
Abstract
Background:
Tobacco smoking exacerbates diabetes-related complications; its prevalence is notwithstanding substantial. Persons with diabetes face a number of barriers and challenges to quitting such as multiple lifestyle restrictions; tailored interventions are required for smoking cessation.
Objective:
To identify research on behavioral interventions for smoking cessation in diabetes.
Methods:
Studies had to be randomized controlled trials, quasiexperimental or systematic reviews. The behavioral interventions included were: the 5As, Cognitive-Behavioral Therapy, Motivational Interviewing, Contingency Management, Health Coaching and Counselling, as compared to standard care. The outcomes were self-reported and/or biochemically verified smoking cessation. CINAHL Complete, MEDLINE Complete, the Cochrane databases of systematic reviews and randomized controlled trials, PsychInfo and PubMed Central were searched until July, 2023. Keywords used included diabetes, smoking cessation and each of the behavioral interventions included.
Results:
1615 papers were identified. Three studies on the 5As/brief advice, 4 on Motivational Intervention and 1 on counseling were retained. The results on the 5As and Motivational Interviewing were conflicting. More intensive interventions appear to be more successful in achieving smoking cessation in smokers with diabetes.
Conclusions:
Future research should focus on the continued development and evaluation of structured smoking cessation interventions based on the 5As, Motivational interviewing and Cognitive Behavioral Therapy.
Background
Introduction
Diabetes mellitus (DM) is a chronic metabolic disorder that poses significant challenges to individual health and public healthcare systems worldwide. This disease affects nearly 422 million people and is directly responsible for 1.5 million deaths, while indirectly contributing to another 17.5 million deaths globally each year. 1 Tobacco smoking is another leading cause of preventable morbidity, and mortality. Tobacco smoking is estimated to lead to the premature death of 6 million people worldwide. 2 Long-term smoking is linked to detrimental health effects, such as the development of cardiovascular disease, chronic respiratory disease and other conditions, that develop over time due to smoking habits. In the general population, individuals who continue to smoke beyond age 40 tend to experience higher levels of pain and disability than non-smokers. 3 Tobacco smoking is also 1 of the most important modifiable risk factors for pre-diabetes and DM. 4 It has also been demonstrated that smoking exacerbates diabetes-related complications and impedes effective self-management. 4 Smoking, for example, substantially increases the risk of cardiovascular disease in both the general population and patients with type 2 diabetes. 5 This increased risk is however more accentuated in persons living with diabetes, as these persons have a twofold additional hazard of cardiovascular disease compared to persons without diabetes 6 ; cardiovascular disease remains the most common cause of mortality among patients with diabetes.7,8
Despite the well-documented risks associated with smoking among individuals with diabetes, the prevalence of smoking in this population is still significant. Durlach et al, estimated the global prevalence of tobacco use amongst individuals with type 1 and type 2 diabetes at 30% and 20%, respectively. 4 Evidence suggests that when compared to other smokers, smokers with diabetes tend to be less motivated to stop smoking, possibly due to several diabetes-related barriers and challenges to quitting. 9 In addition to the commonly reported challenges and barriers to quitting, such as the smoking habit and addiction, individuals living with diabetes have reported that they believe smoking helps them to manage their diabetes, such as, in controlling their blood sugar levels, adhering to their diet and in managing their weight. 10 Living with diabetes and the accompanying required lifestyle changes, is in itself a stressor, and is known to be associated with distress and depression. 10 Persons with diabetes report that they use smoking to cope with boredom, anxiety, depression and stress. 11 All these elements make it additionally difficult for persons with diabetes to stop. 10 As a result, there is an urgent need for targeted interventions to support smoking cessation in people with diabetes.
