
Abstract
Introduction:
The Diabetes Prevention Program (DPP) is effective; enrollment is low. Little research has examined factors driving individuals’ enrollment decisions.
Methods:
In our final survey of a randomized trial comparing methods to increase enrollment in the DPP, we asked participants about factors impacting enrollment. We conducted interviews with a subgroup.
Results:
Participants who completed the survey (n = 299) were primarily female (96 male); middle-aged (mean 52.9, SD = 14.7); white (86%); non-Hispanic (85%). Only 19% reported awareness of the DPP prior to the study. Cost, online availability, and behavior-change motivation were the most highly rated factors influencing enrollment. The median amount participants were willing to pay for the program was $66.50. Phone interviews included 17 individuals who were/were not interested in receiving a referral to the DPP. Those interested described risk awareness, family history, social support, and healthcare-provider influence as facilitating enrollment. Cost, time, travel, unsupportive family, incomplete knowledge about the program’s impact and low self-efficacy were barriers. Among those uninterested, some were already engaging in lifestyle change, and some didn’t see a benefit.
Conclusions:
Results suggest that, even among high-risk individuals, efforts to increase awareness and benefits of the DPP are needed, as are efforts to address cost of enrollment and low motivation.
Trial Registration:
ClinicalTrials.gov protocol ID: 00132307. The Effect of 360 Video and MAPS on Enrollment in the DPP. URL: https://www.clinicaltrials.gov/study/NCT04746781?id=00132307&rank=1.
Keywords
Introduction
More than 97 million Americans have prediabetes, placing them at increased risk of developing Type 2 Diabetes (T2DM). 1 After finding that an evidence-based Intensive Lifestyle program could reduce the risk of T2DM by 58% among people with prediabetes or risk factors for T2DM,2,3 the Centers for Disease Control and Prevention established the National DPP Lifestyle Change Program (National DPP LCP). 4 However as of 2019, less than 1% of U.S. adults with prediabetes have enrolled in the program. 5 The year-long program consists of weekly meetings for the first 16 weeks, followed by monthly meetings over the course of the remaining 12 months. 6 It is facilitated by wellness coaches who teach participants principles of lifestyle change, including strategies for healthy eating and increased physical activity. 6 The program aims are to prevent or delay the development of T2DM, to promote participant engagement in at least 150 minutes of physical activity per week, and to achieve participant weight loss of 5% to 7% of total body weight. 6
Prior research describing the reasons people choose to enroll or not enroll in the National DPP LCP is limited to qualitative studies in select populations who have been referred to the DPP by their healthcare provider. For example, Ross et al, 7 investigated participants’ decisions about whether to enroll or not enroll in a digital version of the UK National Health Service Diabetes Prevention Programme. Among their sample of 32 adults diagnosed with prediabetes who had been referred, they found that a greater sense of self-efficacy regarding behavior change and a discussion with the referring healthcare provider about prediabetes and the nature of the program were positive influences in participants’ decisions to enroll in the program. In contrast, individuals who had made prior efforts at behavior change and felt that they had failed were less likely to enroll. Two additional studies explored National DPP LCP decisions among reproductive-aged females. First, among a sample of 29 adult females living in the U.S., who had initially enrolled in the DPP, knowledge that weight loss and physical activity could reduce or prevent the development of disease was a motivator for continued participation in the program (vs dropping out). 8 In another study with 23 reproductive-aged females living in the U.S., motivation to enroll in a program was related to concern about family history of T2DM and a desire to improve their and their families’ health, while barriers to enrollment included the presence of other health conditions (eg, requiring supplemental oxygen). 9 The only study that has surveyed a larger sample of program participants was conducted by Shawley-Brzooska et al, 10 who surveyed 89 participants living in the U.S. who had completed a free year-long program for individuals with dysglycemia (62% of whom were diagnosed with diabetes). They noted barriers to program adherence (eg, scheduling conflicts and difficulty with transportation). Understanding the context and nuance of decision-making related to National DPP LCP enrollment is essential. Knowledge of these factors is needed to develop effective messaging to promote the program. It’s also a vital component of effective healthcare-provider communication aimed at addressing barriers to program enrollment and engagement.
