
Abstract
Background:
Asthma and COPD are among the most prevalent chronic respiratory conditions, with inhalers as their primary pharmacological treatment. In the UK, metered-dose inhalers (MDIs) account for 70% of all inhaler prescriptions and contribute significantly to the NHS’s carbon footprint, making green prescribing a critical focus. Aligning environmental sustainability with clinical excellence is essential to reducing exacerbations and deaths while minimising carbon emissions.
Objective:
This initiative aimed to assess the localised impact of a structured quality improvement program designed to enhance respiratory care and integrate sustainable prescribing practices. Specifically, it sought to evaluate prescribing patterns, respiratory review completion rates, and the feasibility of transitioning patients from MDIs to lower-carbon alternatives whilst maintaining clinical outcomes.
Methods:
The initiative, implemented at a UK general practice in January 2020, focussed on staff education, restructuring respiratory consultations, and patient engagement. The “treatable traits” paradigm and best practice frameworks guided the program to optimise individualised care. Prescribing data, in-date respiratory review rates, and estimated carbon emissions were analysed over 4 years (2020-2024) using publicly available sources such as OpenPrescribing.net. While education was a component of the intervention, no formal assessment was conducted on its direct impact on prescribing behaviours.
Results:
The practice achieved an in-date respiratory review rate exceeding 90%, rising to over 96% during the most recent QOF period. Over 4 years, the proportion of non-salbutamol MDI prescriptions decreased from 62.9% to 36.2%, aligning with national sustainability goals. Despite growth in the practice population, overall carbon emissions from inhalers were successfully reduced, reflecting a shift towards lower-carbon prescribing.
Conclusion:
This initiative illustrates the feasibility of integrating sustainable prescribing practices into routine respiratory care, aligning with the goals of the national health system. This work highlights the potential of local-level interventions to contribute to broader sustainability efforts in respiratory medicine. Improvements in prescribing patterns and review rates have been noted, but more research is needed to evaluate the impact of educational interventions on healthcare providers’ and patients’ decisions. Future initiatives should focus on structured evaluations of long-term adherence and clinical outcomes.
Introduction
Chronic respiratory diseases are a significant global health burden, contributing to high morbidity and mortality, with 4 million premature deaths annually. 1 Asthma and chronic obstructive pulmonary disease (COPD) remain the 2 most prevalent conditions requiring long-term management.1,2 In the UK, 5.4 million people receive asthma treatment, while COPD remains a leading cause of mortality, with its prevalence increasing in ageing populations.2,3 Despite their differences, both diseases share the common treatment goal of reducing exacerbations to improve patient outcomes.1,2,4
Inhalers are the primary pharmacological treatment for asthma and COPD, with metered-dose inhalers (MDIs) making up 70% of UK prescriptions.2,5 However, MDIs rely on hydrofluorocarbons (HFCs) as propellants, potent greenhouse gases contributing significantly to healthcare-related carbon emissions. A single salbutamol MDI releases greenhouse gases equivalent to driving 175 miles (280 km), with a carbon footprint ranging from 20 to 80 kgCO2e, while a comparable DPI emits the equivalent of just 4 miles (6 km), with a carbon footprint ranging from 1.5 to 6 kgCO2e.2,6,7 With MDIs contributing significantly to healthcare emissions, the Kigali Amendment to the Montreal Protocol mandates the phased elimination of HFCs, reinforcing the urgency for sustainable prescribing practices.5 -7
The UK’s National Health Service (NHS) attributes 13% of its carbon footprint to MDI use, making inhaler sustainability a priority in achieving carbon neutrality by 2040.5,8 In response, the NHS has set a goal to reduce MDI prescriptions by 50% by 2028, emphasising the transition to lower-carbon alternatives such as dry-powder inhalers (DPIs). 2
While DPIs are a viable alternative for most patients over 5 years old, MDIs with spacers remain essential for younger children due to lower inspiratory effort. 2 However, sustainability efforts must go beyond inhaler selection. Reducing excessive reliance on short-acting beta-2 agonists (SABAs) and establishing an appropriate preventer regime is critical to providing optimal clinical management whilst mitigating environmental impact. 6 Overuse of SABAs - defined as requiring more than 4 inhalers per year - substantially increases exacerbation risks while amplifying emissions. 6 Equally, ensuring that patients receive and adhere to preventer therapy reduces the number of rescue inhalers used and enhances disease control.2,6
To achieve these goals, a holistic approach is required, incorporating proactive prevention strategies and the “treatable traits” paradigm. 9 This model, first proposed by Gibson et al, 10 focusses on addressing airway, behavioural, comorbid, and risk factor traits to enhance respiratory control.9,11 Implementing this framework requires a structured approach that ensures “the right treatment (at the right time), for the right patient, in the right formulation, for the right duration.” 12 Personalised prescribing, informed by patient preferences and clinical suitability, optimises both treatment efficacy and sustainability.
