
Abstract
Background:
Colorectal cancer (CRC) screening uptake remains suboptimal despite the importance and effectiveness of various testing options. The purpose of our study was to identify barriers and facilitators to CRC screening in a community-based sample in Salt Lake County, Utah to inform future efforts to develop effective interventions to increase CRC screening.
Methods:
This study enrolled adults eligible for CRC screening at 6 community health events. Participants completed targeted questionnaires based on whether they had discussed screening with a provider and whether they had received screening. We identified participant-reported barriers to CRC screening using descriptive analysis. Univariate and multivariate analyses were used to identify participant characteristics associated with receipt of screening.
Results:
Of the 117 participants who completed the questionnaires, 43.6% were 50 to 60 years old, 36.8% identified as white, and 51.3% identified as non-Hispanic. The most common barrier to colonoscopy was the need for extensive bowel preparation (30.8%). For stool tests, common barriers included handling stool (20.5%) and not understanding how to do the test (20.5%). For virtual colonoscopy, barriers included the need for extensive bowel preparation (21.4%) and cost (21.4%). Most participants (67.5%) believed that they should know about all CRC screening options available, and their importance. The majority of participants (68.4%) preferred to learn about CRC screening from their doctor or healthcare provider. Younger age was associated with non-screening.
Conclusion:
We observed that study participants faced procedural barriers to complete CRC screening and preferred to learn about CRC screening options through their providers. Younger age groups were less likely to receive screening within our study sample. Future, targeted interventions to increase CRC screening should focus on increasing the awareness of the importance of CRC screening and educating patients on the various screening options available and their benefits, especially as they pertain to less invasive tests and targeting younger individuals.
Introduction
Colorectal cancer (CRC) is the second most common cause of cancer-related death 1 and fourth most common cancer with an incidence of 36 new cases per 10 000 people. 2 It also accounts for 7.6% of all new cancer cases in the United States of America (USA). 2 While CRC remains one of the most common causes of cancer-related deaths, CRC-related mortality rates have been decreasing over the past decade from 15.1 per 100 000 people in 2011 to 12.6 per 100 000 people in 2022, 3 largely due to CRC screening.4 -6 If high-risk colorectal polyps or CRC are identified and resected in early stages, the 5-year survival rate for CRC can be as high as 65%. 7 Therefore, many efforts have been taken over the last several decades to increase awareness of, and access to, CRC screening.8,9 Recommended CRC screening tests include fecal immunochemical test (FIT), fecal occult blood test (FOBT), virtual colonography, flexible sigmoidoscopy, and colonoscopy. The US Preventive Services Task Force (USPSTF) recommends that the general population begin screening at 45 years old with subsequent CRC screening happening regularly thereafter. 10 However, despite the recommendations from the USPSTF and the importance of CRC screening in preventing CRC-related deaths, the uptake of CRC screening in the population is suboptimal, and many still face barriers which prevent their access to screening.
Previous community-based studies have attempted to delineate the barriers and facilitators to CRC screening.9,11 -15 Results have shown that there are many barriers to CRC screening including race,15 -19 ethnicity,14,15,17,18,20 lower income,20 -22 lack of education about the importance of CRC screening,13,21 lack of awareness of different CRC screening options, 9 social beliefs, 12 and lack of a visit to a physician.22 -24 There are also many facilitators including higher income, 21 recommendation from a provider,11,15,23,24 education on CRC screening and the different CRC screening options, 25 and visits to a physician. 11 While these community-based studies have produced helpful knowledge regarding the barriers and facilitators to CRC screening, they are limited by the uniqueness of their study populations and contextual factors. For example, a community-based CRC screening study conducted in Mexico will have underlying cultural, geographical, and social contextual factors making their results less generalizable to other communities. 12 Another community-based study conducted in Denver, Colorado focused specifically on participants’ preference for receiving either a FOBT or colonoscopy, disregarding other possible screening tests which may be beneficial/easier to implement in other populations. 26 Of note, we are unaware of any studies addressing the specific CRC screening needs of community members, and the barriers and facilitators to CRC screening, within the state of Utah.
