
Abstract
Introduction/Objectives:
Obesity data is typically obtained from national population surveys, while the use of more accurate electronic medical record (EMR) data is underutilized. The objective of this study is to calculate current obesity prevalence and weight trends using EMR data and compare the results to prior survey-based obesity prevalence projections for the state.
Methods:
This retrospective study analyzed Body Mass Index (BMI) from deidentified EMR data from 16,491 adult patients in urban midwestern primary care clinics between January 2017 and October 2021 for obesity prevalence and weight trajectories, stratified by age and gender.
Results:
There was a large discrepancy between the survey-based self-reported rates of obesity (35.5%) and those calculated from baseline EMR data (47.6%), along with a smaller discrepancy in females (47.9%) compared to males (47.2%). Young adults aged 20 to 29 years showed a larger increase in BMI over time compared to other age groups
Conclusions:
EMR-derived data indicates a prevalence of obesity greater than projections that have been based on self-reported survey data as well as higher weight trends than projected for this midwestern state. As evident from our study, cohorts such as at-risk young adults with a more rapid weight gain trajectory should be prioritized for enhanced obesity management.
Introduction
The rising prevalence of adults with obesity in the United States over the past 3 decades continues to be a public health concern. In 2018, the prevalence of obesity among U.S. adults was 42.4% and by 2030, 81.0% of adult males and 74.9% of adult females are projected to be overweight or obese, which would result in a doubling of obesity rates in just 12 years.1,2 In Nebraska, the self-reported obesity prevalence was 35.3% in 2022, obtained from the Behavioral Risk Factor Surveillance System (BRFSS), a nationally representative telephone survey. 3 Ward et al 4 projected that the prevalence among Nebraska adults will be greater than 50% by 2030.
Obesity is defined by a body mass index (BMI) ≥ 30.0 kg/m2, and severe obesity is defined by a BMI ≥ 35.0 kg/m2 (https://www.cdc.gov/obesity/adult/defining.html and https://www.cdc.gov/obesity/basics/adult-defining.html). It is a significant risk factor for morbidity and mortality of diseases such as hypertension, coronary artery disease, type 2 diabetes, cerebrovascular disease, and many types of cancer, all of which are among the leading causes of death in the U.S. and worldwide.5 -11 Obesity impacts mental health as well, leading to depression, low self-esteem, discrimination, and social bias.12,13 Additionally, it has significant cost implications for the healthcare system, with a consensus that as BMI rises, so do the healthcare costs.1,3,14 From a clinical perspective, it is important to understand obesity incidence and rates given the aforementioned risks and impacts.
Most population data on obesity is based on survey data, such as the CDC-administered National Health and Nutrition Examination Survey (NHANES), 15 or the Behavioral Risk Factor Surveillance System (BRFSS). 16 The cost of a single BRFSS survey phone call has ranged from $40 to $102, 17 and recent costs are $25 for a single internet panel, but declining response rate and rising costs have prompted the search for alternative data collection. 18 While no direct comparison of self-reported survey data and EMR-derived data is evident in a review of the current published literature, it is likely that using EMR data to track population obesity levels is more cost-effective than surveillance studies.
Researchers have utilized primary care electronic medical record (EMR) data to analyze real-time population weight data and trends in Washington and Wisconsin.19,20 Others used EMR data to model weight trajectories to determine association with behavioral and psychosocial characteristics. 21 Some researchers have focused weight trend EMR studies on childhood obesity22 -24 or surveillance of patients having undergone bariatric surgery or other weight loss programs.25 -28 Such studies highlight the benefits of large-sample EMR-based research with the eventual goal of improving quality and efficiency of health care. 29 Leveraging pragmatic clinical measurements from primary care and community settings can be cost-effective and patient-centric, and support the ultimate aim of “strengthening the patient-clinical relationship, promoting communications about things that matter, helping the patients know more about their health and facilitating their involvement in their own care.” 30