Intensive smoking cessation support, including behavioral assistance such as counseling and pharmacological options such as nicotine replacement therapy (NRT), bupropion, or varenicline, has been shown to increase the success rate of smoking cessation in the general population. 12 A scoping review on smoking cessation interventions applied to individuals living with diabetes, and the associated specific challenges and barriers to smoking cessation, reported that this approach could also be beneficial for people with diabetes, helping them cope with the unique challenges associated with their condition. 10 However, given the scope of the review, the review authors did not identify specific behavioral interventions to guide clinical practice in this area. While a subsequent systematic review of stand-alone intensive smoking cessation interventions among individuals with diabetes recommends the use of intensive (long and frequent support sessions) interventions for use among this cohort, the limited number of studies and the inconsistent findings limited the ability to draw recommendations on the use of specific behavioral interventions for smoking cessation among individuals living with diabetes. 13 This scoping review, consequently, fills an important gap in the literature in that it seeks to identify which behavioral interventions have been researched to date and could be applied to assisting persons living with diabetes to quit smoking.
Objectives
The objective of this review was to map the research on behavioral interventions to assist smoking cessation in individuals with diabetes; the behavioral techniques which were the focus of this scoping review are the 5As framework for smoking cessation, Cognitive-Behavioral Therapy (CBT), Motivational Interviewing (MI), Contingency Management (CM), Health Coaching and Counselling.
More specifically this review seeks to explore
the extent of research on the above behavioral interventions for smoking cessation for individuals with diabetes,
identify gaps in the research to date and
make recommendations for the development of future research in this area
Methods
The methodological framework for scoping reviews developed by Arksey & O’Malley, as reviewed by Levac, Colquhoun, & O’Brien, was used in the conduct of this review.14,15 This framework includes 5 stages: identifying the research question, searching relevant studies, selecting studies, charting the data and collating it, summarizing and reporting the results. This scoping review is reported in line with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis extension for scoping reviews checklist (PRISMA-ScR Checklist). 16
Review Question and Eligibility Criteria
The review question addressed in this review is “what is the current scope of research on behavioral interventions to assist smoking cessation in persons with diabetes?.”
Specifically, the behavioral interventions covered in this scoping review were:
The 5 As and brief advice
Cognitive Behavioral Therapy
Motivational Interviewing
Contingency Management
Health Coaching
Counseling
In light of this review question, papers were considered to be suitable for inclusion in this review if they met the criteria outlined in Table 1:
The Inclusion and Exclusion Criteria.

Only studies available in the English language were selected, without any time restriction.
Information Sources
The following databases were searched between the 1st and the 30th of July 2023: CINAHL Complete (EBSCO), MEDLINE Complete, the Cochrane database of systematic reviews, the Cochrane database central register of randomized controlled trials, APA PsychInfo and PubMed Central. The reference lists of retained papers were scanned to identify any additional relevant papers. Alerts were set to identify any additional papers published after July, 2023 until the end of October, 2023. A manual search of the bibliography of papers which were retained based on the title and abstract were scanned to assist with identification of any additional relevant studies.
Search Strategy
The following Boolean search strings were used for the databases search:
(diabetes OR diabetes mellitus OR type 1 diabetes OR type 2 diabetes) AND (smoking cessation OR smoking cessation interventions OR quit smoking OR stop smoking) AND (5As OR 3As OR 5A’s OR 3A’s OR brief advice OR brief intervention)
(diabetes OR diabetes mellitus OR type 1 diabetes OR type 2 diabetes) AND (smoking cessation OR smoking cessation interventions OR quit smoking OR stop smoking) AND (Cognitive Behavio?ral Therapy OR CBT)
(diabetes OR diabetes mellitus OR type 1 diabetes OR type 2 diabetes) AND (smoking cessation OR smoking cessation interventions OR quit smoking OR stop smoking) AND (motivational interviewing OR mi OR motivational interview)
(diabetes OR diabetes mellitus OR type 1 diabetes OR type 2 diabetes) AND (smoking cessation OR smoking cessation interventions OR quit smoking OR stop smoking) AND (contingency management)
(diabetes or diabetes mellitus OR type 1 diabetes OR type 2 diabetes) AND (smoking cessation OR smoking cessation interventions OR quit smoking OR stop smoking) AND (coaching OR health coaching)
(diabetes OR diabetes mellitus OR type 1 diabetes OR type 2 diabetes) AND (smoking cessation OR smoking cessation interventions OR quit smoking OR stop smoking) AND (health behavio?r counsel?ing OR individual behavio?r counsel?ing OR counsel?ing OR behavio?r counsel?ing OR health counsel?ing)
Selection of Sources of Evidence
The retrieved papers were initially compared to the inclusion criteria based on their title and abstract by 1 of the reviewers (R.S.); a second reviewer (J.G.) was responsible for checking the results of this initial screening. Those papers retained after this initial selection were independently rescreened on the basis of the full text by 2 of the reviewers (R.S. and J.G.) to ensure that these met the inclusion criteria. This process was facilitated by the use of a template which was developed to allow extraction of the study characteristics. The template included a section to explain the rationale behind each reviewer’s decision on whether the paper should be included in the review, excluded or if the reviewer was uncertain. The 2 reviewers subsequently compared their decisions for each paper and any disagreement was resolved by discussion with the third reviewer (P.C.) until consensus was achieved.