The aim of this study was to build on this prior work by surveying a larger sample of individuals with prediabetes and describing the relative importance of factors related to the decision to enroll (which may be different than the decision to stay engaged), or not, in the National DPP LCP, and to specifically investigate factors that might impact enrollment that have not previously been quantified (ie, individuals’ awareness of the DPP and their willingness to pay out of pocket for their program). We also sought to determine if there were factors not included in the survey by conducting follow-up phone interviews with a random subset of participants.
Methods
Data for this study come from the final survey in a randomized trial comparing methods to increase enrollment in the National DPP LCP and qualitative interviews with a subset of participants. The protocol for the randomized trial has been published previously. 11 The planned sample size calculated for the randomized trial was 400.
Settings and Recruitment
Study participants were recruited from 2 sites: University of Utah Health and the Midvale Community Building Community Clinic (CBC). University of Utah Health is the Mountain West’s only academic healthcare system and includes 5 hospitals, 12 community clinics, and several specialty centers. The Midvale CBC is an outpatient community health clinic providing medical, dental, and physical therapy, and mental-health services to low-income and uninsured families, with a predominantly Spanish-speaking clientele.
We identified potential participants using each health system’s electronic health record. We then sent the pool of potential participants an email, allowing them to opt out of any further study-related communication. The email included a brief description of the study, and an explanation that they would be contacted on their mobile phone 2 weeks later if they did not opt out. Potential participants who had a bounced email were sent a single letter with the same information. All subsequent questionnaires were sent via links through SMS text
Participants
Inclusion criteria
Both Spanish-speaking and English-speaking patients ages 18 and older from University of Utah Health and the Midvale CBC who reside in Utah were invited to participate in the study. Patients were eligible for the trial if: (1) they were aged 18 to 89 years; (2) had a diagnosis of prediabetes within the past 5 years documented in the electronic health record (ICD-10 code R73.03); and (3) had an email address and mobile telephone number on record with the health system.
Exclusion criteria
Patients were excluded from the study if they had any of the following diagnoses: Type 2 diabetes mellitus (ICD-10-CM E11); Type 1 diabetes mellitus (ICD-10-CM Diagnosis E10), diabetes mellitus due to underlying condition (ICD-10 E08); drug or chemical induced diabetes mellitus (ICD-10 E09); gestational diabetes (ICD-10 024.4); neonatal diabetes mellitus (ICD-10 P70.2); or post-pancreatectomy diabetes mellitus (ICD-10 E13).
In addition, individuals who were currently pregnant and those who had already participated in the National DPP LCP were excluded from the trial, as they are ineligible for program enrollment. These criteria were determined by screening questions at the start of the baseline survey.
Study Design and Data Collection
To obtain complementary qualitative and quantitative data that could be compared, we used a convergent mixed-methods design. 12 The convergent mixed-methods design is a parallel design, in which qualitative data are collected and analyzed separately and later merged in order to connect and interpret the combined results. 12 We selected this design to combine the individual strengths of quantitative and qualitative analysis in order to gain nuance and rich contextualization of the topic through triangulation of the data. The results of our mixed-methods data integration are presented in the discussion section.
The quantitative data for our convergent design came from self-administered Qualtrics surveys, while our qualitative data were collected during one-on-one, semi-structured interviews conducted by phone. Quantitative data used in this study come from both the baseline and final surveys of our randomized trial. In the baseline survey we collected demographic information. These included questions about sex, age, race/ethnicity, height, weight, annual income, and health insurance status.
