
Abstract
Introduction:
Rural cancer survivors often face greater barriers to treatment, which may translate into worse satisfaction with health care.
Objective:
To examine rural versus urban differences in satisfaction with health care among Medicare cancer survivors.
Methods:
Data are from the 2020 Medicare Current Beneficiary Survey (MCBS). Rao-Scott chi-square analyses were conducted to examine rural versus urban inequities in satisfaction with 9 dimensions of health care (health professionals’ concern for health, information about what was wrong, ease/convenience from home, ease of obtaining answers over telephone, getting needs taken care of at same location, availability of specialists, overall quality, and out-of-pocket costs, and availability of care at night/on weekends). Multiple logistic regression analyses were conducted to test for rural/urban differences while adjusting for race/ethnicity, gender, marital status, educational attainment, health insurance (traditional Medicare, Medicare Advantage, dual Medicaid coverage, employer, or self-purchased insurance), and self-rated overall health.
Results:
Rural cancer survivors were less satisfied with the ease/convenience of getting to health professionals (93.35% rural and 96.87% urban) and less satisfied with getting all health care needs taken care of at the same location (88.32% rural and 92.22% urban). These rural/urban differences persisted when adjusting for other factors.
Conclusions:
Health care providers serving rural areas may need to consider new strategies to satisfy some of the unique needs of rural cancer survivors, such as better organizing services at single clinic sites and utilizing telehealth when feasible to reduce the need to travel for in-person services.
Introduction
Cancer survivors need routine health care in the time periods immediately following their diagnosis and extending into the survivorship period.1,2 Maximizing satisfaction with care is relevant to clinical practice as it has been shown to be associated with future health care utilization and health status. 3 One study found that higher satisfaction with care was associated with higher spending on health services, which reflects health care utilization, as well as better self-rated health in the following year among cancer survivors ages 65 years and older. 3 A separate study found that better ratings of personal and specialty clinicians were positively related to receiving surveillance follow-up visits among colorectal cancer survivors. 4
Rural cancer patients face greater barriers to treatment access than urban patients,5 -8 which could persist during survivorship care. Patient satisfaction ratings can be informative for identifying rural/urban inequities in cancer survivors’ health care needs that could be ameliorated through changes in the organization and delivery of services. One prior study based on data from the 2016 Medicare Beneficiary Survey (MCBS) found that rural residents overall, regardless of their cancer history, had lower unadjusted satisfaction rates for 8 of 9 aspects of health care than urban residents. 9 When adjusting for other factors, rural residents had lower satisfaction with the ease or convenience of getting to health professionals from their home and the availability of specialty care when needed. 9 A second study based on 2012 MCBS data found that rural residents had lower satisfaction with insurance for prescription drug coverage than urban residents. 10 Research to date has not examined rural/urban inequities in satisfaction with care among Medicare beneficiaries with a history of cancer, but a handful of studies have examined rural/urban differences in consumer assessments of care based on based on Surveillance, Epidemiology, and End Results Program (SEER) data merged with the Consumer Assessment of Healthcare Providers and Systems (CAHPS®) patient survey, which Medicare regularly administers to beneficiaries.11,12 The CAHPS® includes experiences with care questions that are used to create composite scores reflecting how often services were received or performed, whereas health care ratings and other satisfaction measures assess a more subjective dimension of the degree to which the services meet expectations. 13 One study based on SEER-CAHPS surveys found that rural cancer survivors reported better care coordination composite scores relative to urban survivors. 14 A second study based on SEER-CAHPS surveys revealed no significant rural/urban differences in getting needed care and getting care quickly composite scores among cancer survivors. 15
Although prior research indicates that rural cancer survivors do not have worse assessments of their care than urban survivors, there is reason to suspect that they may have worse satisfaction with care, which could contribute to less follow-up care utilization. As described earlier, analyses of the overall MCBS sample found that rural residents were less satisfied with numerous dimensions of health care than urban residents, 9 and satisfaction has been linked to cancer survivors’ health care utilization.3,4 The main objective of this study was to examine potential rural versus urban inequities in satisfaction with health care among a national sample of Medicare beneficiaries ages 65 years and older with a prior cancer (non-skin) diagnosis. The study tested the hypothesis that rural cancer survivors have lower satisfaction with care than urban cancer survivors. A secondary objective was to examine how other predisposing, enabling, and need factors are associated with satisfaction with care.