This article examines an initiative that integrated sustainable prescribing with best-practice respiratory management in a UK general practice. Implemented independently before aligning with NHS sustainability policies, the approach focussed on staff education, restructuring respiratory consultations, and enhancing patient awareness. By embedding environmental considerations into routine care, the initiative demonstrates how local-level interventions can contribute to national carbon reduction goals while maintaining high-quality respiratory care.
This initiative was driven by 2 primary concerns: excessive reliance on short-acting beta-2 agonist (SABA) inhalers, which increases both exacerbation risks and carbon emissions, and the underuse of preventer inhalers, which are essential for controlling symptoms effectively.2,6 Our approach aimed to optimise prescribing practices through education, patient-centred care, and the adoption of sustainable inhaler alternatives, aligning with NHS sustainability goals.
Objective
This article aims to review a structured quality improvement initiative implemented just prior to the COVID-19 pandemic, designed to enhance both clinical efficacy and sustainability in respiratory consultations. The objectives are to assess how this approach improved respiratory care for high-risk patients in preparation for potential COVID-19 complications, evaluate its continued relevance in post-pandemic healthcare, and analyse its alignment with evolving national green prescribing policies. Despite being initiated independently of government directives, this initiative provides valuable insights into integrating sustainable prescribing practices within routine primary care.
Specific objectives of this initiative include:
• Achieving at least 95% in-date respiratory reviews to promote appropriate and sustainable prescribing practices. Previously, the practice had only met the NHS Quality Outcomes Framewok (QOF) target of 75%.
• Encouraging the transition of patients from MDI to DPI inhalers where clinically appropriate and where patients were willing.
• Reduce the carbon footprint of the practice’s patient population with COPD and asthma while maintaining or improving clinical outcomes.
Methods
This quality improvement initiative was designed in line with the Plan-Do-Study-Act (PDSA) cycle to enhance respiratory care and promote sustainable prescribing practices. Initiated in January 2020, the intervention focussed on 3 core areas: staff education, restructuring respiratory consultations, and patient education. The overarching aim was to create a framework that supported both clinical excellence and environmental sustainability (Figure 1).

Framework for clinical excellence and environmental sustainability.
Plan Phase: Identifying the Need for Improvement
Considering the key objectives listed above, a preliminary review of electronic patient records (EPR) and prescribing data identified gaps in respiratory care, particularly in achieving in-date respiratory reviews and reducing over-reliance on short-acting beta-2 agonists (SABAs). Additionally, the carbon footprint of metered-dose inhalers (MDIs) was recognised as an area for intervention.
Do Phase: Implementing the Intervention
Staff Education
The training was delivered through in-house clinical meetings and external educational events. Topics covered included Global Initiative for Chronic Obstructive Lung Disease (GOLD), Global Initiative for Asthma (GINA), and National Institute for Health and Care Excellence (NICE) guidelines, ensuring adherence to best practices. The carbon footprint of MDIs versus DPIs and the active ingredients available within the local prescribing formulary were also integrated into training.
To support sustainable prescribing, decision-support tools were embedded within the electronic prescribing system, providing real-time alerts on inhaler carbon impact. Prescribers were educated on strategies to overcome patient barriers to switching from MDIs to DPIs, including concerns about administration techniques and familiarity.
Restructured Respiratory Consultations
The traditional annual recall system was replaced with a risk-stratified approach. High-risk patients, identified through EPR and prescribing data, included those:
• Receiving 4 or more SABA inhalers per year (indicating poor asthma/COPD control).
• Without a prescribed preventer inhaler.
• With a history of exacerbations or hospital admissions.
High-risk patients were prioritised for consultation, and structured reviews were conducted to address medication adherence, inhaler technique, and environmental considerations. The treatable traits paradigm was adopted, ensuring a personalised approach targeting airway, behavioural, comorbid, and risk factor traits (Figure 2).