Historically, CRC screening rates for adults aged 50 to 74 years in Utah have been largely similar to those for the USA in general (in 2020 Utah screening rates were 75.6% while the USA screening rates were 73.9%). 27 However, a closer look at Utah CRC screening rates shows that rates have varied across location, race, ethnicity, education, and other sociodemographic factors. For example, the 2020 CRC screening rate for the Salt Lake County Health District (in northern Utah) was 76% while the screening rate for the San Juan Health District (in southeast Utah) was 43%. 28 Additionally, CRC screening rates for Blacks (71.8%), Pacific Islanders (64.3%), Asians (57.3%), and American Indians/Native Alaskans (53.1%) residing in Utah all fell below the Utah state CRC screening average for all races (72.1%). 29 They also fell below the USA screening rates for Blacks (75.3%), Pacific Islanders (65.6%), Asians (65.6%), and American Indians/Native Alaskans (61.1%). 3 These disparities in screening call for a closer, community-based look at barriers and facilitators to CRC screening within the state of Utah to identify potential areas where interventions may be most beneficial in improving CRC screening uptake.
The purpose of our study was to identify barriers and facilitators to CRC screening among a community-based population in Salt Lake County, Utah in order to inform future efforts to develop effective, targeted interventions to increase colorectal cancer screening in this population.
Methods
Study Design
This was a cross-sectional study of adults attending community health events in Salt Lake County, UT. The study was approved by the University of Utah Institutional Review Board (IRB_00123254).
Study Population
We conducted a survey with a convenience sample of adults attending 1 of 6 community health events in the Salt Lake County in 2019. At each event, the research team administered study questionnaires to participants who spoke English or Spanish and were age 45 or older. We excluded those with a previous diagnosis of CRC, inflammatory bowel disease, or a familial cancer syndrome. Questionnaires were accompanied by a consent cover letter and consent was implied with completion of the questionnaire. Participants received a $5 gift card upon survey completion. All health fair attendees were provided with CRC screening information, regardless of whether they participated in the study.
Data Collection
We designed 3 questionnaires for this study: 1 for participants who had discussed CRC screening with a provider and received screening, 1 for those who had discussed CRC screening with a provider but did not receive screening, and 1 for those who did not discuss CRC screening and did not receive screening. Surveys were designed to identify barriers and facilitators to CRC screening based on the current literature. They were translated into Spanish by a professional translation company; the translation was verified by a native Spanish speaker with a certification in medical interpreting (NF). Questionnaires were completed on paper and entered into an electronic database (REDCap). Free response questions in Spanish were translated into English by a member of the study team.
Statistical Analysis
Responses to barriers and facilitator items were reported descriptively. The federal poverty threshold was calculated based on annual income and household size. 30 Univariate analysis was used to measure the association between screening status and participant factors such as age, race, ethnicity, education, marital status, employment, insurance status, whether or not the participant reported a visit with a physician in the past 12 months, language, and federal poverty level. This analysis was conducted for all participants as well as separately for participants ≥50 years of age because the guidelines recommending screening for individuals age 45 were recently released. 10 Using predictors with a P-value of <.05 in the univariate analyses, logistic regression analysis was conducted for all participants and then separately for those ages 50+. Results for the multivariate analyses were considered statistically significant at P < .05. All analyses were completed using R 4.2.2,“dplyr” package, and STATA BE 17.0.
