
Abstract
Objectives:
This study evaluates social, behavioral, and environmental determinants to differentiate between active and inactive asthma and how predisposing, enabling, and need factors elucidate asthma-related health services and asthma control among women in Puerto Rico.
Methods:
This study analyzed secondary cross-sectional data from a subsample of 625 adult females who participated in the Asthma Call Back Survey in Puerto Rico. Logistic and multinomial regression analyses were conducted to examine associations between explanatory variables and asthma outcomes.
Results:
In total, 63% of women reported active asthma, from which 37.9% have not well controlled or very poorly controlled asthma. Women with active asthma were significantly more likely to be out of work, have middle income (US$25,000–<US$35,000), and be obese (≥30 kg/m2). Perceived need of health status is a good predictor to know the odds ratio of women to use emergency room. Women with poorly controlled asthma were significantly associated with increased units of physician urgent visits and emergency room visits.
Conclusion:
The findings confirmed significant determinants for active asthma and adds information on odds ratio for sensitive subgroups that utilize asthma-related health services in higher proportion than their counterparts. These associations suggest a development of asthma management plan targeting women to control the condition and reduce health-care utilization.
Keywords
Introduction
Both lifetime and current asthma prevalence in Puerto Rico reflect no significant changes during the last 10 years. Adult lifetime asthma in the unincorporated territory of Puerto Rico is higher (17.2%) than in the continental United States and Hawaii combined (14.1%). 1 Researchers have determined that Puerto Ricans of both genders have a genetic susceptibility to asthma2–5 and are less responsive to bronchodilators than other Hispanic or ethnic groups.4,6
Among Puerto Ricans, active asthma is consistently higher for adult females than for adult males. 7 Adult females are observed to have higher hospital admissions, higher emergency room visits (ERVs), and higher drug claims for asthma-related symptoms. 8 Among females, the 40–54 years age group is the most impacted by asthma hospitalizations.9,10 Researchers have demonstrated that female hormone levels are associated with reduced lung function, increased asthma susceptibility, and increased incidence of asthma-related symptoms.11–13 Although genetic factors and hormonal risk factors explain some measure of the general propensity for asthma among Puerto Rican women, minimal research exists that targets the distribution of modifiable risk factors or examines the contribution of modifiable risk factors to uncontrolled asthma among adult females in Puerto Rico.14,15