At 6 weeks following randomization, survey questions prompted information about (1) the participant’s prior awareness of the National DPP LCP, (2) the relative importance of factors in choosing whether to enroll in the program or not, and (3) the maximum amount they would be willing to pay for the program. Survey links were sent to participants by SMS text messages, with up to 2 reminders to complete each survey. Participants were asked about their current interest in the National DPP LCP on a scale from 1 to 5, with 1 being very interested and 5 being not interested at all. Several enrollment factors were assessed on a scale of 1 to 5, with 1 being extremely important and 5 being not important at all. Participants were asked, “What is the maximum amount you would be willing to pay for the DPP (if the cost were $1 more, you would be unwilling to pay).” Responses were on a sliding scale from $0.00 to $750.00. Participants received $20.00 incentive payments for completion of the baseline and follow-up survey.
For the qualitative strand of the study, we randomly selected willing participants for phone interviews. A semi-structured interview guide was developed by the study’s primary investigators. The questions were designed to elicit responses about participants’ awareness of their status as a person with prediabetes, awareness of and contact with the National DPP LCP, and barriers to and facilitators of National DPP LCP participation. Interviews were conducted by the study’s 2 primary investigators via telephone at times selected by each participant. Transcripts from audio recordings of the in-depth interviews were created for the purpose of qualitative analysis.
Analysis
We calculated simple descriptive statistics to quantify participant demographics and survey responses. In the survey, participants rated their interest in the National DPP LCP on a scale from 1 to 5 with 1 representing “I am very interested” and 5 representing “I am definitely not interested.” Participants also rated factors regarding their importance in relation to the decision to enroll in the DPP or not (such as cost) on a scale from 1 to 5 with 1 being “extremely important” and 5 being “not important at all.” Prior to analysis, we reverse-coded these responses so that higher ratings expressed more interest in the program and we excluded individuals who did not respond to the question.
Audio recordings of the phone interviews were transcribed by study research assistants and were reviewed for accuracy by an additional research assistant. Transcripts were uploaded to the Dedoose qualitative coding software version 9.0.107. 13 The goal of the qualitative analysis was to stay close to the data in order to capture a low-inference summary of participants’ experiences and to reflect the language used by participants. To support this goal, we used a qualitative descriptive approach using content analysis and thematic analysis. 14 Deductive codes were used to index barriers and facilitators to program enrollment, as well as participants’ prediabetes awareness. The transcripts were reviewed for novel insights provided by the participants, and additional inductive codes were created to capture these. Discrepancies in coding were reviewed by all authors during coding meetings and were resolved by group consensus. All authors were involved in the coding process and in the development of the study’s qualitative themes. The themes were organized by comparing across the coding categories and across participant intention to engage in the program.
After analyzing the quantitative and qualitative data separately, we compared these discrete datasets through group discussion and memos. After deliberation, we integrated the quantitative and qualitative data through the narrative report of the discussion section to detail how these data converged or diverged and to provide a well-rounded description of the enrollment decision-making of people with prediabetes.
Ethical Considerations
The study was approved by the University of Utah’s Institutional Review Board (IRB; IRB_00163014).
Results
Characteristics of the Participants
The study’s sample was primarily white (n = 257) and non-Hispanic (n = 255). More than two-thirds of the 299 participants were female (n = 203), and the average age of participants was 52.9 (SD = 14.7). Please see Table 1 for details about participant demographics.
Demographics of People Completing Follow Up Survey.

Quantitative Results
Of the 299 participants who completed the follow-up survey and were therefore included in this analysis, 81 (27.1%) requested a referral to the National DPP LCP and 7 enrolled in the program. Awareness of the program prior to the study was limited among this sample; just 57 participants (19%) reported awareness of the program prior to study enrollment. Participants’ rating of their interest in the National DPP LCP on a scale from 1 to 5 (with 1 representing “I am definitely not interested” and 5 representing “I am very interested”) resulted in a mean of 3.45 (SD = 1.1) amongst the 242 participants who provided a rating. For the rating of the importance of factors in relation to the decision to enroll in the DPP or not, cost of the program was the most important (mean score = 4.99, SD = 1.2, n = 295), followed by availability of classes via the internet (mean score = 4.85, SD = 1.2, n = 295), motivation to change health behaviors (mean score = 4.8, SD = 1.0, n = 295), length of the classes (mean score = 4.5, SD = 1.2, n = 295), travel distance to classes (mean score = 4.4, SD = 1.3, n = 295), language in which the classes were offered (mean score = 3.9, SD = 1.6, n = 294), and—the least often cited as most important—the factor of availability of childcare (mean score = 2.7, SD = 1.4, n = 294). Last, the median result for the maximum dollar amount participants were willing to pay for the program was $66.50, and ranged from $0 to $700 (n = 264).