Results
One hundred and seventeen participants participated in the study. A total of 70 (59.3%) participants had received some type of screening before, 17 (14.4%) reported no screening but had discussed it with a medical provider, and 30 (25.4%) participants had not received screening and had never discussed screening with a medical provider. Of those who had received screening, 57 (81.4%) had a colonoscopy, 18 (25.7%) had a stool test, 6 (8.6%) had a flexible sigmoidoscopy, 5 (7.1%) had a virtual colonography (CT colonography), 1 participant (1.4%) was not sure which test they had, and 2 participants (2.9%) marked “other.” Most participants were between 50 and 60 years old (43.6%), White (36.8%) and non-Hispanic (51.3%). A total of 23.7% enrolled participants were Spanish-speaking. Regarding educational and health insurance status, 47% had a college degree or higher, and 75.2% possessed any kind of health insurance. See Table 1 for detailed information about participant demographics.
Participant Characteristics.

One missing value.
2-5 missing values.
6-10 missing values.
11 or more missing values.
Poverty threshold defined as 1-2 person household with income <$15 000, and 3+ person household with income <$30 000.
Barriers to CRC Screening
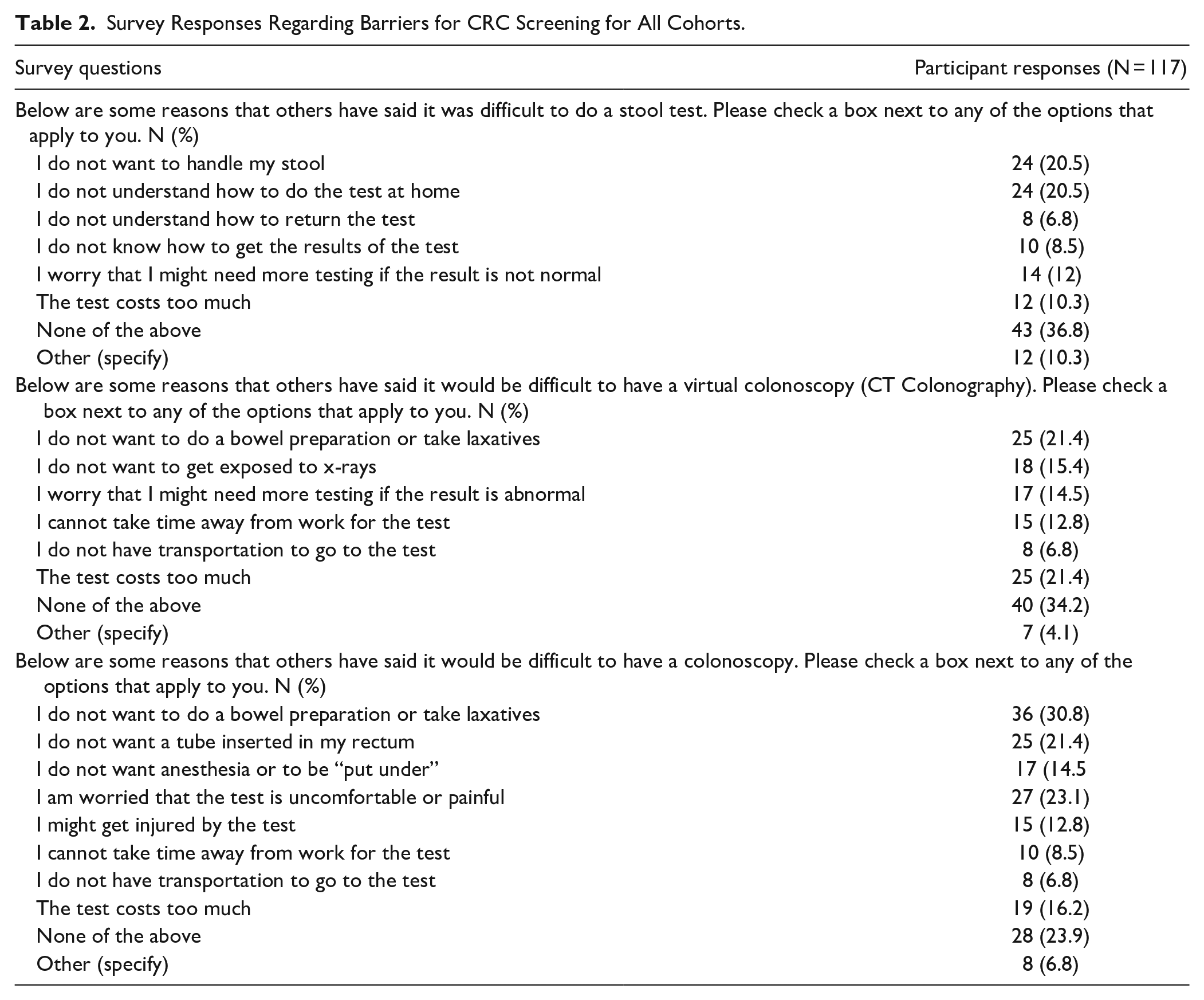
Participants identified several barriers to the different types of CRC screening. Commonly cited barriers to completing a stool-based test were “I do not want to handle my stool” (20.5%) and “I do not understand how to do the test at home” (20.5%). While 36.8% of participants answered “None of the above” for barriers to stool-based screening, some (10.3%) answered “other” and included remarks like, “Haven’t heard from anyone,” and “I feel the result cannot