Methods
Conceptual Model
The Behavioral Model of Health Services was applied to guide the inclusion of variables that could be associated with satisfaction with care. 16 The original model posited that predisposing (eg, demographic), enabling (eg, health insurance coverage), and need (eg, health status) factors influenced health care utilization. 16 A later model posited that those same factors influence outcomes of health care utilization, such as satisfaction. 16
Data
The data source is the 2020 Medicare Current Beneficiary Survey (MCBS), the most recent publicly available MCBS dataset. 17 The MCBS represents a national sample of persons enrolled in Medicare, who are eligible because of age (65 years or older), end stage renal disease, or disabilities. For this study, analyses focused on persons ages 65 years or older, who self-reported a history of cancer other than skin cancer, and who were enrolled in Medicare at any point in 2020. The unweighted sample size was 2438 and the weighted sample size was 9 938 437.
Dependent Variables
The MCBS includes 9 single items assessing satisfaction on a 4-point scale from very satisfied to very dissatisfied. Survey respondents did not rate a particular dimension of care if they had no experience with it. These items assessed:
Health professionals’ concern for overall health
Information given to you about what was wrong with you
Ease, convenience of getting to health professionals from where you live
Ease of obtaining answers about treatment, prescriptions over telephone
Getting all health care needs taken care of at same location
Availability of care by specialists when needed
Overall quality of care in last year
Out-of-pocket costs
Availability of health care at night or on weekends
Because the responses were skewed toward being satisfied, a binary variable representing very satisfied/satisfied and very dissatisfied/dissatisfied was created. Prior work making use of satisfaction variables in the MCBS and other national datasets, such as the Medical Expenditure Panel Survey (MEPS), have also similarly created a binary satisfied/dissatisfied variable. 9
Independent Variables
The main predisposing variable of interest was rural versus urban residence. The MCBS categorized residence as non-metropolitan (rural) or metropolitan (urban) according to whether the respondent resided outside or within a core-based statistical area with an urban core of at least 50 000 persons. Predisposing variables included race/ethnicity and gender. The MCBS categorized race/ethnicity as non-Hispanic White, non-Hispanic Black, Hispanic, and other race/ethnicity, with the other category comprising “other single races not of Hispanic origin, Two or More Races, or Unknown Races” (p. 20) and gender as male or female. 17 Enabling variables were educational status (less than a high school degree, a high school or vocational/technical/business degree, or more than a high school degree) and health insurance. Health insurance variables were not mutually exclusive and included traditional Fee-for-Service (FFS) Medicare or Medicare Advantage coverage, Medicaid dual eligibility for at least part of the year (yes/no), private employer sponsored health insurance (yes/no), and private self-purchased health insurance (yes/no). Need was assessed with a single-item rating of one’s self-rated general health compared to someone of the same age and categorized as excellent, very good, good, or fair.