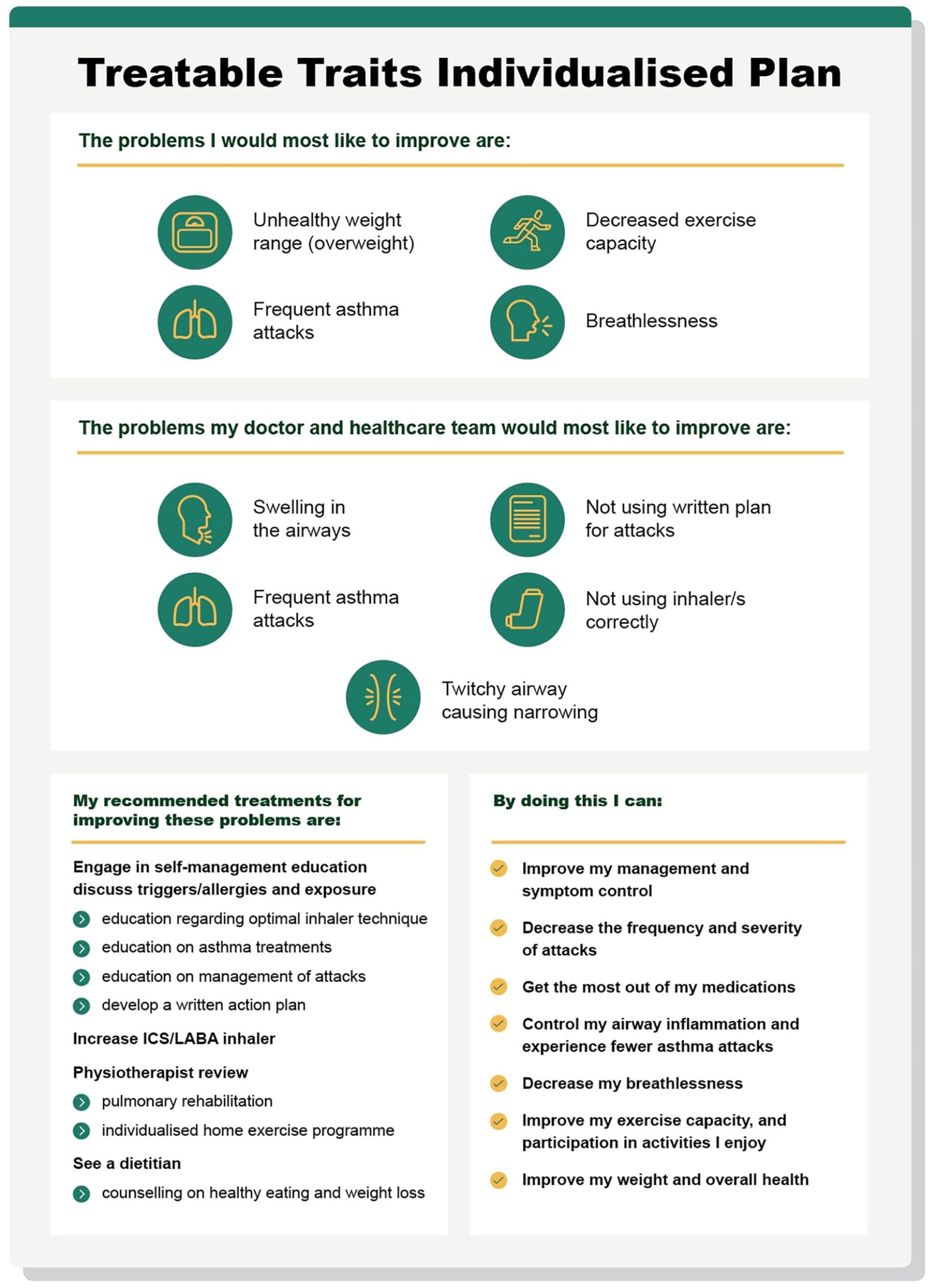
Example of a Treatable Traits Individualised Plan.
Patient Education
Patients were provided with education on MDI versus DPI techniques, both in person and remotely, tailored to individual needs. Training devices were used for demonstration, including:
• DPI trainers that emit a whistle when adequate inspiratory effort is achieved.