The review process was conducted by using RefWorks (2023) (ProQuest LLC).
Data Charting Process
Data extraction from the retained papers was performed using a data-charting form developed by 1 of the authors (R.S.). The process was iterative, involving 2 reviewers (R.S. and J.G.) who charted the data independently. Any disagreement was then discussed, and the information extracted from the studies was updated accordingly. To guarantee the effectiveness of data extraction, a trial run was carried out with a sample of 4 papers to check for any required amendments before the data were extracted from all the papers. No amendment was required.
Data Items
Data items included the author’s name, year, country, study design, population details, sample size, methods, intervention and control details, measured outcomes, time intervals at which outcomes were assessed and study results.
Synthesis of Results
Given the heterogeneity in behavioral therapies tested in the studies included in this scoping review, a narrative approach was used to synthesize the results for each behavioral therapy.
Results
Papers Included in the Review
The PRISMA flow chart presented in Figure 1, provides a trail of the selection of studies on the behavioral therapies which were included in this review, that is the 5As model and brief advice, Cognitive Behavioral Therapy, Motivational Interviewing, Contingency Management, Health Coaching and Counselling. As seen in Figure 1, a total of 1615 papers were identified by the search strategy described in section 2.2 and 2.3.
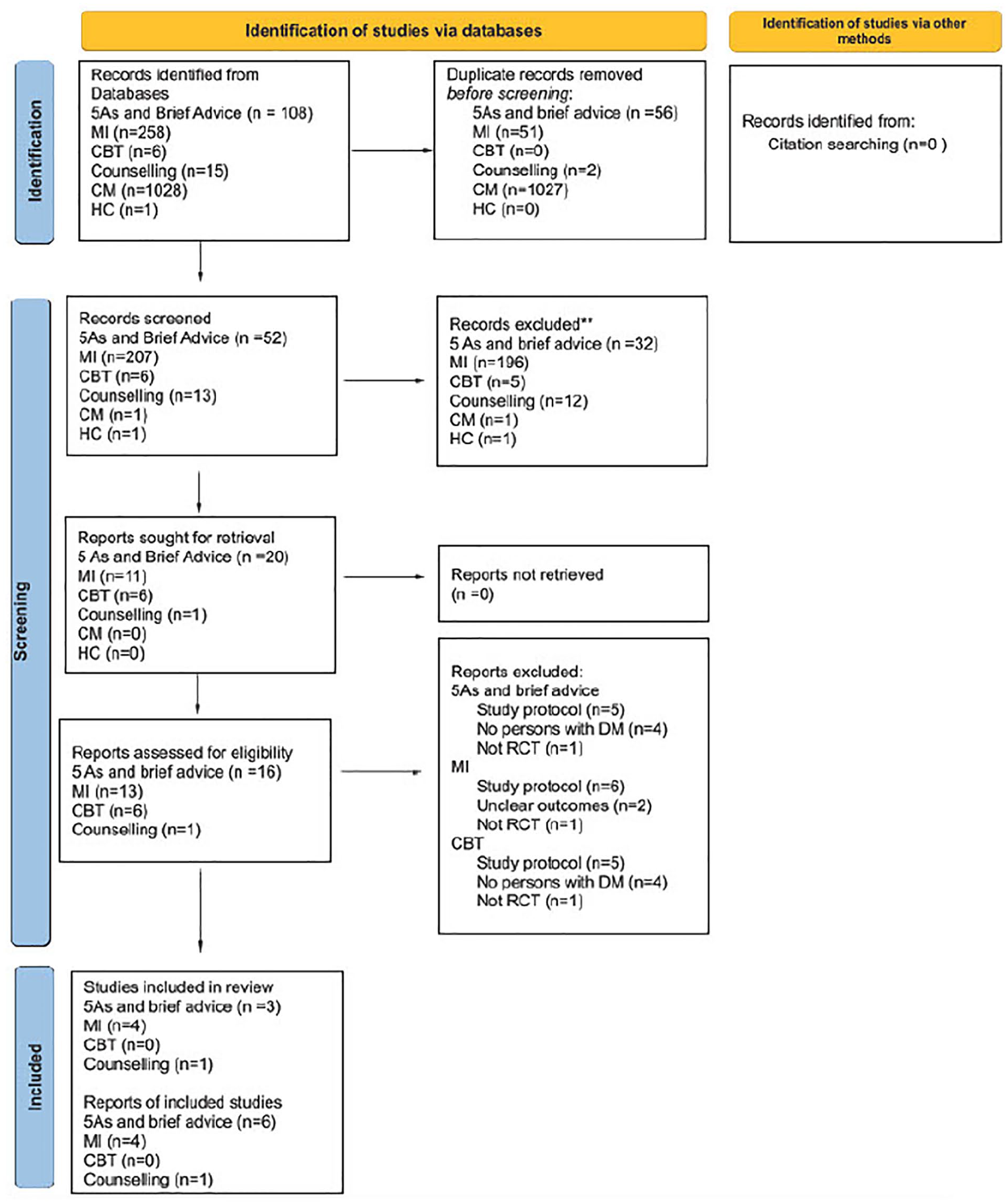
PRISMA 2020 flow diagram for scoping review of behavioral therapy to assist smoking cessation in persons with Diabetes Mellitus.
Of these, 107 hits were related to papers on the 5As and brief advice. As seen in Figure 1, following removal of duplicates and scanning of the papers on the basis of their title and abstract, 16 papers were identified for retrieval. Following assessment of eligibility for inclusion on the basis of the full text, 11 papers were excluded as these were reports of study protocols, did not