be as accurate.” Commonly cited barriers to completing a virtual colonoscopy or CT colonography were “I do not want to do a bowel preparation or take laxatives” and “the test costs too much” (21.4%), though over a third (34.2%) of participants answered “None of the above.” “Other” (4.1%) responses on the barriers to a virtual colonoscopy included “Haven’t heard from anyone” and “not diagnostic enough.” The most common barrier to completing a colonoscopy screening was “I do not want to do a bowel preparation or take laxatives” (30.8%), however, 6.8% said “other” and included responses such as “It is kind of embarrassing” and “no discussion with anyone” (Table 2). Study participants who discussed screening with a provider but did not receive screening also cited “I do not need the test because I feel fine” (11.8%) as a reason for not receiving screening. However, a majority of this cohort (47.1%) answered “none of the above” when asked to give a reason for not receiving screening (Supplemental Table 1).
Survey Responses Regarding Barriers for CRC Screening for All Cohorts.
Facilitators to CRC Screening
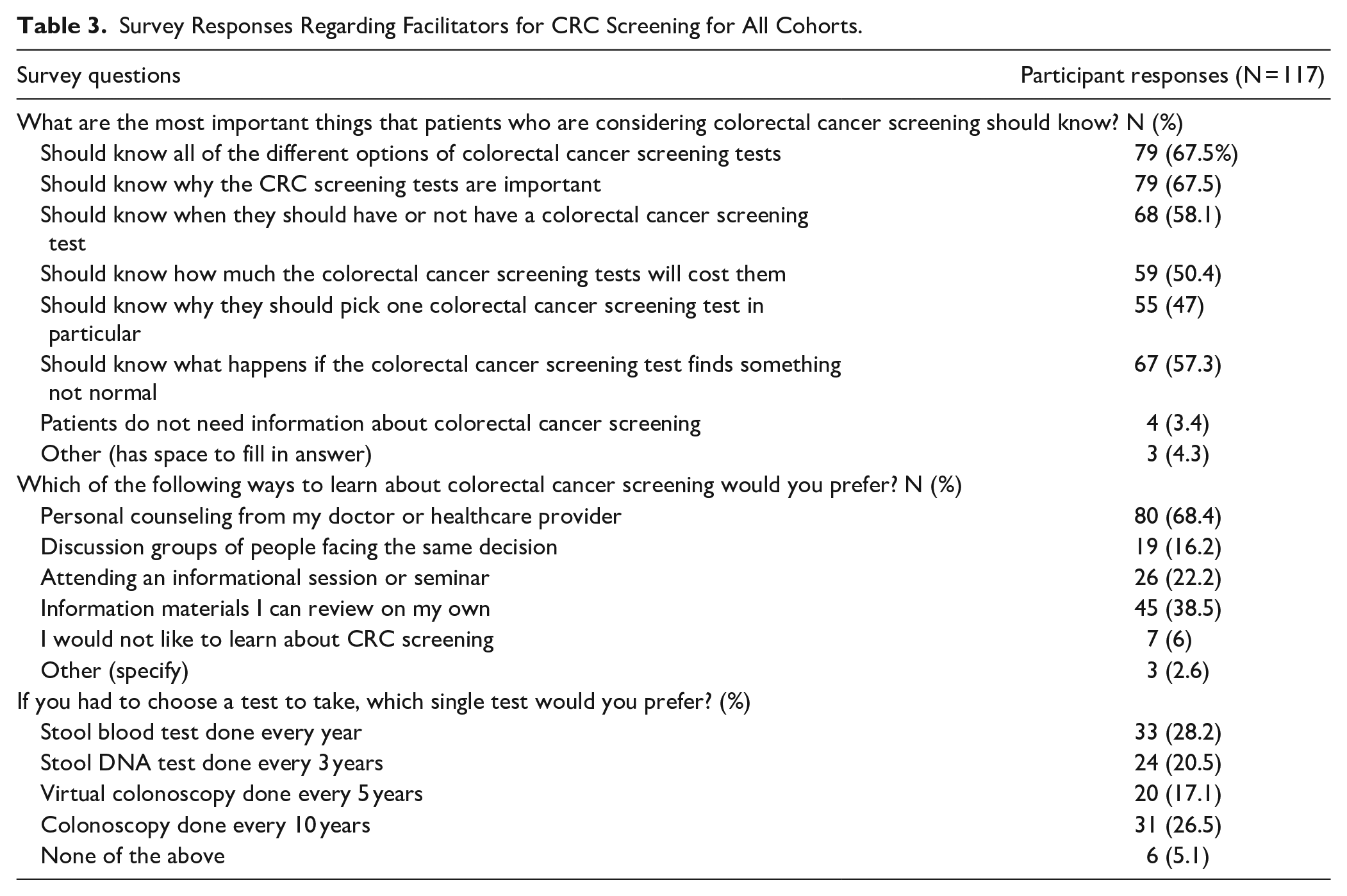
Participants also identified several facilitators that helped or would help them to complete CRC screening. These facilitators highlighted the type of information that participants thought useful about CRC screening and how participants preferred to receive that information. For example, 67.5% of participants felt that patients who are considering CRC screening should know all of the different options of CRC screening available, as well as why the CRC screening tests are important. The majority of participants (68.4%) preferred to learn about CRC screening from their doctor or healthcare