• In-check DIAL G16® devices that signal excessive force, improving inhaler technique.
Post-consultation, digital education materials were sent via AccuRx, reinforcing key messages. These included:
• Asthma UK: Inhaler technique guides.
• British Lung Foundation: At-home pulmonary rehabilitation programs.
• Local support programs: Smoking cessation and weight management.
Each patient received a personalised asthma or COPD care plan delivered digitally. The plans outlined prescribed medications, proper usage instructions, and action steps for worsening symptoms using a traffic light system. Reminders emphasised the importance of spacers for MDIs, oral hygiene, and inhaler recycling.
Study Phase: Evaluating the Impact
Key performance indicators (KPIs) were tracked to assess effectiveness:
• In-date respiratory review rates: Monitored via EPR to ensure compliance with the 95% target.
• Prescribing patterns: The proportion of MDIs to DPIs was analysed using OpenPrescribing data.
Patients receiving new inhalers were followed up within 4 to 6 weeks to assess adherence, effectiveness, and satisfaction. For those continuing on stable treatment regimens, ongoing 3-, 6-, or 12-monthly reviews were scheduled as per best practice.
Act Phase: Refinements and Sustainability
Findings from the initial implementation cycle guided refinements in patient education and follow-up strategies. Based on emerging data, consultations emphasised shared decision-making to ensure that patients felt comfortable with inhaler transitions.
As this was the first initiative of this nature in the practice, no predefined quantitative reduction target for MDI prescribing was set, as the transition depended on patient choice. However, by integrating sustainability into routine consultations, it was anticipated there would be a measurable increase in DPI prescribing while maintaining clinical efficacy.
Results
The impact of this initiative was assessed through prescribing trends and in-date respiratory review rates. Data was compared from January 2020 (pre-intervention) to January 2024 (post-intervention), with additional comparisons to national QOF data (2022-2023) where applicable.
In-Date Respiratory Reviews
At baseline (January 2020), the practice had an in-date respiratory review rate of 75%, meeting the Quality and Outcomes Framework (QOF) minimum target but leaving room for improvement. Following the intervention, this rate increased to 95% by January 2024, exceeding the practice’s pre-intervention performance. In the 2022 to 2023 QOF reporting year, 98.03% of asthma patients had up-to-date reviews, notably exceeding the national average of 77.36%. Similarly, 96.48% of COPD patients had in-date reviews, compared to the national average of 87.98%, potentially influenced by the increased funding available during this period. 13

Reduction in MDI Prescribing and Transition to DPIs
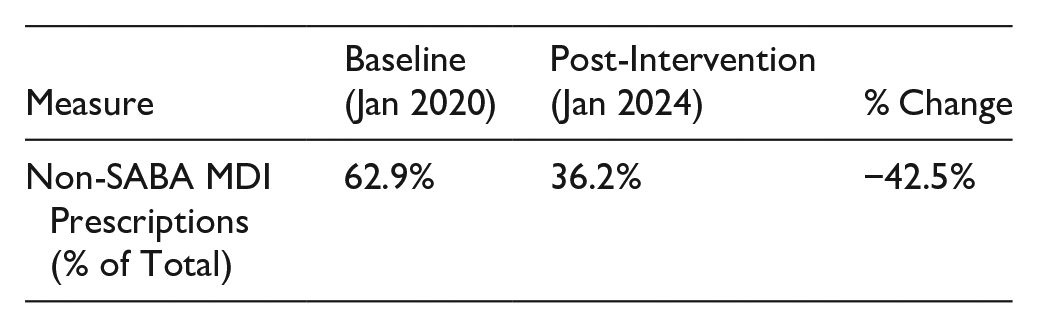
In January 2020, 62.9% of non-SABA inhalers prescribed were MDIs. By January 2024, this figure dropped to 36.2%, representing a relative reduction of 42.5% in MDI prescribing, whilst DPI prescribing increased to 63.8% of all non-SABA inhaler prescriptions.
This prescribing shift aligns with NHS green prescribing goals, which set a 50% reduction target in MDI use by 2028. However, as this was the first initiative of its kind, no predefined quantitative success threshold was set, and results were interpreted as directional improvements rather than statistical absolutes.