include persons with diabetes, did not include the 5As or brief advice in their intervention or did not use a randomized controlled design. The alerts set on the databases identified an additional relevant paper in November 2023, which was included in the review. In summary, 6 papers, reporting 3 studies, were retained.
There were a total of 258 hits for motivational interviewing. As seen in Figure 1, following removal of duplicates and scanning of the papers on the basis of their title and abstract, 13 papers were identified for retrieval. Following assessment of eligibility for inclusion on the basis of the full text, 9 papers were excluded as these were reports of study protocols, had unclear outcomes or did not use a randomized controlled design. Four papers reporting 4 studies on the use of Motivational Intervention were retained.
There were a total of 6 hits for Cognitive Behavioral Therapy. As seen in Figure 1, following removal of duplicates and scanning of the papers on the basis of their title and abstract, 1 paper was identified for retrieval. This was not eligible for inclusion in the review as it reported a study protocol. No studies on the use of Cognitive Behavioral Therapy were therefore included in this review.
There were a total of 147 hits for counseling. As seen in Figure 1, following removal of duplicates and scanning of the papers on the basis of their title and abstract, 11 papers were identified for retrieval. Following assessment of eligibility for inclusion on the basis of the full text, 10 papers were excluded as these were reports of study protocols, did not actually use counseling as an intervention, include a survey of nurses’ views on the use of counseling in smoking cessation with persons with diabetes, included both persons living with cardiac conditions and diabetes, but did not present results for the 2 cohorts separately. One study designed the use of counseling as a non-intensive comparison rather than an intervention. One paper reporting 1 study on the use of counseling to assist smoking cessation in persons living with diabetes was retained.