Analysis
Sample characteristics and dependent variables were compared across rural/urban residence, with the Rao-Scott chi-square test to detect any statistically significant differences. Multivariate logistic regression analyses were conducted to determine if rural/urban differences persisted while adjusting for other factors. SAS (SAS Institute Inc., Cary, NC) survey procedures incorporating full sample and replicate weights were used to account for the complex sampling scheme. 18
Results
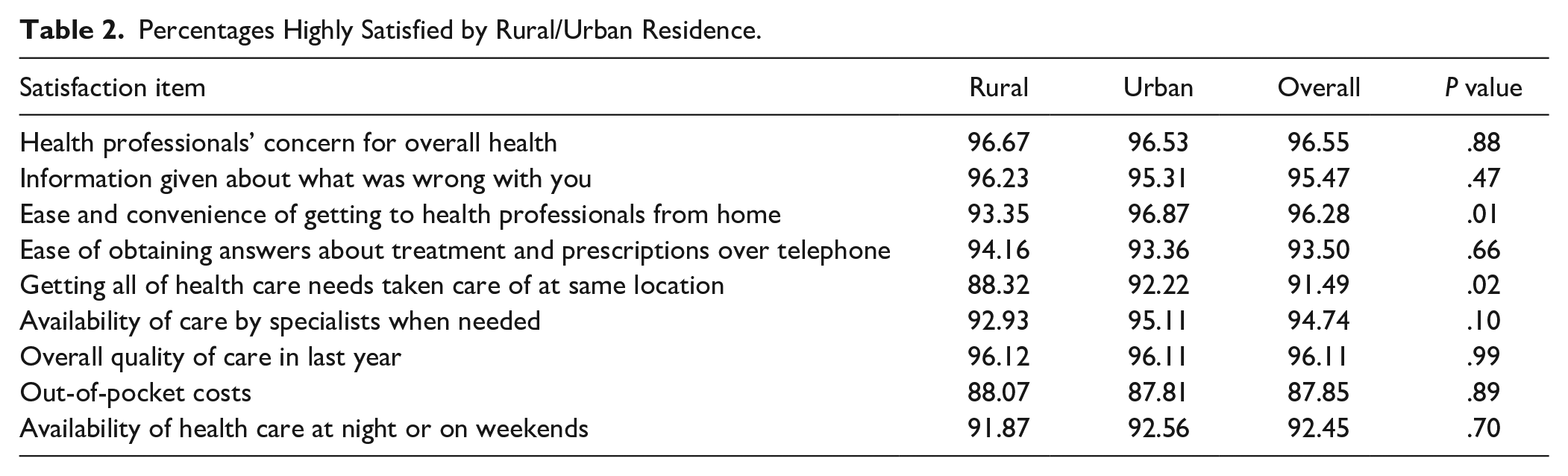
Table 1 illustrates that higher proportions of the rural sample were non-Hispanic White, had Medicare FFS coverage, and had less than a high school education or a high school or technical degree. As shown in Table 2, rural cancer survivors were less satisfied with the ease/convenience of getting to health professionals (93.35% rural and 96.87% urban) and less satisfied with getting all health care needs taken care of at the same location (88.32% rural and 92.22% urban). For the sake of brevity, multivariate results are only reported for the prior 2 satisfaction factors, as significant rural/urban differences were not found for the remaining satisfaction factors in either the bivariate or multivariate analyses. When adjusting for other factors, the rural/urban differences in these satisfaction factors persisted, as shown in Table 3. Rural residents had lower odds of satisfaction with the ease/convenience of getting to health professionals from their home (OR = 0.525; 95% CI 0.276, 0.996) and lower odds of satisfaction with getting all of their health care needs at the same location (OR = 0.654; 95% CI 0.441, 0.971). Males had higher odds of satisfaction with getting all of their health care needs taken care of at the same location (OR 1.982; 95% CI 1.402, 2.803). Very good (OR = 7.655; 95% CI 2.533, 23.140) and good (OR = 2.839, 95% CI 1.166, 6.909) self-rated overall health were associated with higher odds of satisfaction with the ease/convenience of getting to health professionals from home; and very good self-rated health was associated with higher odds of satisfaction with getting all health care needs taken care of at the same location (OR = 2.784; 95% CI 1.16, 6.76).
Sample Characteristics by Rural/Urban Residence.

P-values correspond to Chi-Square tests of rural/urban differences across variables (eg, to test for rural/urban differences in race/ethnicity).
Percentages Highly Satisfied by Rural/Urban Residence.
Adjusted Odds of Ease and Convenience of Getting to Heath Professionals from Home.