Environmental Impact
In January 2020, the practice prescribed 258 SABA inhalers, with an associated carbon impact of 6,015 kgCO2e. Due to a growing patient population, the number of SABA inhalers prescribed increased to 371 by January 2024. However, the associated carbon impact decreased to 5,938 kgCO2e, reflecting a shift towards lower-carbon inhaler alternatives.
For non-SABA inhalers, substantial reductions in MDI prescriptions were achieved. In January 2020, MDIs made up 62.9% of non-SABA inhalers prescribed (322 out of 512 inhalers), placing the practice in the 82nd percentile nationally. By January 2024, the proportion of MDIs dropped to 36.2% (279 out of 770 inhalers), representing a 57.6% reduction. This shift placed the practice in the 4th percentile nationally (see Figure 3), reflecting its leadership in sustainable prescribing practices (Figure 4).

Reduction in carbon impact of prescribed inhalers 2020-2024.
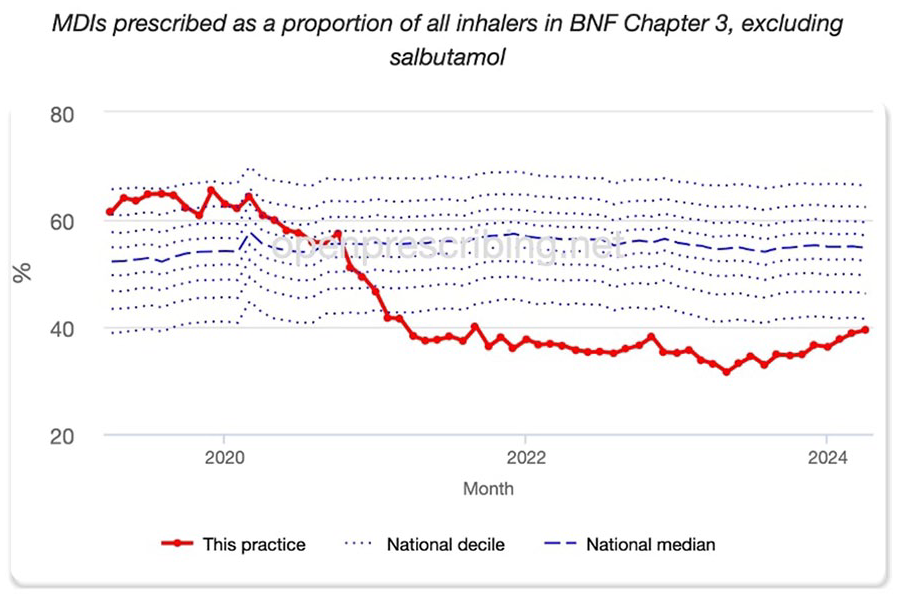
MDIs prescribed as a proportion of all inhalers in BNF Chapter 3, excluding salbutamol (OpenPrescribing.net).
Statistical Considerations and Limitations
As this was a quality improvement project, no a priori statistical significance threshold was set, and no formal hypothesis testing was conducted. Future iterations of this initiative could incorporate statistical analyses, such as chi-square tests for categorical prescribing data and paired t-tests for pre/post comparisons. Additionally, while prescribing data trends were robust, patient adherence and satisfaction measures were not formally analysed, representing an area for further research.
Discussion
The approach implemented by the authoring practice demonstrates how local initiatives can drive meaningful improvements in respiratory care and environmental sustainability. By adopting the treatable traits paradigm, care was personalised and holistic, focussing on individualised interventions that improve patient outcomes whilst reducing reliance on high-carbon inhalers. The incorporation of best practice principles - ensuring the right treatment (at the right time), for the right patient, in the right formulation, for the right duration - provided a structured framework that optimised treatment efficacy and sustainability.
National Impact and Theoretical Context
The prescribing changes observed in this initiative align with broader NHS sustainability goals, particularly the commitment to reducing MDI prescriptions by 50% by 2028 and achieving net-zero carbon emissions by 2040. The reduction of non-salbutamol MDIs by 57.6% over 4 years demonstrates the feasibility of transitioning to low-carbon prescribing while maintaining clinical standards. However, further research is needed to assess the feasibility of replicating these results across different healthcare settings.