provider. A few participants also indicated that they would like to learn about CRC screening through “webex online workshop” and “YouTube” (Table 3). Of those who had received screening, 70% cited a recommendation from their doctor as the number one reason they underwent CRC screening. A little over half (52.9%) received CRC screening information from their doctor, while 54.3% reported that a family member helped them make the decision to screen (Supplemental Table 2). Of those who did not receive screening but discussed screening with a provider, 58.8% said that they received information about CRC screening from their provider, and 35.3% said that a family member helped them make the decision about CRC screening (Supplemental Table 3).
Survey Responses Regarding Facilitators for CRC Screening for All Cohorts.
Demographic Barriers and Facilitators
Univariate and multivariate analyses
The univariate analysis performed for the entire cohort identified several factors associated with non-screening. These included younger age, lack of college education, employment, no health insurance, lack of a physician visit in the past 12 months, and being an English speaker (all P < .05). In the multivariate model for the entire cohort, younger age was associated with non-screening (Supplemental Table 4). In the separate univariate analysis including only those 50 years of age and older, younger, white, married, employed participants with no college education and lack of health insurance, who were English speaking, and lived above the poverty threshold were less likely to get screened (all P < .05). In the multivariate model limited to age ≥50 years, younger age and lack of insurance were associated with non-screening (P < .05) (Supplemental Table 5).