There were a total of 1028 hits for Contingency Management. As seen in Figure 1, following removal of duplicates and scanning of the papers on the basis of their title and abstract, 1 paper was identified for retrieval. This was not eligible for inclusion in the review as it reported a study protocol. No studies on the use of Contingency Management were therefore included in this review.
There were a total of 75 hits for Health Coaching. As seen in Figure 1, following removal of duplicates and scanning of the papers on the basis of their title and abstract, 1 paper was identified for retrieval. This paper was not deemed to be eligible for inclusion in the review in view of the concomitant use of Varenicline in the intervention group which made it difficult to separate the effects of pharmacotherapy from that of the behavioral therapy, in this case, health coaching. No studies on the use of Health Coaching were therefore included in this review.
The studies on the 5As and brief advice, motivational interviewing and counseling which are included in this scoping review are described and summarized in Table 2.
Studies on the Use of Behavioral Therapies to Promote Smoking Cessation in People With Diabetes.

The 5As and Brief Advice and Smoking Cessation in DM
The 3 studies (Table 2) which examined the effectiveness of the 5As and brief advice in supporting smoking cessation in DM present conflicting results with the results of 1 study17 -19 reporting a higher odds of quitting smoking in persons in the intervention group whilst the other 2 studies20 -22 reported no significant result.
These inconsistent results are likely due to the differences between the interventions used in the studies. The study by Thankappan et al included delivery of 30-minute counseling sessions which included the 5As together with the 5 Rs, that is relevance, risks, rewards, roadblocks and repetition.17 -19 The intervention delivered in the study reported by Li et al and Lam et al was less intensive, with one 20-minute counseling session which had been adapted from the 5As and telephone follow-ups after 1 week and 1 month.21,22 The intervention by Albaroodi et al was the least intensive, consisting of a 5-minute session utilizing the 5As. 20
The difference in results may therefore be due to the length of the counseling sessions and the number and length of follow-up, where smokers are reminded to quit smoking.
Motivational Interviewing and Smoking Cessation in DM
Similar to the results of the studies on the use of the 5As and brief advice, the results for the studies on the effectiveness of motivational interviewing in persons with DM to assist with smoking cessation are inconsistent. Of the 4 studies which explored the effectiveness of motivational interviewing, only Perez-Tortosa et al reported a positive significant difference in smoking cessation with the motivational interviewing intervention.23 -26
Once more, whilst all the studies utilized motivational interviewing there were substantial differences in the way in which the latter was delivered in the different studies. The main outstanding difference in the study by Perez-Tortosa et al when compared to the other studies, was the use of an intensive intervention which was also adapted to the individual participant according to their level of change. 25 This meant that the number of sessions each participant received varied between 5 and 7 sessions. The participants’ level of change was assessed regularly; the intervention received, therefore, was dynamic and based on the person’s current needs.
Counseling and Smoking Cessation in DM
One study explored the effectiveness of counseling in assisting persons living with diabetes to quit smoking. 27 The intervention delivered included a 40-min nurse-led counseling session combined with education, and the negotiated setting of a smoking cessation date with the participants. Nicotine Replacement Therapy was also offered for a period of 3 months to under half (n = 105) of the intervention group (n = 208), although only 10 participants utilized the Nicotine Replacement therapy for the whole prescribed period. The results of this study showed a positive statistically significant difference in smoking cessation with the use of the counseling intervention; for those who did not stop smoking in the intervention group, there was a significant decrease in the number of cigarettes smoked.
Discussion
The Current Scope of Research on Behavioural Interventions to Assist Smoking Cessation
The present review has explored various psychological interventions for smoking cessation in individuals with diabetes, including the 5As and brief advice, Cognitive Behavioral Therapy, Motivational Interviewing, Contingency Management, Health Coaching and Counseling. The results of this review show that a number of psychological interventions, particularly Cognitive Behavioral Interventions, which have been shown to be effective in supporting smoking cessation in the general population and has been extensively researched in the management of chronic diseases, have as yet not been researched in relation to persons living with diabetes.28 -30 This gap in the literature creates an excellent opportunity for the development of knowledge in relation to smoking cessation in persons with diabetes.