Because cost was cited as the most important factor in the enrollment decision, we did a post-hoc analysis to compare income between individuals who enrolled in the DPP versus those who did not. We found that the mean income amongst enrollees was $84 498 and was $79 852 among non-enrollees. Since the number of enrollees was small compared to non-enrollees, we used a Wilcoxon rank-sum test to compare these, and the difference was not significant (W = 949.5, P = .99).
Qualitative Results
Of the 17 participants who completed a qualitative interview, most were non-Hispanic (94%, n = 16), white (88%, n = 15), and female (59%, n = 10), with a mean age of 48 (range = 20-78). More than half (59%, n = 10) expressed interest in enrollment in the National DPP LCP although none had formally enrolled at the time of the interview.
During the qualitative interviews, participants described their decision-making about program enrollment. Based on these qualitative responses, this allowed the qualitative-coding team to organize responses according to participant program interest and then to identify subthemes under the 2 broader themes of (1) Interested in the National DPP LCP, and (2) Not interested in the National DPP LCP. Subthemes under the first theme included (1) Barriers among those who desire program participation and (2) Facilitators among those who desire program participation. Subthemes under the second theme included (1) Already engaging in lifestyle change and (2) Do not see a need to participate in the program.
Theme 1: Interested in the National DPP LCP: Barriers among those who desire program participation
Among participants who expressed interest during their interview in National DPP LCP participation, 6 barriers to participation were identified. The first barrier was the cost of the program. Participants described issues with insurance that prevented them from participating (eg, an insurance stipulation for in-person program attendance which conflicted with a work schedule). The program’s total cost was considered high and was also discussed as a barrier. The second barrier was the time commitment for program participation. Participants found the prospect of consistently carving out time for class difficult when considering other responsibilities. The third barrier was travel to classes. Traveling to an in-person class was considered burdensome and costly. The fourth barrier—unsupportive network member(s)—related to the day-to-day changes that would require support from participants’ social networks in order to make successful lifestyle change (eg, family support for dietary changes). The fifth barrier—incomplete information—underscored a lack of knowledge among participants about what the program could do for them. Since some people had already made lifestyle changes, they were unsure whether the program could help with additional risk reduction. Finally, the sixth barrier was low self-efficacy. Participants described being unsure about whether they would be able to apply program principles within their day-to-day life. See Table 2 for quotes about barriers among participants who desired to participate in the program.
Barriers Among Those Who Desire Program Participation.

Theme 1: Interested in the National DPP LCP: Facilitators among those who desire program participation
Among participants who expressed interest in program enrollment during their interview, 4 facilitators to National DPP LCP participation were identified. The first was risk awareness. Participants who were aware of their risk for developing diabetes were often motivated by this risk awareness in order to prevent T2DM and improve their health. Participants talked about motivation to gain additional knowledge from the program to support long-term health. The second facilitator to program participation was having a family history of diabetes. First-hand experience with family members’ diabetes illness trajectories compelled participants to want to take proactive steps to avoid developing diabetes. Participants cited family members’ experiences with diabetes as motivators to avoid diabetes if possible. A third facilitator was social support provided by social-network members, such as family, friends, and their partners. For example, participants said their partners were reassured by their interest in program participation because they were pleased the participants would gain information and skills to reduce their risk of developing diabetes. The fourth facilitator was provider influence. When healthcare providers made clear the risk and consequences of becoming diabetic, participants were motivated to improve their health (eg, motivation to improve the HbA1c laboratory). See Table 3 for additional quotes about facilitators to program participation.
