
Abstract
Introduction
In most recent estimates between 2011 and 2014, the prevalence of obesity in children aged 2 to 19 years in the United States was 12.7 million, about 17% of all children and adolescents. 1 The obesity epidemic has been attributed to increasingly sedentary lifestyles and unhealthy dietary intake. In addition, there are significant physical and mental health outcomes associated with obesity, including cardiovascular disease, diabetes, and depression. To combat this public health issue, the US Department of Health and Human Services has targeted childhood obesity in its Healthy People 2020 campaign to decrease the proportion of children with obesity aged 2 to 19 years by 10% to a target of 14.5%. 2
Multiple socioeconomic factors are associated with overweight and obese weight status in adolescents, including low-income status, inadequate access to healthy foods and limited safe outdoor play areas. This results in limited guidance for children and adolescents on how to make healthy lifestyle choices.3-5 Conversely, positive environmental factors, such as caregiver involvement in meal preparation, access to full-service grocery stores, positive peer support, and family meals have correlated with child and adolescent obesity resilience.6,7
Adolescents’ self-identified challenges to a healthy lifestyle and their association with obesity have yet to be determined. Prior studies have noted the importance of recognizing barriers to adolescent behavior change, as well as the important roles of self-reflection and feelings, rather than environmental factors.8,9 Another study explored how African American adolescents view their obese status and found that they desired more family involvement in healthy weight-related behaviors. 10 A review examined key barriers to healthy lifestyles, including a lack of resources and enablers (personal interest and motivation, family and friends practicing healthy behaviors), but did not report on possible associations with obesity. 11
There are a multitude of factors that can dictate weight status; however, there are limited studies regarding the perception of adolescents and its correlation with weight status. The primary objective of the current study reports on urban pediatric patients’ self-identified challenges to healthy lifestyles and examines multiple social and environmental risk factors associated with pediatric obesity. Identification of self-identified specific risk factors for obesity will allow for targeted clinical guidance and public health interventions to combat the obesity epidemic.
Methods
From May to August 2014, patients aged 9 years or older who presented for an office visit at an urban pediatric clinic were eligible to participate in this institutional review board–approved, cross-sectional study. Patients’ height and weight were gathered at each visit and recorded in their medical record during the study period.
Body mass index (BMI) was calculated from the medical record and reported as BMI-for-age percentiles, according to the Centers for Disease Control and Prevention (CDC) growth charts for the children and adolescents. Those who were categorized ≥95th percentile were identified with obese weight status, ≥85th and <95th percentile was categorized as overweight, ≥5th and <85th percentile was categorized as normal weight, and <5th percentile was categorized as underweight. 12 Caregiver height and weight and education attainment status were also collected as self-reported data. Patients with incomplete BMI data were excluded.
Caregivers consented and adolescents who assented for the study were each given a 20-question survey based on the 2011 CDC Youth Risk Behavior Survey (YRBS) to assess health behaviors and environments in exchange for a $5 gift card. The survey assessed dietary intake of healthy and unhealthy foods, exercise, and environmental factors to identify perceived challenges to eating healthy foods and being active. Dietary intake responses were dichotomized to daily intake vs. less than daily intake for analysis. Exercise was dichotomized with 3 or less days of exercise compared with 4 or more days in the past 7 days. Education levels were dichotomized to a binary variable for analysis.
We refer to the group made up of children and adolescents in our study as “adolescents” and parents and nonparent caregivers as “caregivers.” Data analysis was completed using SAS 9.3 (Cary, NC). Because of the small sample size of adolescents who are underweight, normal weight, and overweight, they were combined as the group without obesity in analysis. Demographic characteristics and factors that were associated with obesity in adolescents were identified using t-test and Wilcoxon rank test for numerical variables and chi-square test, Fisher’s exact test, and logistic regression for categorical variables. A multivariable logistic regression model controlling for confounders was completed with statistically significant variables. All P values presented in tables or figures were 2-sided, with values less than .05 considered as statistically significant.
Results
A total of 132 patients were enrolled in the study. Two were excluded for incomplete height or weight, leaving 130 patients for analysis. All participants self-identified their ethnicity as non-Hispanic black and hold public health insurance. The majority of the adolescents enrolled were categorized as obese weight status (68%); 22 (17%) as overweight status, 18 (14%) as healthy weight status, and 1 (0.8%) as underweight status. The latter 3 groups made up the adolescent group without obesity (32%) (Figure 1).

Demographic composition of 130 adolescents based on weight status.