Longitudinal studies suggest that weight trajectories traditionally peak in midlife and later stabilize and slow down or decline in the elderly. 31 Weight gain over time has been associated with increased risk of mortality. Maintaining a normal and stable weight across adulthood is important and preventing weight gain in early adulthood may prevent premature deaths in later life. 32 Such studies on BMI trajectories are often limited by recalled weight, 32 or lower age cut-offs at age 30 or 40 years.33,34 However, emerging data is suggesting that weight gain is occurring at younger ages faster and that different age groupings may need to be included, such as young adults in the 20- to 29-year age group. 32
While rates of obesity for the state of Nebraska have been projected based on self-reported surveys, accurate information from a large cohort across the adult age span is not currently available. The overall goal of our study was to utilize EMR data to calculate the current obesity prevalence in urban Nebraska, determine weight trends over the past 5 years, and compare the results to Ward et al.s 4 projections for 2030. Our specific aims were to use retrospective EMR patient data to 1. identify current obesity prevalence and weight trends for all adults (from the age of 20 years) and 2. identify subgroups of individuals (by decade of age) with increasing weight trajectories. Such information can impact direct patient care by allowing primary care providers to target these groups for enhanced weight management counseling and education and identify areas that would benefit most from public health messaging to facilitate healthy living choices and to prevent additional weight gain.
Methods
This retrospective EMR study cohort consisted of living adults aged 20 years old and above who were seen in urban primary care clinics affiliated with an academic medical center in Nebraska between January 2017 and October 2021. Patients who were deceased or pregnant were excluded. Those included in the study had 1 weight recorded in the EMR in January 2017 and at least 1 other weight measurement recorded in the EMR between January 1, 2017, and October 31, 2021. Deidentified BMI data, along with demographics including age, gender, ethnicity, and race, were extracted. In most cases, BMI was automatically calculated in the EMR. In about 12% of cases, the extracted data did not include BMI; in those cases, BMI was manually calculated based on the provided height and weight. Age was grouped into 10-year intervals, as seen in other studies on weight trajectories. 32 The average BMI was calculated for each age group for both females and males.
Descriptive statistics were used to calculate the frequencies and percentages of the demographics, obesity prevalence for females and males, and overall obesity prevalence. Change in BMI during the study period was calculated for each age group for both females and males by subtracting the BMI in January 2017 from the BMI in October 31, 2021. The IRB deemed it did not need to be reviewed because the data was de-identified.
Results
The number of patients fulfilling the criteria for review was 16,491, comprising 390,407 weight measurements with a mean of 23.7 weight measurements (SD = 23.3) per patient during the 5-year study period. The sample was made up of 59.7% females and 40.3% males. The study sample had a mean baseline age of 54.3 years (SD = 1.71) and a mean baseline BMI of 30.6 (SD = 7.1). Further sample demographics are presented in Table 1.
Baseline Characteristics of the Study Population.
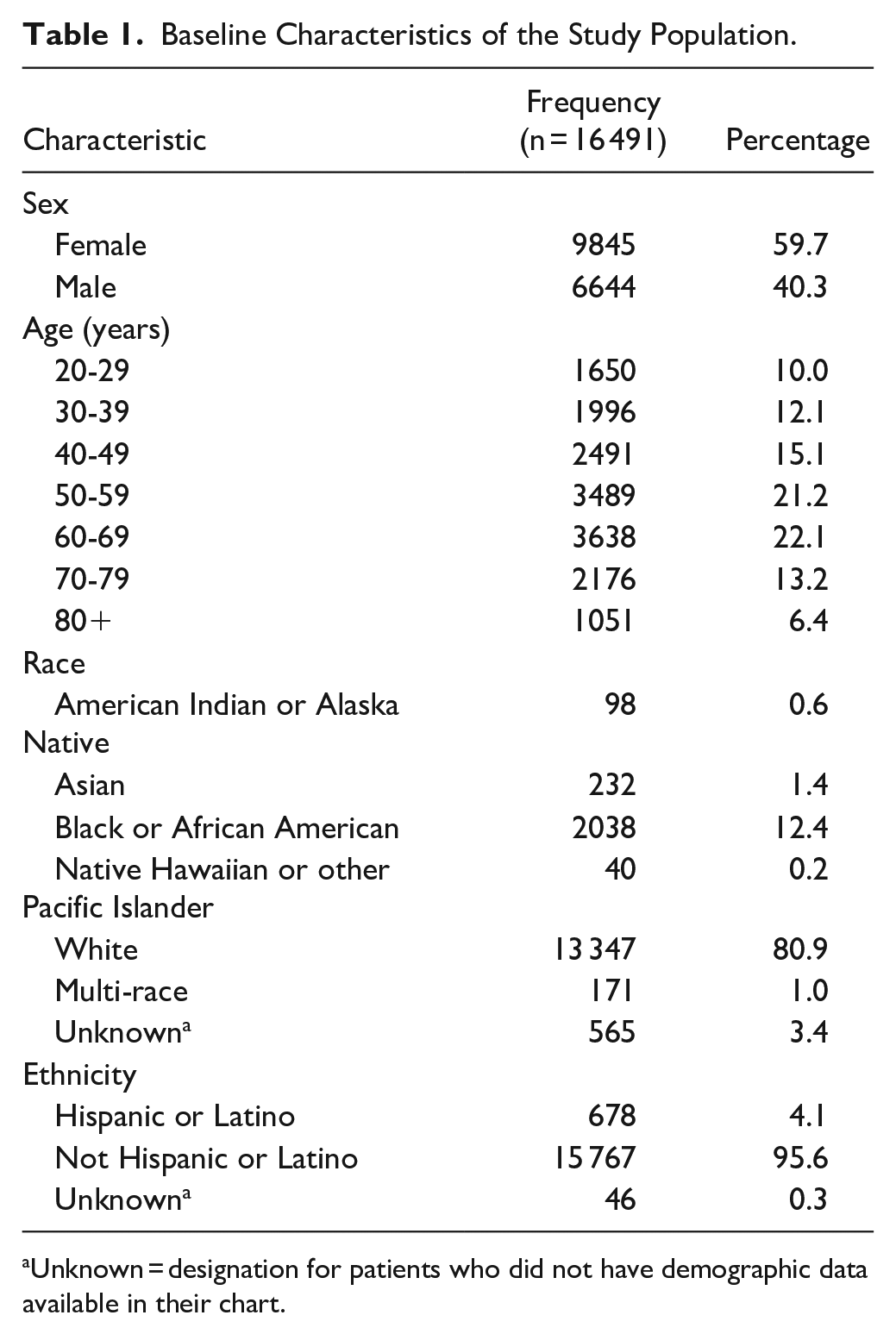
Unknown = designation for patients who did not have demographic data available in their chart.
Among the study sample, the prevalence of obesity at baseline was 47.6% (95% CI = 46.8-48.3) and the prevalence of severe obesity was 24.0% (95% CI = 23.4-24.7). The obesity and severe obesity prevalence by gender is presented in Table 2. Figures 1 and 2 further illustrate prevalence of obesity over time, broken down by age group and gender.
Prevalence of Obesity and Severe Obesity.