If similar initiatives were widely adopted, modelling suggests that a reduction in MDI prescribing at scale could contribute to an estimated 2.6% reduction in NHS carbon emissions annually. 14 While this projection is based on practice-level data, broader implementation would require additional evaluation at a national level to validate the impact of such transitions. Comparisons to international benchmarks, such as Sweden, where only 13% of inhalers are MDIs, indicate that significant reductions in MDI use are achievable with the right strategies and system-wide alignment.15,16
Despite an increase in the practice population, carbon emissions from inhaler prescriptions decreased from 6015 to 5938 kgCO2e, reflecting the role of prescribing interventions in mitigating environmental impact. These reductions suggest that sustainable prescribing can be implemented effectively alongside routine clinical care, though further long-term monitoring is needed to assess the durability of these changes.
Education as a Catalyst for Change
Education was one of several components aimed at improving prescribing behaviours and patient adherence. Training provided to staff on the environmental impact of inhalers was integrated into broader clinical decision-making strategies, encouraging discussions around sustainable alternatives. The role of education in behaviour change is supported by established frameworks, such as the Theory of Planned Behaviour (TPB), which suggests that awareness influences prescribing decisions. However, no formal qualitative or quantitative assessment was conducted to measure the direct impact of education on prescribing patterns, and its specific contribution remains unquantified.
While patient education was included within consultations to enhance understanding of inhaler technique and sustainability considerations, its impact on adherence and prescribing choices was not formally assessed. Surveys by Asthma + Lung UK indicate that awareness of inhaler environmental impact is generally low, with 60% of patients willing to switch to DPIs when informed. 2 While this aligns with the goals of the initiative, no formal data collection was undertaken within the practice to measure patient attitudes before and after educational interventions. Future studies should incorporate structured patient feedback to evaluate the extent to which education influences decision-making and adherence.
Additionally, inhaler technique training and the promotion of inhaler recycling programs were introduced to support best practices in inhaler use. Proper disposal of MDIs is a critical component of reducing environmental impact, as it minimises plastic waste and prevents the release of residual hydrofluorocarbons (HFCs). Although the adoption of recycling programs was encouraged, no formal data was collected on patient participation rates, highlighting an area for further evaluation.
Challenges and Opportunities
While this initiative demonstrated measurable improvements in prescribing practices, challenges remain in ensuring continuity of care across healthcare settings. New patients transferring into the practice often arrived with MDI prescriptions, necessitating additional review and counselling to align with sustainable prescribing goals. This underscores the need for system-wide alignment to support consistent implementation of green prescribing strategies beyond individual practices.
Financial incentives, such as those provided by the Investment and Impact Fund (2022-2023), may have played a role in supporting other practices in the initial adoption of sustainable prescribing, but it was not continued in subsequent years. 2 Without continued policy-driven incentives, maintaining momentum in green prescribing may be challenging, particularly for practices balancing multiple clinical priorities. Future policy efforts should consider embedding sustainability targets within standard prescribing frameworks to ensure long-term adoption.
The cost of DPIs, historically a barrier to widespread use, has become less prohibitive with recent pricing changes. This suggests that financial constraints are no longer the primary limiting factor, and that behavioural and structural barriers - such as patient familiarity with MDIs and clinician prescribing habits - are the key challenges to address.2,17 Ensuring that shared decision-making remains central to prescribing discussions will be critical in overcoming these challenges and achieving sustained improvements in respiratory care.
Conclusion
The UK’s high reliance on MDIs presents a significant opportunity to reduce the environmental impact of respiratory care through green prescribing. While this initiative demonstrated changes in prescribing trends towards increased DPI use and in-date reviews, the role of education in achieving these outcomes remains unclear due to the absence of formal before-and-after assessments.
The decision to incorporate provider and patient education was based on the need to align prescribing behaviour with NHS sustainability goals, as well as existing evidence that awareness influences prescribing habits. However, no specific educational programs were evaluated for their impact, and no structured assessment of changes in awareness was undertaken. Future initiatives should include baseline and post-intervention evaluations to assess the direct impact of education on prescribing behaviour and patient adherence.
This initiative provides a model for embedding sustainability into routine clinical care. However, addressing challenges such as continuity of care, system-wide policy alignment, and patient engagement will be essential for scaling green prescribing efforts across the NHS. Future research should focus on quantifying the role of educational interventions, analysing the impact of prescribing changes on clinical outcomes, and ensuring that sustainability targets do not compromise patient care. Lessons from international best practices indicate that system-wide changes are achievable but require robust data-driven evaluation and strategic policy support to sustain long-term impact.