Facilitators Among Those Who Desire Program Participation.

Theme 2: Not interested in the National DPP LCP: Already engaging in lifestyle change
Among participants who expressed during their interview that they were not interested in participating in the National DPP LCP, 3 factors were identified under the subtheme of Already engaging in lifestyle change. The first factor was that participants felt they had already successfully made lifestyle changes on their own. These participants believed they had a foundation of knowledge and access to information, and that they were already taking proactive steps to avoid developing diabetes. The second factor among those who were uninterested in the program was the fact that some had already enrolled in another program (eg, WeightWatchers®). Last, the third factor was weight loss among participants who were uninterested in program enrollment. These participants believed they had lowered their risk of developing diabetes through weight loss, and, therefore, did not need the National DPP LCP. See Table 4 for additional quotes relating to these factors.
The Factors Among Those Who Do Not Desire DPP Participation.

Theme 2: Not interested in the National DPP LCP: Do not see a need to participate in the program
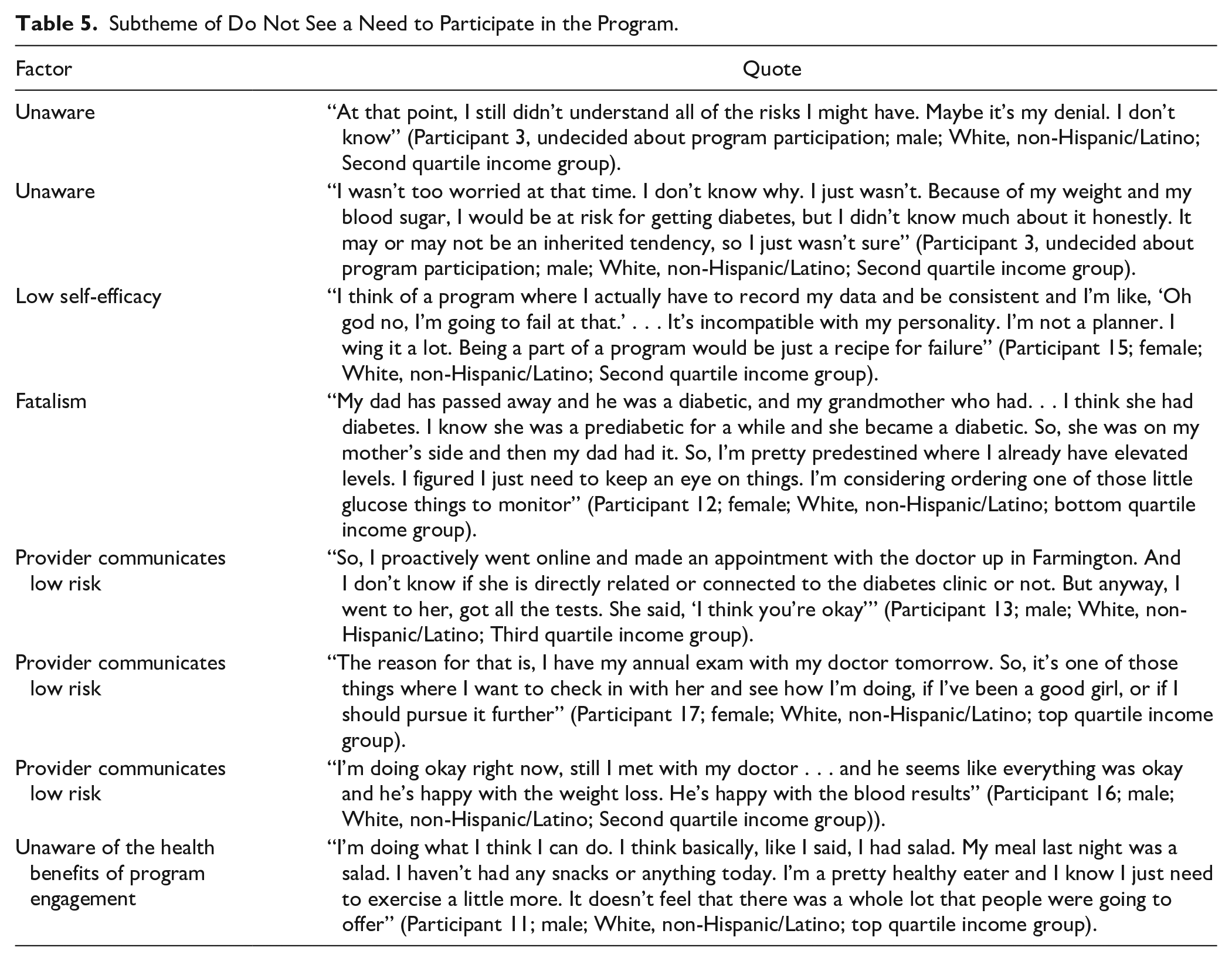
Among participants who expressed during their interview that they were not interested in participating in the National DPP LCP, 5 factors were identified under the subtheme of Do not see a need to participate in the program. The first factor was participants’ unawareness of risk. Some participants talked about not understanding the implications of their health indicators (eg, BMI, HbA1c) in relation to their risk for developing diabetes. In contrast, the second factor of participants’ fatalism illustrated the belief that some participants felt they were “predestined” to develop diabetes, or that they would fail at an attempt to engage in the program (ie, low self-efficacy). The third factor was provider influence, where participants believed that their healthcare providers had communicated that they were at low risk for developing diabetes, and that providers were happy with the results of participants’ lifestyle change (eg, weight loss, laboratory results). Last, the fifth factor was a lack of understanding among some participants of how the program might help them (eg, social support for behavior change, or reversal of a prediabetes diagnosis). See Table 5 for additional quotes related to the subtheme Do not see a need to participate in the Program.
Subtheme of Do Not See a Need to Participate in the Program.
Discussion and Conclusions