Abbreviation: CI, confidence interval.

Female obesity prevalence by age group from January 2017 to October 2021 (BMI ≥ 30.0 kg/m2).

Male obesity prevalence by age group from January 2017 to October 2021 (BMI ≥ .0 kg/m2).
During the study period, the average BMI of females increased among patients aged 20 to 29 years by 1.24 (95% CI = 1.03-1.46), 30 to 39 years by 0.65 (95% CI = 0.43-0.86), and 40 to 49 years by 0.41 (95% CI = 0.22-0.60). The average BMI of males increased among patients aged 20 to 29 years by 0.68 (95% CI = 0.44-0.92), 30 to 39 years by 0.21 (95% CI = −0.01-0.43), and 40 to 49 years by 0.09 (95% CI = −0.10-0.27). The average BMI among both females and males aged 50 to 80+ years decreased. Table 3 and Figures 3 and 4 depict the trend in BMI over the course of the study period, broken down by age for females and males.
Weight Trend Among Adults From January 2017 to October 2021.

Abbreviations: CI, confidence interval; SD, standard deviation.

Female average BMI (kg/m2) by age group from January 2017 to October 2021.

Male average BMI (kg/m2) by age group from January 2017 to October 2021.
Figure 5 compares the 2021 Nebraska obesity prevalence to the 2030 projections reported by Ward et al. 4