This is the first study addressing the determinants for asthma-related health services and asthma control among adult female population of Puerto Rico. Research specifically targeting females stated that health studies should explore risk factors by gender and recommended disaggregating data by sex.16–18 In addition, this is the first study that employed Andersen’s behavioral model (BM) to elucidate asthma-related health services and asthma control among this target subpopulation.
BM was initially developed in the 1960s to explain the use of health services,19,20 but it was redirected to evaluate health service utilization decisions at the individual level and is now solely credited with what has proven to be a more robust application of the earlier concepts. 20 According to the BM (Figure 1), the determinants of health service utilization can be classified as predisposing, enabling, or need factors.19–22 Predisposing characteristics are those variables that prime individuals to use health-care services and include demographic characteristics, social structure, and health beliefs. 21 Enabling resources facilitate or impede health-care use and include personal, family, and community resources. Need has two dimensions. Perceived need is the individual’s own assessment of the need for medical services, while clinically evaluated need is the health-care provider’s professional recommendation for service use. 21 Andersen’s BM has been widely used in primary and secondary data analyses, 23 mainly to assess chronic conditions among adults and its associations with health-care utilization.24–26 Additionally, BM has been employed to assess asthma-related health services among children.27,28
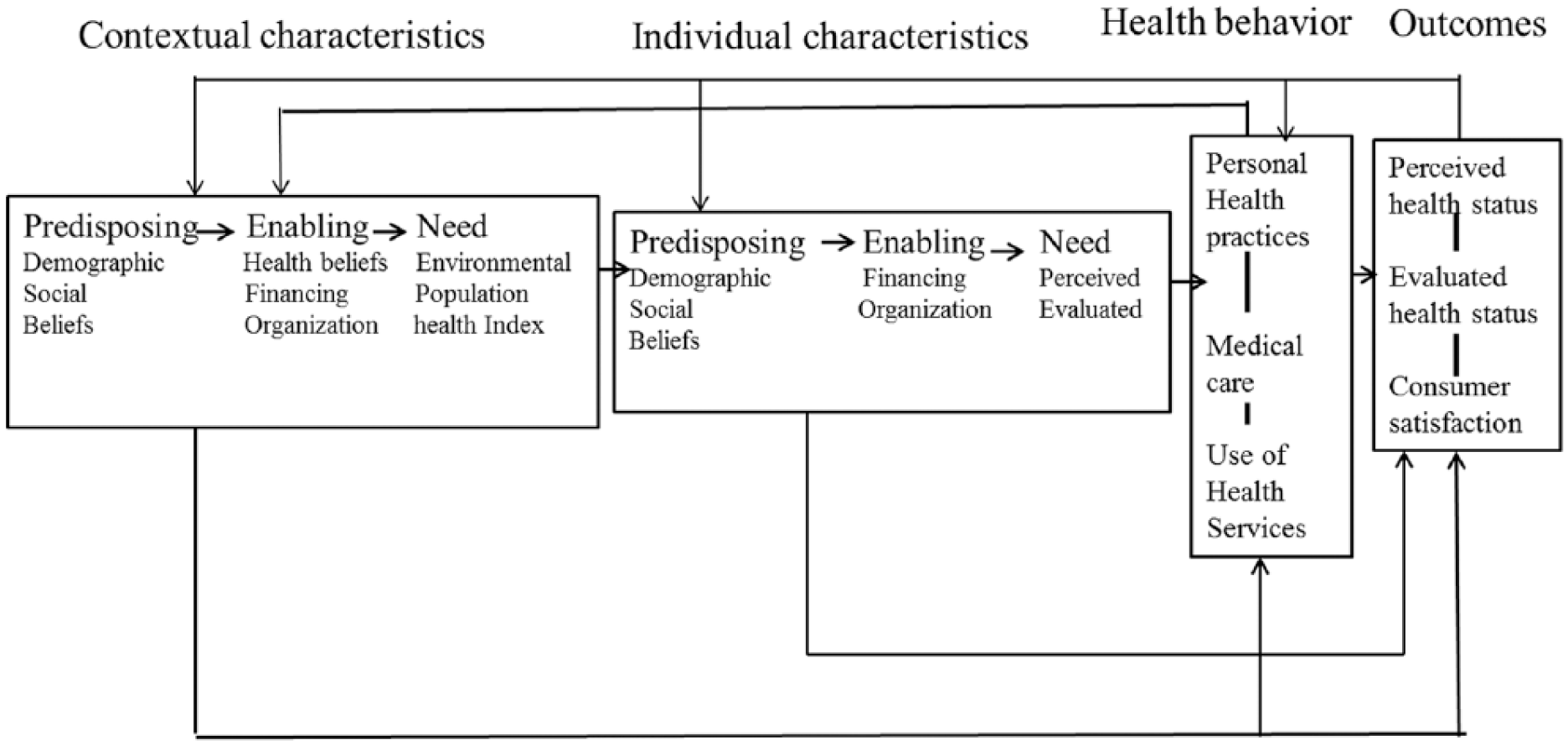
The behavioral model of health services use 2000s version.
The goal is to establish (a) whether there were differences between active and nonactive asthma status among adult females living in Puerto Rico and (b) how the Andersen model predictor factors explain asthma-related services and achieved level of asthma control among adult females living in Puerto Rico.
