitudes on vaccine uptake to identify probable side effects and their prevalence, enabling prompt answers to any safety issues that may develop. 49 The capacity to evaluate vaccine performance in real-time also allows for adaptive vaccination techniques, such as administering booster doses depending on emerging data on fading immunity or the appearance of new variants.
Challenges of Harnessing AI for Mpox Diagnosis and Control
1. Data Privacy and Security
Protecting patient information is critical, especially when handling sensitive health data. AI systems require access to large datasets, which raises concerns about potential data breaches and unauthorized access. Ensuring compliance with regulations such as HIPAA (Health Insurance Portability and Accountability Act) is essential to safeguard patient privacy. 50
2. Quality and Quantity of Data
The effectiveness of AI models depends heavily on the quality and quantity of the data used for training. In the case of mpox, there may not be enough high-quality, labelled datasets available for training AI algorithms. This data scarcity can result in models that lack the robustness to handle real-world variations in symptoms and disease presentations.47,50
3. Model Generalizability
AI models trained on specific datasets may struggle to generalize when applied to different populations or clinical settings. This limitation can lead to diagnostic errors, particularly in regions with varying demographic and epidemiological profiles. Ensuring AI models work effectively across diverse environments is a challenge. 50
4. Algorithm Bias
AI systems can inherit biases present in the data they are trained on, which may lead to disparities in diagnostic accuracy across various demographic groups. In the context of infectious diseases, where equitable healthcare access is critical, addressing bias in AI training datasets is essential to ensure fair and accurate diagnoses. 50
5. Integration into Healthcare Workflows
Incorporating AI tools into existing healthcare systems presents challenges. Healthcare professionals may be reluctant to adopt AI due to concerns about its reliability, the need for additional training, and the fear that AI may replace human judgment. Successful integration requires careful planning and change management strategies. 50
6. Regulatory and Ethical Challenges
The implementation of AI in healthcare is subject to strict regulatory oversight. Ensuring compliance with medical regulations and ethical standards can be a significant challenge for developers and healthcare providers. The rapid pace of AI advancements often outstrips existing regulatory frameworks, leading to uncertainty. 50
7. Multidisciplinary Collaboration
Effective AI implementation requires collaboration between various stakeholders, including data scientists, healthcare professionals, and policymakers. Poor communication and a lack of collaboration can hinder progress and lead to suboptimal outcomes. 50
8. Real-Time Diagnosis Limitations
AI has the potential for real-time diagnosis, but technical limitations, such as processing speed and the need for reliable internet connectivity, can slow down decision-making in clinical settings. Ensuring AI systems can operate efficiently in diverse environments is critical. 47
9. Interpretability of AI Decisions
Many AI models, especially deep learning algorithms, function as “black boxes,” making it difficult for clinicians to understand how diagnoses are made. This lack of transparency can reduce trust in AI systems, hindering their acceptance and integration into healthcare practices.51 -53
10. Continuous Learning and Adaptation
AI systems must be updated regularly with new data to stay relevant. However, the rapidly changing nature of diseases like mpox, with new variants and symptoms emerging, complicates this process. Establishing systems for ongoing learning and adaptation is vital for maintaining the effectiveness of AI tools. 50
11. Technical Challenges
The development and deployment of AI systems often require significant computational power and advanced algorithms. These technical requirements may not be feasible in all healthcare settings, particularly in low-resource environments. 50
12. Trust and Acceptance
For AI systems to be successfully adopted, healthcare professionals and patients must trust them. Concerns about the accuracy of AI diagnoses and potential errors can lead to skepticism. Building trust through transparency and reliability is crucial for widespread adoption. 50
13. Implementation Costs
Developing and implementing AI systems can be expensive, requiring substantial investment in technology, training, and infrastructure. This financial burden may be a barrier for many healthcare organizations, particularly those operating in resource-limited settings. 50
14. Ethical Implications
The use of AI in healthcare raises important ethical questions regarding accountability and responsibility for diagnostic errors. Determining who is liable when an AI system makes a mistake is a complex issue that requires thoughtful consideration. 50
15. Public Perception and Misinformation
Public understanding of AI in healthcare can be shaped by misinformation and fear. It is essential to address misconceptions and educate the public on the benefits and limitations of AI to foster acceptance and trust in these technologies. 50
Future Directions for Mpox Eradication
The potential to devise a method to rapidly and accurately classify available mpox genomes by applying innovative AI technologies such as ML and DL to the genetic signatures identified in the genomes is seen. It is possible to use artificial neural networks (ANN) and ontology-based side effect prediction frameworks to evaluate the side effects of any type of drug or formulation that may be used for the treatment of Mpox. 52
A forecast for a secure cloud-based system for comprehensive mpox management is also seen, where patient data, wearable devices, smartphone data, and AI models can be deployed on the cloud to enable access to healthcare professionals to enhance remote mpox diagnosis. The incorporation of clinical, laboratory, epidemiological, demographic, and other parameters to allow system-wide analysis for healthcare resource allocation is also important. 46
To minimize the further spread of mpox, teleconsultation via remote video conferencing can also be integrated by various healthcare institutions into their healthcare systems, and appropriate symptomatic treatment can be dispensed remotely for mild cases. Explainable artificial intelligence (XAI) methods such as Shapley additive explanation, LIME, Eli5, and QLattice can be incorporated by researchers and clinicians to enhance the interpretability of the model outputs, which will help to better understand the model predictions using different visualizations. 46
Furthermore, mpox eradication is possible with the unfolding of AI models, which encompass a rapid understanding of infection biology, early warning of outbreaks, contact tracing, acceleration of diagnostic development, drug discovery, and the facilitation of drug design.16,21,53 -56 Rapid progress on all fronts to make progress on surveillance, monitoring, prevention, and treatment at the same time to eradicate the disease is imperative. A focus on mpox will be a step forward, as the second outbreak has already occurred in recent times. 52
More reliable polynomial neural networks should be trained by AI developers to develop a predictive model that could forecast Mpox cases developing in countries over the next decade to facilitate its eradication. 57 Also, interdisciplinary efforts among AI developers and healthcare professionals are paramount; as a result, medical validation of AI models must be performed by healthcare professionals to establish the validity and reliability of the models, measure the algorithm’s robustness, and ensure the continuous auditing of AI systems. 46 Figure 2.

Future directions for mpox eradication.
Study Limitations
Despite the clinical and public health importance of this study, unfortunately, limited clinical and field data on AI and vaccines on mpox were found. Also, this study covered literature up to 2024; the final inclusion of 55 studies (versus higher counts in related reviews) reflects the strict criteria applied to ensure methodological quality, clinical relevance, and a specific focus on AI-based applications in mpox control. Further clinical and epidemiological studies, including meta-analyses, should be conducted by researchers on this topic to overcome these limitations.
Conclusion
This study found that the use of AI tools has proven to be significant in mpox detection, treatment, and prevention. Also, there are advancements in mpox vaccine development, the integration of AI in mpox vaccination and challenges, future directions regarding AI innovations, strategies for disease eradication, and collaboration between AI developers and healthcare workers. The documented kinds of literature provide evidence-based methods that the eradication of mpox is possible with the help of AI.
Footnotes
Author’s Note
Excel Onajite Ernest-Okonofua is now affiliated to Igbinedion University, Okada, Edo State, Nigeria.
Author Contributions
All authors made substantial contributions to this study.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Transparency Statement
All the authors have approved the submitted version and have agreed both to be personally accountable for their contributions and to ensure that questions related to the accuracy or integrity of any part of the work, even ones in which they are not personally involved, are appropriately investigated, resolved, and the resolution documented in the literature.