In this project we conducted mixed-methods analysis of factors that drive individuals’ National DPP LCP enrollment decisions. We found that, even among individuals with an ICD-10 code for prediabetes who were reminded during the study that they had been diagnosed with prediabetes, most were unaware of the existence of the National DPP LCP. In regard to factors driving enrollment, we found that cost, individuals’ motivation for behavior change, and the availability of the program via the internet were the most highly-rated factors impacting program enrollment decisions.
In relation to cost, we found that the median amount participants were willing to pay for the program was $66.50, considerably less than the $500 out-of-pocket cost they would incur if their insurance did not cover the program. Prior literature repeatedly confirms that cost is a major barrier to National DPP LCP participation,15 -17 indicating a need to implement strategies that overcome this barrier. Some recommendations that have been considered are offering incentives, such as gym memberships, 8 or providing scholarships to offset the cost. 16 In our study, we found online availability of the program, cost, time, and travel are closely related factors in decisions regarding program enrollment; and that competing responsibilities impede a person’s ability to attend on a consistent basis. These factors are consistent with the limited research investigating enrollment decisions. 10 Additionally, the in-person program may require significant travel, which can add to the cost, thus emphasizing the need for increased availability of an online program. For individuals who feel that lack of time due to responsibilities is a barrier, offering a self-paced virtual version of the program may also be a future consideration.
We found that some individual-level factors relating to motivation for behavior change affected interest in program enrollment. First, for example, awareness of risk related to family history impacted some participants’ motivation to enroll. Conversely, other participants believed their family history would cause development of diabetes regardless of intervention. These somewhat contradictory findings underscore the need to understand individuals’ barriers to and motivators of enrollment so that these can be directly targeted through tailored health-messaging campaigns. Second, many participants emphasized weight loss as a goal of the program. However, the National DPP LCP emphasizes other important components, such as healthy eating and coping skills, 3 which were less emphasized by participants in this study. Third, our study provides evidence that the National DPP LCP presently is not effectively communicating why participation in the DPP is optimal, as opposed to self-directed health-behavior change or participation in another program. More explicit messaging about the specific benefits of what the DPP has to offer (eg, greater reduction in the risk of developing T2DM, peer support, focus on maintenance of healthy behaviors long term) may act as a motivator to program enrollment and engagement.