Methods
The study systematically analyzed cross-sectional data from the Asthma Call Back Survey (ACBS) conducted during 2011 and 2012 in Puerto Rico. ACBS is conducted every year by the Puerto Rico Behavioral Risk Factor Surveillance System (PR-BRFSS) of the Department of Health of Puerto Rico with the assistance of the Centers of Control and Prevention (CDC). Survey follows CDC protocols to meet data quality standards applied to the 50 states and US territories (i.e. Puerto Rico, Guam, and the Virgin Islands). The BRFSS survey has three sections: core questions, optional questions, and regional questions. 29 Participants in the ACBS are those who reported being diagnosed with asthma at any point in time in the PR-BRFSS main interview. These participants are recruited by the PR-BRFSS for callback 2 weeks after the main interview completion date. 30 The eligible participants are individuals 18 years or older living in a typical household and college housing but not in vacation homes, group homes, or institutions. 30 The sample is randomly generated from a sampling frame of landline and cellular telephones with each having equal probability of selection. Each year, the total sample size includes at least 4000 interviews in Puerto Rico; 20% of the interviews are from cellular and 80% from landline phones. 30 Participants who affirmatively respond two questions in the BRFSS main survey: “Have you ever been told by a doctor or other health professional that you have asthma?” and the subsequent question, “Do you still have asthma?” are classified as current or actively asthmatic. For those who answered that question negatively are classified as asthmatic but not currently active. 31 The richness of data from the BRFSS-ACBS permits the inclusion of variables consistent with the latest version of Andersen framework (Figures 2–3). For this investigation, 12 independent variables were applied derived from the BRFSS that are interconnected to ACBS dataset: four sociodemographic and/or predisposing variables (age group, marital status, education, and employment), five behavioral variables (smoking, smoking level, physical activity, meet aerobic recommendations, and body mass index (BMI)), two enabling variables (income, health insurance), and one need-related variable (health status). From 1444 variables of ACBS, we utilized 14 variables: 3 dependent variables of (a) current asthma status, (b) asthma-related health-care utilization (composed by asthma urgent visits, asthma ERV, and asthma hospitalizations), and (c) asthma control (composed of number of asthma symptoms in past 30 days, frequency nighttime awakenings in past 30 days, and frequency of rescue medicine). The independent variables included seven environmental variables (secondhand smoke, mold inside, pets inside, cockroach inside, rodents inside, dehumidifier use, and air cleaner inside).

Andersen behavioral model for health care utilization on asthma.
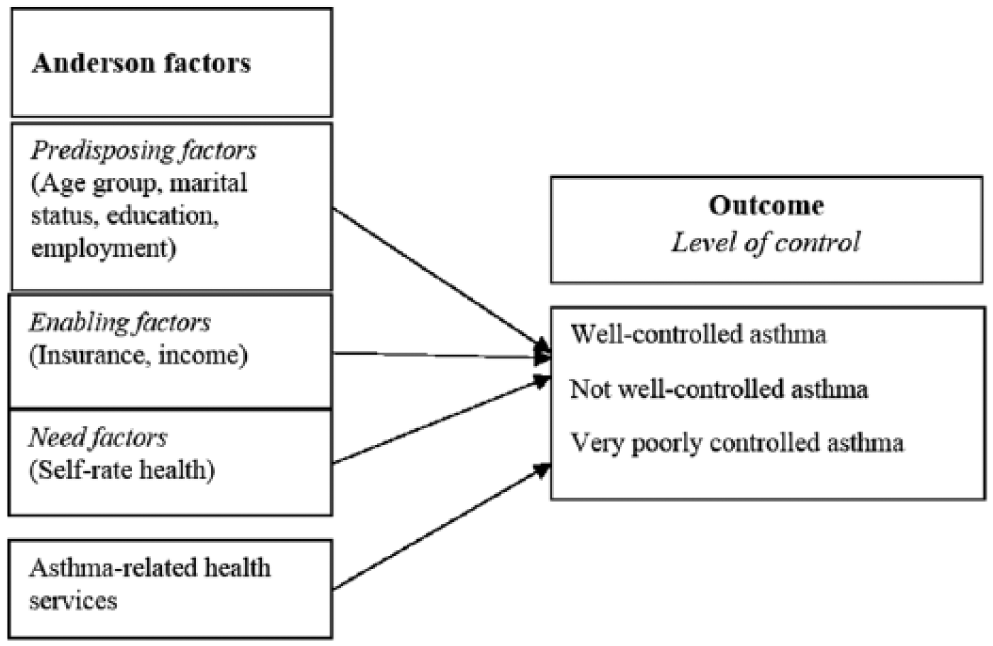
Andersen factors and health care utilization explaining asthma control level.
The analysis combined 2 years to increase power sample using data that have the same sampling and weighing methodology. The Puerto Rico ACBS had 366 respondents during 2011 and 434 participants during 2012 for a total of 800 participants. Data for 2 years were combined to develop a subsample appropriately formatted for the study operationalization requirements. Subsample databases were standardized in terms of variable order and answer codes for each year. The combination of data from 2 years required the adjustment of the weight variable in the dataset of each year. For that purpose, the sum of calculated weights of each year was divided by 2 to obtain the final weight for this subsample.