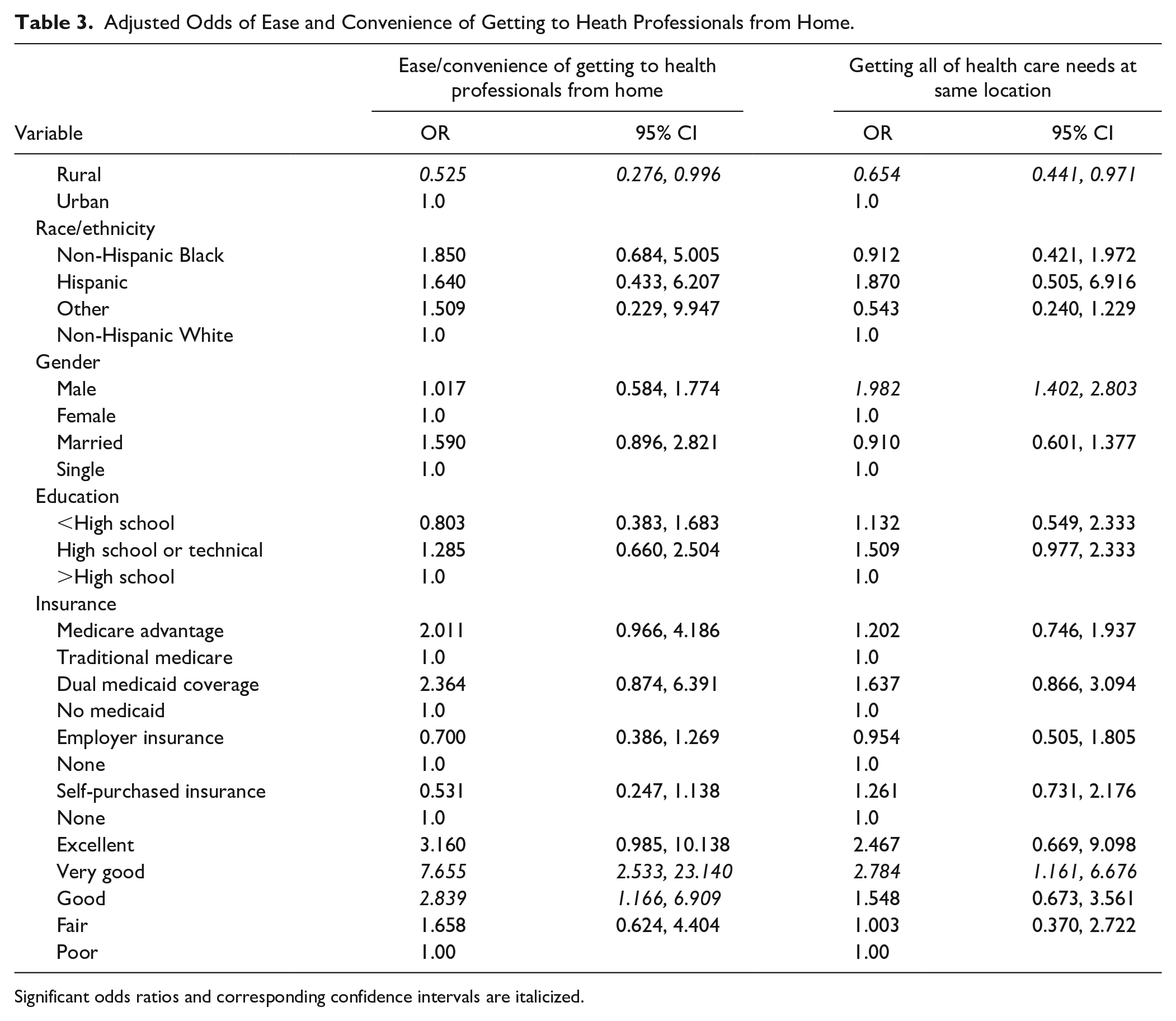
Significant odds ratios and corresponding confidence intervals are italicized.