Nebraska obesity and severe obesity prevalence in October 2021 from this study compared with 2030 projections for Nebraska and the U.S. reported by Ward et al. 4
Discussion
Our study provides the actual prevalence of obesity and weight trajectories over 5 years in adults across the age span in our midwestern state. It updates previous projections for our state that were based on self-reported data using EMR data. This methodology is emerging as a pragmatic approach to answer primary care research questions with accuracy and efficiency, and our study is indicative that a large sample study can leverage information from the clinical setting to inform providers and public health stakeholders.
In our study, obesity is widely prevalent, impacting half of the population under 70 years of age. There is a large discrepancy between the self-reported rates of obesity from the 2022 BRFSS (35.3%) and those recorded in the medical records in our study (47.6%). There could be several reasons for this discrepancy. The most commonly reported factor in other studies is self-report bias in both males and females.35 -37 Another factor that may contribute is the use of obesogenic medications, including psychiatric medications such as anti-psychotics, mood stabilizers, and antidepressants, as well as the use of long-term oral steroids, hormone-based chemotherapy, and other pharmacologic agents.38 -42 Other contributing factors may include psychosocial factors, health disparities, disability, and other medical conditions that may lead to weight gain.43 -45 However, our study would suggest that, compared to self-reported data, EMRs can provide greater accuracy in weight and BMI and yield data that is reflective of what clinicians can anticipate seeing in practice. The greater prevalence of obesity in female patients in our study is consistent with emerging trends in other countries and, more recently, in the United States,1,2,46 -50 which has prompted obesity gender disparity research.
Our study also determines the weight trajectories throughout adulthood, and we note a more rapid rise in both male and female young adults (20-29 years) compared to any other age grouped by decade. They had the greatest change in BMI and trends in weight gain, compared to all other age cohorts, with implications for adverse impacts on mortality. 32 This finding is similar to emerging national trends,51 -53 and should be of considerable concern to clinicians, as young adult weight gain can have considerable impact on health outcomes later in life.54,55 There are many possible reasons for this weight gain among young adults, including an unhealthy lifestyle with increased screen time. The CDC has identified increased screen time (the amount of time one spends on an electronic device such as TV, smartphone, tablet, laptop, computer, and/or video games) as an important public health concern due to its link to poor health outcomes and weight. 56 The negative impact of increased screen time on weight gain among children and adolescents has been intensely studied.57 -60 It is known that screen time is often a sedentary behavior and leads to decreased physical activity, which may further exacerbate the impact on weight gain and obesity.61 -64
A meta-analysis of observational studies found a positive association between physical inactivity and sedentary behaviors with obesity among adults. 65 Additionally, some researchers have found a negative impact of consuming foods higher in sugar, saturated fat, refined grains, and processed foods on weight gain and obesity.66 -68 Similarly, increased consumption of sugar-sweetened beverages (SSBs) have been linked to rising rates of childhood and adult obesity.69 -71 Nebraska was the fifth-highest state in purchasing SSB per capita. 72 Future clinical and community interventions targeting the prevention of further weight gain would likely benefit from efforts to decrease screen time and other sedentary activities, increase physical activity, and increase consumption of nutritious foods while decreasing consumption of calorie-dense, non-nutritious foods.
Obesity stigma plays multiple roles in the obesity epidemic. First, the stress associated with weight stigma has been linked to overall worse physiological health status including a higher risk of obesity, diabetes, hypertension, and many mental health conditions, which can lead to a vicious cycle of weight gain and ongoing weight stigma.73 -75 Additionally, those who perceive weight stigma by healthcare providers may be discouraged from seeking care or have more barriers preventing weight loss.76 -78
While we noted a BMI increase among young adults, those aged 50 to 80+ years of age were noted to have a slight decrease in BMI during the study period. These findings may be consistent with what is known as sarcopenic obesity, which is a combination of unhealthy excess body fat with loss of fat-free mass including muscle and bone.79,80 Another possible explanation is unintentional weight loss from chronic medical conditions including cancer, COPD, and neurodegenerative disorders.81 -83 Ultimately, these findings would be best examined in future research. The use of EMR data in the primary care setting for research is currently underutilized but evolving and with additional clinical information, studies such as this will eventually enhance patient care and outcomes.
This study has several limitations. The results may not fully represent the general population. Younger and healthier patients are less likely to seek healthcare, so this study sample may overrepresent older or medically complex patients. Additionally, the results may overestimate average BMI per age group as patients with higher BMI may have had greater visit frequency. Since the study included patients who received care at an urban medical center, the results do not represent a Nebraska population that is largely rural. The study results were not analyzed by race given that the population in Nebraska and, therefore in our study sample, is primarily white. Further, the study did not account for other medical conditions that may impact weight gain and/or loss. Lastly, most height data recorded in the EMR is self-reported, which may be impacted by self-reporting bias.
Conclusions
Our study indicates that rates of obesity may be increasing more quickly than predicted, and that future interventions should target at-risk younger adults who are displaying more rapid weight gain trajectories. The management of obesity is costly and overwhelming for healthcare systems and communities. A change in the current practice of relying on expensive survey-based or inaccurate self–reported obesity data to the use of inexpensive and more accurate EMR data to assess not only obesity prevalence but for future predictions is evident from our study. Comprehensive and collaborative interventions from both public health and medical experts will be critical for success.
Footnotes
Acknowledgements
We would like to thank Mary Beth Steele for her assistance with manuscript preparation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funded by the University of Nebraska Medical Center.
Ethical Approval
This retrospective study cohort consisted of living, non-pregnant adults aged 19 years old and above who were seen in an outpatient family medicine clinic at a single urban medical center in Nebraska. The IRB deemed it did not need to be reviewed because the data was deidentified.
Data Availability Statement
Raw data were generated at University of Nebraska. Derived data supporting the findings of this study are available from the corresponding author BK upon request.