A statistically improved dataset resulted for the subsample of women diagnosed with asthma to conduct several logistic and multinomial regression analyses at 0.05 as a level of confidence. A logistic model was utilized for the dependent variable of current asthma status (active/inactive asthma). The independent variables were social (age group, marital status, education, income, employment, and health insurance coverage), behavioral (smoking (yes/no), physical activity (yes/no), and BMI (normal weight: 20–25 kg/m2, overweight: 25–30 kg/m2, and obese: ≥30 kg/m2)), and environmental variables (secondhand smoke (yes/no), mold inside (yes/no), pets inside (yes/no), cockroach inside (yes/no), rodents inside (yes/no), dehumidifier use (yes/no), and air cleaner inside (yes/no)).
For the dependent variable asthma-related health-care utilization, three regression models were utilized to determine the association between the dependent variables and Andersen predictors. A Multiple linear regression (MLR) was run for the dependent variable asthma urgent visit (continuous). For dependent variables ERVs (yes/no) and hospitalizations (yes/no), a logistic regression (LR) was ran utilizing the same predictors according to Andersen model. The independent predisposing variables are age group (18–34, 35–44, 45–54, and 55 years or older), marital status (married, divorced, widowed, separated, and never married), education (did not graduate high school, high school graduate, college or technical college, and graduate from college), and employment (employed for wages, self-employed, out of work, homeworker, student, and unable to work); enabling variables are income (less than US$15,000, 15,000 to less than US$25,000, 25,000 to less than US$35,000, 35,000 to less than US$50,000, 50,000 or more) and health insurance (yes/no); and need variables are self-rate health status (excellent, very good, good, fair, and poor).
Finally, three models utilizing MLR were run for the dependent variable asthma control (well controlled, not well controlled, and very poorly controlled) to determine the extent to which it was associated with the independent variables of predisposing factors, enabling factors, need factors, and asthma-related health-care utilization. Achieved level of asthma control was assessed by number of symptoms in the past 30 days, times of nighttime awakenings in the past 30 days, and times using a asthma rescue medication. 32 The continuous variable number of asthma symptoms in the past 30 days was statically manipulated to an ordinal variable, where 1–8 days was classified as well controlled, from 9 to 29 days was classified as not well controlled, and symptoms every day in the past 30 days and during the day was classified as very poorly controlled. Times of nighttime awakenings in the past 30 days were transformed to the ordinal variable, where less or equal 2 days/nights was classified as well controlled, from 3 to 12 days/nights was classified as not well uncontrolled, and more or equal than 13 days/nights in the past 30 days was classified as very poorly control. Finally, for frequency of rescue medication, responses for questions “How many times a week you used short-acting beta2 agonists (SABA)” were grouped. There are 11 questions about different SABA medications (including ilp08_3: Albuterol, ilp08_4: Alupent, ilp08_9: Bitolterol, ilp08_10: Brethaire, ilp08_20: Maxair, ilp08_21: Metapropteronol, ilp08_23: Pirbuterol, ilp08_24: Proventil, ilp08_28: Terbutaline, ilp08_30: Tornalate, ilp08_33: Ventolin). The times that a participant used SABA medications were totalized and divided by 7 (to estimate daily use in week). The collapsed variable had three categories following the National Asthma Educational and Prevention Program (NAEPP) guidelines (<0.29/day (well controlled), >0.29 times/day but <2 times/day (not well controlled), and >2 times per day (very poorly control) as shown in Table 1). 33 Missing data ranged from 18 cases to 92 cases in variables BMI and income, respectively, which is sensitive information tied to social desirability bias. 34
Dependent variables.

AA=No active asthma MD= No doctor of medicine visit past year
Results
Among 625 women who were diagnosed with asthma in any time of her life, 63% (395) had active asthma. In total, 65% of them were 55 years or older. Nearly 40% of adult females were married; 34% did not graduate from high school, and 41% were out of work for more than 1 year. In total, 61% of the participants had an income of less than US$15,000. Almost all women had health insurance (97%). In total, 37% of the females were categorized as obese (≥30 kg/m2) according to the calculated BMI. In total, 56% of women did not engage on 30 min or more of moderate-intensity physical activity on all or most days of the week. Table 2 shows Pearson test indicating that there was a statistically significant association between behavioral independent variables and asthma status. There was a statistically significant association between physical activity and asthma status, where Pearson χ2(2), n = 625 = 6.326, p ≤ 0.05. The strength of this association was weak according to Cramer’s V = 0.101. Additionally, there was a statistically significant association between BMI and asthma status, where Pearson χ2(1), n = 607 = 17.853, p ≤ 0.001. The strength of this association was also weak according to Cramer’s V = 0.171.