Discussion
This study used a community-based sample from Salt Lake County, Utah to identify barriers and facilitators to CRC screening to ultimately inform future interventions aimed at improving CRC screening rates in this community. Participants most often cited procedural barriers to completing CRC screening. The common responses noted as barriers were: “I do not want to handle my stool,” “I do not understand how to do the test at home,” and “I do not want to do a bowel preparation or take laxatives.” Participants expressed a desire to learn about the different types of CRC screening tests available and preferred to learn about CRC screening through their healthcare providers. For participants who had already received CRC screening, a majority of them cited a recommendation from their doctor as the number one reason for them completing CRC screening, as recommended. Most participants who discussed CRC screening with a provider but did not receive any screening tests thereafter did not choose a reason for not receiving screening, and instead answered “none of the above.” In the multivariate analysis for the entire cohort as well as the multivariate analysis for those ≥50 years, younger age was an important indicator for non-screening.
While our participant responses in general showed a lack of understanding, fear, embarrassment, or disgust for all the different CRC screening tests, research shows that less invasive CRC screening methods have higher levels of uptake among patients.26,31 In further support of this idea, the majority of our study participants preferred stool-based tests as their preferred method for CRC screening. This is similar to findings by DeBourcy et al 26 who found that 53% of their study participants preferred FOBTs to colonoscopies due to the convenience and ease of FOBTs. Other literature comparing the benefits of different CRC screening tests reported that people are more likely to participate in CRC screening when FIT is offered versus when a colonoscopy is offered. 32 This may be due to the simplicity, convenience, and low requirements of completing a FIT.26,33 Most providers recommend a colonoscopy as a CRC screening procedure because of its diagnostic accuracy and because of a colonoscopy eliminating the need for any CRC screening for up to 10 years.32,33 However, other less invasive screening tests hold value for those individuals who need easier access to CRC screening and simpler testing methods. 26 We recommend that patients be made aware of different CRC screening options and their advantages and disadvantages, so as to be able to make an informed decision. However, further research is warranted to study the effectiveness of such a self-efficacy promoting educational approach.
Medical providers play a vital role in creating awareness and educating patients on the benefits and risks of CRC screening. 23 Our study participants cited receiving information from their provider as their most preferred way to learn about CRC screening. Additionally, those study participants who had already received CRC screening cited a recommendation from their provider as the number one reason for completing screening, highlighting the importance of improving access to care. However, some of our participants did discuss screening with a provider and yet did not opt to receive any CRC screening. About half of the participants who failed to receive any CRC screening did not disclose a reason for their choice to not screen. This suggests that a simple recommendation from a provider may not be enough for a subset of the population. Peterson et al 23 recommend that provider recommendations be coupled with improved patient-provider communication regarding CRC screening, such that improvements should be made to the quality of the conversation, rather than focusing on whether or not the conversation occurred. In another community based study, results showed that a good patient-provider relationship was a key facilitator to increasing CRC screening.12,34 Increased quality time with a patient has the potential to improve outcomes and increase compliance to treatment as previously reported by Drossman et al. 34 This may be due to increased trust and communication between provider and patient. 34 Another study found that adherence to CRC screening guidelines was most successful when education about CRC screening and easy access to screening, such as mailing a FIT, were paired together. 20 It may be beneficial for providers to tailor their CRC screening discussions to the patients’ needs, offering information on different CRC screening options that the patient can access and complete. This will improve patient-provider communications by providing more in-depth knowledge about the different CRC screening options and their benefits.
Our multivariable analysis demonstrated that younger age and lack of insurance are associated with non-screening. Lack of insurance can be a barrier from a patient perspective due to cost as well as the provider perspective, as providers may be more reluctant to give a recommendation for cancer screening to patients without insurance.13,19,24 Improving access to care and insurance may help patients and providers overcome the cost of screening. Regarding age, it is important to note that our study was conducted soon after USPSTF changed the recommended screening age. 10 Because of a previous lack of recommendation for CRC screening in younger ages, these age groups may not know that they are eligible to get screened at an earlier age. However, our findings were similar to findings in an older, community-based study where age was the only significant sociodemographic risk factor for non-screening. 11 This is particularly concerning as CRC incidence in those aged 45 to 49 is increasing.4,5,35 Early detection of CRC leads to better outcomes, due to CRC being easier to treat at earlier stages.4,36 We recommend that future campaigns should focus on increasing awareness about the importance of CRC screening specifically for younger populations.