The behavioral therapies which have been researched amongst smokers with diabetes are the 5 As, Motivational Interviewing and Counseling. The results of the studies for the first 2 are contradictory. For both the 5 As and motivational interviewing, a possible explanation may be that intensive interventions are required with multiple sessions of at least 30 min each being required. The results of Perez-Tortosa et al suggest that a dynamic intervention with the proactive adaptation of the intervention to the person’s level of change is helpful in assisting with smoking cessation. 25 These results mirror those in a systematic review which sought to identify the components of successful smoking cessation interventions in persons living with DM. 13 This reported that in general, irrespective of the smoking cessation intervention, an intervention including 3 to 4 sessions, lasting more than 20 min each, was more likely to be associated with smoking cessation success. 13
Directions for Future Research on the Use of Behavioural Therapies to Assist Persons With DM to Quit Smoking
The results of this and previous reviews provide the basis for a framework for the development of behavioral support interventions for persons with diabetes who smoke. The intensive interventions identified as being effective to date could serve to build structured behavioral therapy programs for persons with diabetes. Structured programs need to be evidence-based, and suit the needs of the person, must have specific aims and objectives, and support the person and their family members and carers in developing attitudes, beliefs, knowledge and skills. 31 The structured program must stipulate and provide in written form the content to be delivered to persons with diabetes, the mode of delivery, the number of sessions to be included, the use of aides, such as written, audio-visual or technological materials. 31 The persons delivering the intervention must have received accredited training and certification and the program must be quality assured and must be regularly reviewed by independent assessors who also check for consistency in the delivery of the program. 31 The outcomes of the program must also be audited regularly. 31
Structured educational programs have been consistently found to be effective in improving self-management and glucose stability in persons with diabetes, when compared to unstructured approaches where the delivery of the intervention is left to the discretion of the different health care providers.32 -35 In view of the latter, it is recommended that the development and evaluation of a structured behavioral program on the basis of the 5As and motivational interviewing, which include the components of the interventions delivered by Thankappan et al, Thankappan et al and Perez-Tortosa et al should be the focus of future research.17,19,25 Other behavioral therapies including counseling need to be further researched to identify the intervention components which are effective, before structured programs are developed and tested.
Nicotine is a highly addictive chemical which results in physical and psychological withdrawal symptoms when a person seeks to stop smoking, making smoking cessation very difficult. 36 In view of this, the use of nicotine replacement therapy or other drug treatments such as varenicline or bupropion are likely to be required to assist with smoking cessation in persons receiving behavioral therapy to improve the outcomes of the latter. The 2 studies included in this review, which utilized nicotine replacement therapy, do not provide an indication if this assumption could be true, since the research design of these studies does not allow an assessment of the specific contribution of the behavioral therapy and nicotine replacement therapy to the outcomes, individually or in combination with each other.24,27 Future studies should include 3 arm randomized controlled trials which would allow the exploration of the added benefits of combining behavioral therapies with nicotine replacement therapy or other smoking cessation medications.
Strengths and Limitations of the Scoping Review
This scoping review sought to be comprehensive in terms of the search, included 2 reviewers throughout and sought to present the results transparently to allow evaluation of the conclusions reached and allow replicability of the review.
In view of the complexity of the interventions reviewed, the comparison and identification of the active components of the interventions as well as those components which were not effective in encouraging smoking cessation in persons with diabetes was problematic and this is a limitation in arriving at conclusions.
Conclusion
This scoping review has highlighted the limited research available in relation to the use of behavioral therapy to assist with smoking cessation in persons with DM. This therefore is a research area which should attract the attention of researchers with an interest in diabetes care and smoking cessation, particularly in view of the increased risk of complications as a result of smoking experienced by persons living with diabetes. This research should focus on the development of a structured behavioral therapy program using the 5As and Motivational Interviewing as well as more basic research in relation to other behavioral therapies, such as Cognitive Behavioral therapy, in view of continued unclear outcomes of these therapies. Also required is the use of 3 arm randomized controlled trials to evaluate the possible added benefits of accompanying behavioral interventions with nicotine replacement therapy or other drugs used to assist with smoking cessation.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.