Chi-square results for significant behavioral characteristics and current asthma status among women in Puerto Rico.

p ≤ 0.050.
The frequency distribution of environmental risks shows that only 8% were exposed to secondhand smoke in their homes. Environmental controllers for humidity (10%) and dust in homes (15%) were used infrequently among participants. Among the four age groups, adult females 55 years or older reported a higher percentage (88%) of less education; a higher percentage were out of work for more than 1 year (71%), were retired (97%), or were unable to work (80%). This age group also had less annual income (75%) compared to other age groups. Additionally, 76% of adult females 55 years or older reported to have fair or poor self-rated health. This age group also reported a lower percentage of physical activity and a higher percentage of being obese. About one-third of women (30.4%) had visited a physician urgently because of asthma during the previous year to the assessment (3.66 average; standard deviation (SD) = 4.83), while only one-fifth (20%) had visited an emergency room (ER), and 12% women had hospitalization in the previous year of the assessment. The average number of asthma symptoms in the last 30 days of the assessment was 7.38 (SD = 10.99). For nighttime awakenings in the last 30 days, the mean was 3.90 times (SD = 8.62). Women who reported to have not well controlled or very poorly controlled asthma were 37.9%, where 30% of them were under 55 years of age or more.
The LR model for active asthma was statistically significant (χ2(33) = 50.813, p = 0.025), and it explained 13% of the variance (Table 3). The significant predictors for active asthma were being out of work for more than a year (odds ratio (OR) = 2.342), income of US$25,000–<US$35,000 (OR = 3.135), and the BMI indicator of obese (OR = 2.349). The rest of sociodemographic and environmental variables were not significant.
Summary of logistic regression for significant socioeconomic and behavioral characteristics among women with asthma during 2011 and 2012 in Puerto Rico.

BMI: body mass index; SE: standard error; OR: odds ratio; CI: confidence interval.
p ≤ 0.050. **p ≤ 0.010. Otherwise p > 0.050.
For asthma-related health services, the MLR for physician urgent visits in the last 12 months was not significant. However, the LR model for ERVs in the last 12 months of the assessment was statistically significant (χ2(26) = 44.925, p = 0.012), explaining around 17% of the variance. The model showed (Table 4) that being self-employed (B = 1.581, p = 0.030, OR = 4.860) was a significant predictor for ERV indicating that self-employed respondents were 4.86 times more likely to have a visit to the ER than respondents who were employed. Self-rated health status was a significant predictor, B = −2.710, p = 0.003, OR = 0.067, indicating that these respondents were 14.93 times more likely to not have a visit to the ER in the last 12 months than respondents who rated their health status as poor. A self-rated health status of good was also a significant predictor, B = −0.999, p = 0.024, OR = 0.368, indicating that these respondents were 2.72 times more likely to not have a visit to the ER in the last 12 months than respondents who rated their health status as poor. Finally, a self-rated health status of fair was also a significant predictor, B = −0.797, p = 0.016, OR = 0.450, indicating that these respondents were 2.22 times more likely to not have a visit to the ER than respondents who rated their health status as poor. The rest of the predisposing, enabling, and need factors were not significant. The Wald test did not demonstrate statistical significance between the binary-dependent variable asthma hospitalizations in the last 12 months (yes or no) and any of the Andersen model predictors.
Results of the logistic regression of predisposing, enabling, and need factors predicting a visit to the ER for asthma-related services in the last 12 months.

ER: emergency room; SE: standard error; OR: odds ratio; CI: confidence interval.
p ≤ 0.050. **p ≤ 0.010. Otherwise p > 0.050.