Discussion
This study provides information about rural/urban inequities in satisfaction with health care among Medicare beneficiaries surviving cancer. The hypothesis that rural cancer survivors are less satisfied than urban cancer survivors was confirmed for measures pertaining to the convenience and centralization of services. Overall, these results are more positive than those from a study based on 2016 MCBS data, which found that rural residents with and without cancer had lower satisfaction with each of 9 aspects of health care examined in that study. 9
Lower satisfaction with the convenience and centralization of services could have consequential effects on cancer survivors’ follow-up care access. Prior research has shown that colorectal cancer survivors who have better personal and specialty doctor ratings are more likely to have follow-up visits for cancer surveillance. 4 Telehealth is one potential mechanism to improve the convenience of health care services and facilitate access to services that are frequently offered across multiple sites. Telehealth use expanded substantially during the COVID-19 pandemic among the nation at large, 19 and a review of the extant literature on cancer survivors’ use of telehealth concluded that they generally have high levels of satisfaction with telehealth. 20 Other research suggests that telehealth could serve as a means of improving the convenience and coordination of health services among rural residents. Even prior to the pandemic, rates of telehealth utilization among rural Medicare beneficiaries were increasing. 21 Moreover, family physicians practicing in rural areas reported at higher rates than those practicing in urban areas that telehealth was beneficial for assuring accessible and continuous care as well as facilitating patients’ access to specialists. 22
A secondary objective of this study was to determine how other key predisposing, enabling, and need factors were associated with satisfaction. Of the remaining predisposing characteristics, female gender was negatively associated with satisfaction with the centralization of services. A recent report summarized inadequacies in primary care for women, including not having a usual source and poor coordination, which could translate into lower satisfaction with the centralization of services at a single site. 23 Conversely, other research revealed that older women are more satisfied with their health care overall 24 and their personal doctors than are men. 25 Going forward, more research is needed to further elucidate gender differences and inform clinicians and health care managers about how to organize and deliver services to improve satisfaction.
Self-rated overall health, which reflects need for health care, was associated positively with satisfaction with the convenience and centralization of services. Similarly, a survey of approximately 5000 persons ages 65 years and older in Texas found that those with better overall health ratings were more likely to be highly satisfied with their health care overall. 24 The cross-sectional nature of the former study does not allow one to interpret if satisfaction leads to better health or vice versa. However, research based on the nationally representative Medical Expenditure Panel Survey found that high levels of satisfaction with care were longitudinally predictive of better self-rated health. 3 On the other hand, health status may instead predict satisfaction, as a study conducted among persons with prostate cancer found that health status predicted satisfaction with care over the year following treatment. 26
Limitations
This paper’s findings should be considered within the context of several methodological limitations pertaining to the cross-sectional study design and lack of specificity in several key measures. Because the study design is cross-sectional, the findings represent associations at a single point in time. A major limitation of the satisfaction measures is that they are not specific to cancer-related services. Moreover, the MCBS does not ask any information about the time since the cancer occurrence or treatment, primary care site, or cancer-related comorbid conditions.
Conclusions and Implications
Health care providers serving rural areas may need to consider new strategies to satisfy some of the unique needs of rural cancer survivors, such as centralizing services at single clinic sites or utilizing telehealth when feasible to reduce the need to travel for in-person services. Further research should investigate whether rural survivors’ lower satisfaction with 2 dimensions of health care accessibility, the ease/convenience of getting to care and getting care at the same location, inhibits their use of cancer survivorship follow-up services.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by the Federal Office of Rural Health Policy (FORHP), Health Resources and Services Administration (HRSA), U.S. Department of Health and Human Services (HHS) under cooperative agreement # U1CRH30041. The information, conclusions and opinions expressed in this document are those of the authors and no endorsement by FORHP, HRSA, HHS, or the University of Kentucky is intended or should be inferred.