The mean age of adolescents without obesity enrolled was 14.2 ± 2.7 years and of adolescents with obesity, 13.5 ± 2.4 years. There was no difference in age, gender, and education between adolescents with and without obesity (Table 1). In addition, caregiver age, obesity status, and education were not statistically different between the 2 adolescent groups. However, the calculated BMI of caregivers in adolescents with obesity was higher than adolescents without obesity (36.2 ± 9.7 vs 32.9 ± 7.5 kg/m2), though both are still in the obese weight range.
Comparison of Demographic Characteristics of Non-obese and Obese Adolescents.

Values are mean ± standard deviation (range).
n = survey response number within non-obese adolescents group, survey response number within obese adolescents group.
Statistical significance.
Self-reported dietary and health behaviors based on survey answers were compared between the 2 adolescent groups. Adolescents without obesity reported more frequently engaging in heavy exercise for 30 minutes at least 4 days within the past 7 days (P = .04). This group also reported higher percentages in ever trying to lose weight (P < .0001). Intake of vegetables, fruits, sweetened drinks, and high-fat snacks and daily food preparation at home were not statistically different between the 2 adolescent weight groups. Limited access to healthy foods was also found not to be statistically significant. The only factor that was statistically significant in perceived challenges to eating healthy foods between the 2 groups was that the friends of adolescents with obesity do not eat healthy foods (Table 2).
Comparison of Self-Reported Health Behaviors and Perceived Challenges of Healthy Living of Non-obese and Obese Adolescents.

n = survey response number within nonobese adolescents group, survey response number within obese adolescents group.
Statistical significance.
Perceived challenges to healthy living were also compared between the adolescent groups. Environmental barriers to eating healthy were found not to be statistically different between the 2 groups. Environmental barriers to being physically active were also not statistically significant. An unsafe neighborhood to play outside or a school not offering an after-school program with physical activity may be perceived challenges for adolescents with obesity but were not statistically significant (Table 2).
To adjust for potential confounders, a multivariable logistic regression model controlling for caregiver BMI, self-reported exercising 4 or more days in the past week, trying to lose weight, and friends not eating healthy foods was found to be significant. Exercising 4 or more days still showed a 0.34 decreased odds of being obese (95% CI 0.13-0.93) and a self-report of trying to lose weight showed 11.1 increased odds of being obese (95% CI 4.2-33.3) (Table 3).
Multivariable Logistic Regression Model for Predicting Obesity Based on Survey Responses.
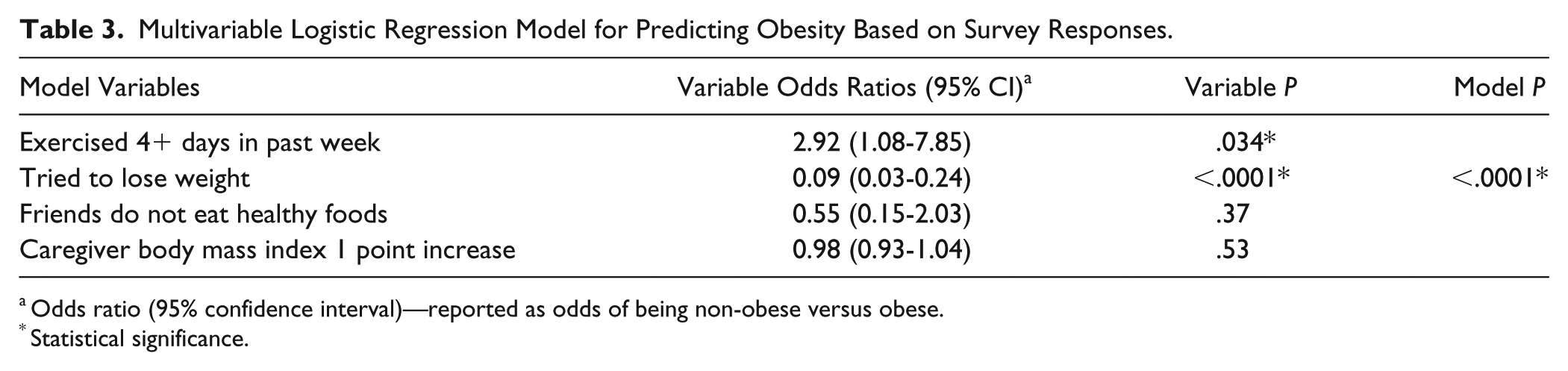
Odds ratio (95% confidence interval)—reported as odds of being non-obese versus obese.
Statistical significance.