The MLRs for very poorly controlled asthma symptoms in the last 30 days (B = 0.261, p = 0.001, OR = 1.299) and for very poorly controlled nighttime awakenings in the last 30 days (B = 0.297, p = 0.001, OR = 1.345) were explained mainly by asthma-related health services. One-unit increase in urgent visit would result in a 1.299 increase in the relative risk for very poorly controlled symptoms relative to well-controlled symptoms (Table 5). One-unit increase in urgent visit would result in a 1.345 increase in the relative risk for very poorly controlled nighttime awakenings relative to well controlled (Table 6). ERVs in the past 12 months was also a significant predictor (B = 1.851, p = 0.032, OR = 6.363), which suggests that having ERVs would result in a 6.363 increase in the relative risk for very poorly controlled relative to well-controlled asthma according to nighttime awakenings (Table 6). The rest of the predisposing, enabling, need, and asthma-related health services factors were not significant.
Results of the multinomial logistic regression of predisposing, enabling, need, and asthma-related health-care utilization factors in the last 12 months predicting asthma control by frequency of asthma symptoms in the last 30 days.
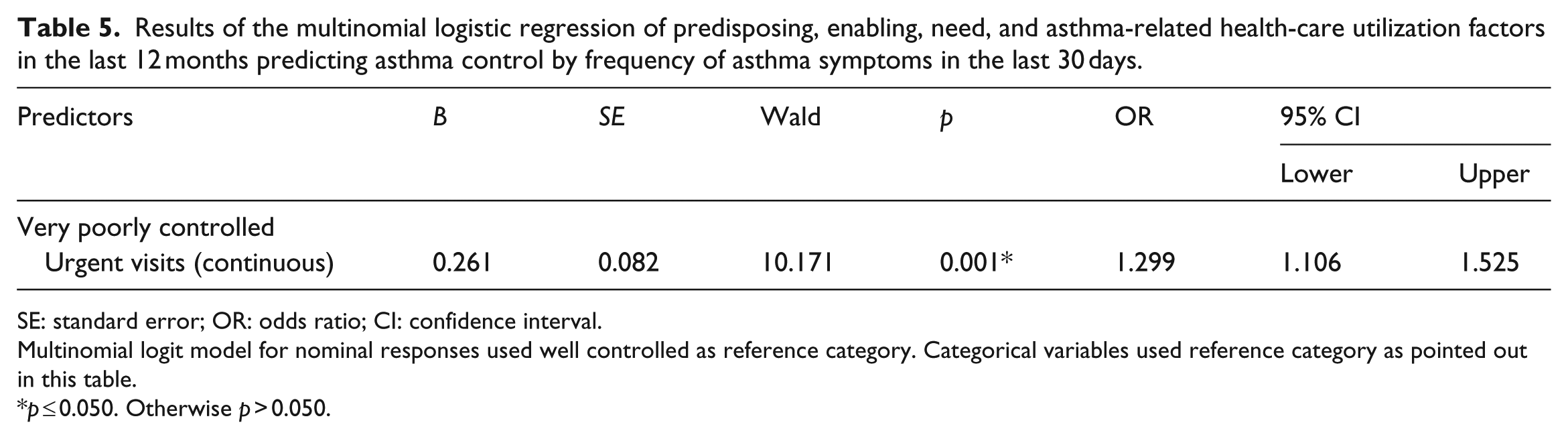
SE: standard error; OR: odds ratio; CI: confidence interval.
Multinomial logit model for nominal responses used well controlled as reference category. Categorical variables used reference category as pointed out in this table.
p ≤ 0.050. Otherwise p > 0.050.
Results of the multinomial logistic regression of predisposing, enabling, need, and asthma-related health-care utilization in the last 12 months predicting asthma control by nighttime awakenings in the last 30 days.

ER: emergency room; SE: standard error; OR: odds ratio; CI: confidence interval.
Multinomial logit model for nominal responses used well controlled as reference category. Categorical variables used reference category as pointed out in this table.
p ≤ 0.050. **p ≤ 0.010. Otherwise p > 0.050.