Unlike other studies,15 -19,37 we did not find race or ethnicity to be statistically important facilitators or barriers to CRC screening amongst our study population. However, while race and ethnicity were not statistically significant in our study, they remain important factors when analyzing barriers and facilitators to CRC screening in Utah. While Utah’s CRC screening rate has been historically similar to that of the US, the screening rate for Hispanic adults in Utah is almost 10% lower than the US Hispanic adult screening rate (43% vs 53%).38,39 Additionally, CRC screening rates for Blacks, Pacific Islanders, Asians, and American Indians/Native Alaskans all fall below the Utah state CRC screening average for all races (72.1%). 29 The different findings in our study could be attributed to the fact that our survey was dispersed at local health fairs, where there could be a greater proportion of people with a desire to be healthy and who are up to date on their healthcare needs. The importance of this topic and the disparities outlined warrants further research to determine the CRC screening needs of different races and ethnicities in Utah.
Our study has several limitations. First, we recruited participants from community health events. This can potentially lead to selection bias as most people attending community health events tend to have a greater desire to be healthy and focus more on improving their health. However, these community events were intended to reach underserved populations, thus potentially expanding the reach of our survey to those community members who ordinarily would not have participated in a study like ours in a conventional health setting. Second, our study enrolled a community-based population from Utah, potentially limiting generalizability to other populations. We were also unable to distribute the survey in other counties within Utah. However, we conducted the study in the most populous county in Utah hoping to capture many, diverse perspectives that can be applicable to other areas in the state. Finally, we were unable to collect information on gender and sex and are therefore not able to comment on how these factors affect colorectal cancer screening behaviors and attitudes.
Conclusion
CRC screening is highly effective at preventing CRC-related deaths, but many populations still have difficulty accessing screening and the CRC screening uptake is suboptimal. We observed that study participants primarily face procedural barriers to CRC screening and consider a recommendation from their doctor regarding CRC screening as an important facilitator. We also reported that participants generally prefer to learn about different CRC screening options and their benefits from their healthcare provider, and that younger or uninsured individuals are less likely to get screened. We recommend that providers give more information to patients on all CRC screening tests, especially the less invasive ones (such as stool-based tests), as their uptake is better than more invasive tests like colonoscopy. We also recommend that CRC screening campaigns should especially be tailored to younger age groups in order to increase CRC screening among this demographic age group. Further research is needed on the potential benefits of such efforts.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319251316659 – Supplemental material for Barriers and Facilitators to Colorectal Cancer Screening Among Health Fair Attendees in Utah
Supplemental material, sj-docx-1-jpc-10.1177_21501319251316659 for Barriers and Facilitators to Colorectal Cancer Screening Among Health Fair Attendees in Utah by Jordan E. Johnson, Svenja Pauleck, Andrea J.H. Williamson, Maranda Pahlkotter, Federica S. Brecha, Nathaniel Ferre, Nancy Ortiz, Robin L. Marcus, Sheetal Hardikar and Jessica N. Cohan in Journal of Primary Care & Community Health
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Utah Cancer Action Network [NU58DP006321].
Ethical Considerations
This study received ethical approval from the University of Utah IRB (approval IRB_00123254) on August 14, 2019.
Consent to Participate
Participants were given a consent cover letter for review before starting the surveys. If the participant chose to continue with the survey, consent was implied. The need for a signature documenting consent was waived.
Consent for Publication
Not applicable.
Data Availability
The datasets generated during and/or analyzed during the current study are not publicly available due to sharing limitations in the consent cover letter and University of Utah policy, but are available from the corresponding author on reasonable request and with appropriate IRB and data sharing agreements.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.