Discussion
Our study demonstrated that adolescents with and without obesity perceive and report barriers to living a healthy lifestyle differently. There was no difference in demographic factors between the two groups of adolescents in our study, including caregiver obesity and education, which have been shown in prior literature to be linked to their children’s weight status. 13 We were able to control for a difference in caregiver BMI and found that it was noncontributory, differing from other studies and perhaps showing a complex relationship of environmental factors modifying genetic factors. In other studies, adolescents listed a lack of available healthy foods, lack of family members eating healthy, and less desirable school activity programs as barriers to healthy behaviors.11,14-17 Additionally, it is interesting to see that reporting an attempt to lose weight was significantly associated with weight status, but healthy diet and active behaviors do not seem to be associated with this difference. These differences remain true in our adjusted model.
Our study findings show varying results from what has been published in the literature. Unlike prior studies, we found that adolescents without obesity reported increased exercise frequency compared to adolescents with obesity. 18 In this study, self-reported food intake and healthy food behaviors were not associated with weight status differences. The only factor that was statistically significant was frequent exercise, which decreased odds of obesity by 0.34. In univariate analyses, peer influence in eating healthy was statistically significant, but this did not hold true in the multivariable analysis. While more research into this is needed, this may show that parental influence may not be as significant as previously reported, and the target of office counseling should also be directed at adolescents and their peers. Peer group influences are important to explore and consider in tackling obesity from multifaceted approaches, as supported by past studies.16,19,20
Our study has several strengths and limitations. While some articles use self-reported height and weight, our study objectively measures this data, decreasing underestimates of actual BMI and weight status, as people tend to underreport weight and overreport height.21,22 The survey questions were modeled after a tested and validated national survey for youths. While national surveys include a large population, it is also imperative to assess local trends, as a higher proportion of participants in this study expressed not eating vegetables and fruits and not exercising in the prior week.
A limitation is generalizability to all pediatric patient populations, as our study includes a non-Hispanic Black population with socioeconomic challenges who seek care in an urban clinic. This is a cross-sectional survey, so the frequency of healthy behaviors (eating healthy fruits and vegetables and exercising) may be dependent on school-provided meals, activity, and weather. However, these surveys were distributed during late spring and early summer months, so even when adolescents were in school and families were in nice weather, exercise frequency remained low, as there may be other factors at play, such as neighborhood safety. We were not able to detect differences between healthy weight and overweight adolescents because of the small sample size. Another limitation is that the adolescents may perceive barriers that may not actually be present. Studies have demonstrated that adolescents may fault barriers rather than a lack of self-motivation for healthy behaviors. 23 Another limitation may also be response and recall bias, with a tendency of individuals to report favorable behaviors, which may skew results. Theoretically, both groups of adolescents with obese and non-obese weight status would exhibit these biases.
In this study, we found that an active lifestyle above other factors may contribute to obesity resilience. On the other hand, obese weight status was found in adolescents who had friends who did not engage in healthy behaviors. However, these adolescents with obesity were also less likely to report exercise and more likely to report trying to lose weight. This may suggest additional factors beyond environmental barriers, such as inaccurate perception of true weight status and a lack of knowledge of effective components of a weight loss program. Response bias in reporting socially desirable behaviors could also play a role.
Overall, our study demonstrates the need to further identify what barriers remain between a desire to lose weight and the initiation of behaviors for weight loss, as well as finding ways to encourage more exercise, such as reaching out to patients through peer groups. By knowing the adolescents’ perceived barriers and its associations with weight status, health care and public health professionals can use this information to tailor their clinical treatment and policy guidance.
Conclusion
Our study explored perceived barriers and risk factors associated with obesity in adolescents who may have multiple socioeconomic challenges to healthy lifestyles. Exercise has a significant role in weight status, thus reiterating the call for activity over sedentary behaviors. Health care professionals can improve communication with adolescent patients if they understand that peers may influence weight status compared with family members and adolescents with obesity perceive their condition differently. As obesity is a challenging public health epidemic, clinicians and all health professionals who work with adolescents should be aware of the need to highlight physical movement and that perceptions about barriers may differ between groups.
Footnotes
Acknowledgements
The authors thank Jason C. Ho for his review of the manuscript.
Author Contributions
SKL, AC, and RL conceived and carried out experiments and HL analyzed data. All authors were involved in writing the paper and had final approval of the submitted and published versions.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: SKL and RL received funding from the Ohio Department of Medicaid to conduct this study. SKL and AC received funding from University Hospitals Rainbow Babies and Children’s Hospital for presentations at conferences. SKL received travel support from Mead Johnson to present this research at a resident research symposium.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This program is partially funded by the MEDTAPP Healthcare Access (HCA) Initiative and utilizes federal financial participation funds through the Ohio Department of Medicaid. Views stated in this presentation are those of the researchers only and are not attributed to the study sponsors, the Ohio Department of Medicaid or to the Federal Medicaid Program. MEDTAPP HCA Initiative funding supports teaching and training to improve the delivery of Medicaid services and does not support the delivery of Medicaid eligible services.