Discussion
The importance of this study is based on female disparity in asthma morbidity in Puerto Rico and the differences in asthma management and impact of utilization of asthma-related health services. Among adult females aged 18 years or older, who have been diagnosed with asthma in Puerto Rico, there is a high prevalence (63%) of active asthma that remained constant during both years assessed. The population of women diagnosed with asthma is mostly (61%) poor (<US$15,000 annually) as compared to the 40.2% of population with the same household income in Puerto Rico. 35
Almost the entire population assessed (97.1%) had health insurance coverage, which is considered a strong predictor of health-care access, 23 physician recommendations of an asthma management plan. 27 In Puerto Rico, nearly 40% of the population is eligible for public health insurance covered through programs offered by the local government. 36 In addition, 37% of the population is covered by private health insurance offered through employers, and 18% is covered by federal programs, such as Medicare and Veterans benefits. 36 Overall, Puerto Rico has 6.4% fewer people without health insurance coverage as compared to 13.4% in the United States. 37 Even though Puerto Rico has high health insurance coverage, there are higher percentages of health-care cost barriers as compared with other unincorporated US territories, such as Guam and the Virgin Islands. 38 Barriers other than financial have been documented for filling asthma prescriptions, such as asthma devices not covered by the insurance plans, as well as concerns about the side effects and long wait times in the pharmacy.39,40 Inhaled corticosteroids, the most clinically effective medication for asthma control, had the lowest utilization rate among available treatments during 2000–2003. 39 Furthermore, inhaled corticosteroids were less likely to be prescribed for asthma sufferers with public insurance than for individuals with private insurance during the same period. 39
In this study, 41% of women self-reported to be out of work for more than 1 year. Women out of work for more than 1 year were 2.34 times more likely to have active asthma than those who were employed. Unemployment is a significant predictor for poor asthma outcomes and is one of the reasons for a patient’s dissatisfaction with life. 41 Findings from our study also indicated that women with a low-middle income (US$25,000–US$35,000) were 3.14 times more likely to have active asthma than women who earned less than US$15,000. Lower income is a predictor of asthma severity in the United States.42,43 However, in Puerto Rico, the group of women classified in the low-middle income experience greater economic pressure because they have no social welfare like those who are under lower income bracket. Additionally, the US Census classified 25% of women in Puerto Rico as the head of the family with no husband present 44 and who in the majority of cases do not receive alimony from the former husband. Women are at higher risk of being more vulnerable to bad health outcomes due to disparities strengthened by social factors, 45 such as being the only family head.
Results confirmed that physical activity and BMI were important predictors for active asthma. Among women with active asthma, 60% did not engage in physical activity. Additionally, almost three-quarters of women with active asthma were classified as overweight (25–30 kg/m2) and obese (>30 kg/m2), and one-third were under the age of 55 years. Obesity is a known risk factor for activity restriction among women. 46 This study confirmed that obese women were 2.35 times more likely to have active asthma. Obesity has been associated with increased degree of asthma prevalence;14,47 asthma severity among women; 48 and worse physical health status, activity restriction, and worse quality of life. 46 Conversely, regular physical activity is associated with reduced risk of exacerbation of asthma among women. 49
Additionally, this study was the first to assess the relationship between Andersen factors and asthma health-care utilization among adult females in Puerto Rico. Although neither of Andersen factors were significant for physician urgent visits due to asthma, predisposing and need factors were significant for ERVs. Women who were self-employed were 4.86 times more likely to visit an ER than women who worked for an employer. Social characteristics such as employment make people more or less prone to use health services. 22 Most uninsured workers are self-employed, and the ER is the first option for health care because it is a required service by federal provision to all patients without insurance. 50
This study confirmed that women with active asthma who self-reported a better health status were less likely to use the ER. Women who self-reported very good health status were 14.9 times less likely to visit an ER; those with good health status were 2.72 times less likely, and those with fair health status were 2.22 times less likely to visit an ER. ERVs are more likely associated with acute illness. 51 Perceived need factors in chronic conditions have a significant impact on health-care utilization.20,25,51,52 For hospitalizations due to asthma, the significant factors showed wide confidence intervals (CIs) and were not taken into consideration.
This study demonstrated significant predictors for very poorly controlled asthma symptoms and very poorly controlled nighttime awakenings in the previous 30 days but not for asthma medication use. Asthma symptoms were predicted by physician urgent visits in the previous 12 months. The mean for number of urgent visits to the physician was nearly four times, and the maximum number of visits was 26 times in the previous 12 months of the assessment. OR showed that one unit of increase in physician urgent time visits among women would result in 1.30 increases in relative risk of asthma symptoms poorly controlled.