Consistent with literature, social and provider support seem to be both facilitators of and barriers to program participation.8,15,17,18 Lack of family support created a barrier to enrollment even among participants interested in the program. Common themes were lack of family members’ understanding of the appropriate behavioral modifications participants needed to implement for a healthier lifestyle. For example, some participants felt the need to prepare separate meals for themselves and their families, which could also add to the barrier of cost. Certain solutions have been proposed to address this barrier, such as encouraging familial participation in the program to increase awareness of diabetes and its complications while also reinforcing health behaviors as a family.17,18 Provider influence in program participation illustrates the power of the patient-provider relationship. Trust in the patient-provider relationship in conjunction with better provider education about the National DPP LCP could possibly facilitate program enrollment. 11
Limitations
While we intended to recruit a diverse sample, our participants were primarily white and non-Hispanic. Most were insured and over two-thirds of participants identified as female. Thus, findings may not apply to minoritized populations or those without health insurance. Additional approaches for recruiting minoritized and Spanish-speaking participants should be considered in future studies.
Follow-up survey participants were a subset of the larger RCT participants and may not be representative of the prediabetic population. It is possible that the reason for enrolling or not enrolling might differ between the individuals who participated in our follow-up survey and interview versus those who did not.
Strengths and Mixed-Methods Integration
The combination of qualitative and quantitative data provides rich information about barriers and facilitators to program participation. The quantitative data revealed participants’ willingness to pay, interest in the program, and reasons for not enrolling. The qualitative data added context and richness to the quantitative data, providing a more complete understanding of our research question and giving us additional information about participant willingness to pay for participation—information that helped us to understand qualitative responses about cost barriers. The qualitative data gave us more nuanced information about participants’ reasons for not enrolling (eg, making their own lifestyle changes, fatalism, and family history). Our findings were consistent with the ADA’s recent recommendation for a 3-month program, as offering a shorter National DPP LCP option would likely be attractive to some of our participants. In our quantitative data, we found a failure to enroll in the program by participants, even those who expressed interest in the program. Notably, we found that people did make lifestyle changes after risk notification but were simply not prepared to join a 12-month program. The mixed-methods analysis revealed a more nuanced picture revealing that some participants who did not enroll in the program reported making lifestyle changes on their own.
In sum, our study results highlight the need for efforts to increase public awareness of the National DPP LCP as a means to help people make sustainable changes to their lifestyle and reduce their risk for T2DM. Our results also suggest that targeted health-messaging campaigns to address specific barriers to enrollment and provide information about the broader benefits of the program are needed. Possible targets include the cost of the program; the belief that the program is unnecessary, and its implied corollary that most individuals can make and maintain lifestyle changes on their own without support; and fatalism amongst individuals with a strong family history of T2DM who may believe that they will develop T2DM regardless of their behaviors.
Footnotes
Acknowledgements
We would like to thank Marta and Nancy Valadez, who were the study’s Motivation and Problem Solving Coaches. We thank the administrators and staff of the Diabetes Prevention Program at the University of Utah and the Midvale Community Building Community Clinic for their participation on this project. Last, we are grateful to the study’s project advisors at the CDC.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the Centers for Disease Control and Prevention [Contract#: 75D30120C09181]. Research reported in this publication was also supported by the National Institute of Nursing Research of the National Institutes of Health [Award Number F31NR020431]. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Consent to Participate
Prior to study engagement, people who were eligible for the study reviewed an online consent cover letter before completing a baseline survey and being randomized.
Consent for Publication
Not applicable.
Ethical Considerations
The study was approved by the University of Utah’s Institutional Review Board (IRB; IRB_00163014).
Data Availability
Data may be made available through contact with the corresponding author.