Very poorly controlled nighttime awakenings in the previous 30 days were predicted by physician urgent visits and ERVs. Results showed that one unit of increase in physician urgent time visits would result in women having 1.35 increases in the relative risk to have more than 13 days/nights with nighttime awakenings in 1 month. Additionally, ERVs would result in 6.36 increases in relative risk to have more than 13 days/nights by month with nighttime awakenings. Poor asthma control was associated also with an increase in ERVs during the last year of the assessment among adults from New England. 53 In 2011, Latin American patients with poorly controlled asthma had greater utilization rates of asthma-related services. 54
There are several limitations in this study related to nature cross-sectional data. The observed relationships do not imply causality, and findings cannot be generalized to populations that did not participate in the ACBS or to other populations surveyed during other time periods. Selection bias could be a potential threat because eligible respondents for ACBS had the right and the opportunity to refuse to participate. There is a possibility that those who refused may have been systematically different from those who chose to participate. However, Puerto Rico has one of the lowest refusal rates (18.6%) as compared to the median of the United States for the same survey. Because asthma outcomes have seasonal variation, self-reported asthma may be underestimated during 2011 and 2012, when PR-BRFSS did not collected data all year long. Additionally, responses for physical activity, smoking, and weight to calculate BMI are subject to validity of self-response, because of sensitive to social desirability. 33 Finally, although the total subsample size was adequate according to the power sample analysis, the broad CIs in some of the predictors of the multinomial models reflected small samples by each cell. Small samples will result in very wide CIs around the estimated OR, independently if the predictor had a significant p-value. 55
It is highly recommended to reduce variables selected to operationalize Andersen factors to reduce the small sample size among predictors. One consequence of the model’s inclusivity is that it demands an overwhelming variety and amount of data to operationalize in its entirety and is overly expansive for any given piece of research. The fact that BMI was significant in LR models supports further analysis including this predictor in the Anderson framework as a need factor for asthma-related health services and asthma achieved level of control. Finally, a further study requires including 3 years of data, which is the maximum time frame allowable for the ACBS, in order to increase the sample for MLR analysis.
Conclusion
This study confirmed that BM can guide secondary data analysis for asthma utilizing LR and MLR models. Predisposing, enabling, and need factors, together with health-care utilization, explained or predicted asthma outcomes. This study contributed to the limited literature on asthma-related health services and asthma control among women in Puerto Rico. The findings confirmed significant determinants for active asthma and adds information on OR for sensitive subgroups that utilize asthma-related health services in higher proportion than their counterparts. In addition, the study adds information on OR for subgroups of women who are more vulnerable to have poorly controlled asthma. Subgroups of women who are out of work, the poor working class, and obese are more susceptible to have active asthma. Women classified under category self-employed utilized more the ER than their counterparts. In addition, need factor of self-rate health status is a good predictor to know the OR of a women to use ER. The better perception of their health, better the chance not to visit an ER. Additionally, increase in physician urgent time visits predicts that women will be more likely to have everyday asthma symptoms and nighttime awakenings in 1 month.
These findings could guide health-care professionals to develop a more individual asthma management plan for adult females. The fact that certain subgroups among women with asthma are at higher risks than others is important information to be considered by health-care professionals dealing with patient’s asthma management and control. Understanding sociodemographic and behavioral characteristics of women with asthma could improve the asthma management plan to reduce poor outcomes and higher costs in asthma-related health-care utilization. Moreover, this information should be used in promotional and educational programs to increase asthma knowledge among women on how to improve asthma self-management, as well as personalized medicine in asthma management plan.
Supplemental Material
SMO745903_Supplementary_Material_REV1 – Supplemental material for Asthma-related health services and asthma control among women in Puerto Rico
Supplemental material, SMO745903_Supplementary_Material_REV1 for Asthma-related health services and asthma control among women in Puerto Rico by María Calixta Ortiz-Rivera in SAGE Open Medicine
Footnotes
Acknowledgements
Thanks to Dr Mary Lescoe-Long, Dr Cheryl B. Cullen, Dr Laurence Fulton, and Dr Gudeta Fufaa from Walden University for the study recommendations; Dr Ruby Serrano for providing cues to work with Behavioral Risk Factor Surveillance System and the Asthma Call Back Survey; and Dr José Bartolomei and Eliseo Acevedo from the Puerto Rico Asthma Project for providing 2011 data not accessible to the public.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The protocol for this investigation was approved under the number IRB 05-14-15-0153777.
Supplementary material
Supplementary material for this article is available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.