
Abstract
Introduction:
Colonoscopy is a critical component of colorectal cancer (CRC) screening and patient navigation (PN) improves colonoscopy completion. A lay navigator remotely providing navigation across rural primary care organizations (PCOs) could increase PN access. In preparation for the Colonoscopy Outreach for Rural Communities (CORC) study, we examined partners’ perspectives on contextual factors that could influence CORC program implementation, and adaptations to mitigate potential barriers.
Methods:
We interviewed 29 individuals from 6 partner PCOs and the community-based organization (CBO) delivering the PN program. An analysis approach informed by Miles, Huberman, and Saldana identified critical themes. Results are reported using the Framework for Reporting Adaptations and Modifications-Enhanced (FRAME).
Results:
Potential barriers included that rural patients are hard to reach remotely and might mistrust the navigator, and the CBO is unfamiliar with the patient communities and does not have patient care experience or pre-existing communication pathways with the PCOs. Program content and navigator training was adapted to mitigate these challenges.
Conclusions:
Our study highlights contextual factors to account for before implementing a remote, centralized patient navigation program serving rural communities. Gathering partner perspectives led to intervention adaptations intended to address potential barriers while leaving the core components of the evidence-based intervention intact.
Introduction
Colorectal cancer (CRC) is the second leading cause of cancer death in the U.S. 1 Rural counties experience CRC disparities; they have a higher incidence of CRC, late-stage diagnosis, and CRC mortality than urban counties,1,2 and lower CRC screening rates.3 -5 Colonoscopy is a critical component of screening recommendations to reduce CRC incidence and improve prognosis.6,7 Evidence exists that patient navigation (PN), which provides education, care coordination, barriers resolution, and motivational interviewing,8 -11 increases colonoscopy completion among medically underserved populations such as rural patients.12 -15 Patient navigators are often embedded within healthcare delivery systems, but PN can also be effective when the navigator is outside of the clinic.16,17 An offsite PN model serving multiple communities could bring PN to more patients to increase screening in rural regions.
Colonoscopy Outreach for Rural Communities (CORC) is a type 1 hybrid implementation effectiveness study 18 examining if a remote, PN program delivered by a lay person at an external community-based organization (CBO) can increase colonoscopy completion among patients from geographically disparate rural primary care organizations (PCOs). The CORC PN program is based on the New Hampshire Colorectal Cancer Screening Program (NHCRCSP), 16 a centralized navigation model that targeted uninsured and underinsured patients referred for colonoscopy across New Hampshire. A NHCRCSP study found that patients in the PN group were 11.2 times more likely to complete colonoscopy than control patients (96% vs 69%, P < .01). 16 Prior to undertaking this study, we made 3 adaptations to the NHCRCSP PN model to reduce the resource intensity of the program to make it easier to implement in rural communities: using a lay rather than nurse navigator, housing the navigator at a CBO, and reducing the number of topics to be discussed with patients. 13
Identifying and addressing barriers to implementation through contextual assessments and adaptations is critical.19 -21 The CORC program involved collaboration across 6 geographically and administratively distinct rural PCOs and a CBO, and required developing a new partnership between each PCO and the CBO. To improve likelihood of program success, we conducted a needs assessment and collaborative program adaptation with our study partners. This co-adaptation process is part of co-design, an established approach for engaging partners in identifying needs and building or adapting programs to meet those needs.22 -26 The goal of this study is to examine PCOs and CBO partners’ perspectives on potential implementation barriers and adaptations to mitigate potential barriers. The results informed final design and implementation of the CORC program and add to understanding of implementation contexts found in rural settings that might need to be accounted for before implementing an external virtual patient navigation program.
Methods
Study Design
We used a qualitative study design guided by content analysis methodology. 27 We conducted interviews with CBO and PCO staff to learn about their perspectives on determinants that could promote or impede CORC program success and intervention adaptations to mitigate those potential barriers. This study followed the Consolidated Criteria for Reporting Qualitative Research checklist. Study procedures were reviewed by a human subjects review board and determined to be exempt research (see Ethical Approval and Informed Consent Statements on the title page).
Guiding Framework
The Framework for Reporting Adaptations and Modifications-Enhanced (FRAME) is an implementation science framework that provides a construct to facilitate understanding of intervention adaptations.28,29 Table 1 outlines the FRAME application in this study. We focus our reporting on the FRAME questions of what was adapted, and the reasons and goals for the adaptations. The research team made final adaptation decisions prior to implementation, based on input gathered from key informants, and with the goal of preserving core intervention components. Using FRAME to detail the changes made and the rational for adaptations will help determine whether the modifications successfully addressed the adaptation goals,28,29 and it supports thick description to elucidate the relevance of findings to other contexts. 30
FRAME for CORC Co-Adaptation.

Setting
CORC partners include 1 CBO that employs and supervises the CORC navigator, and 6 rural PCOs across 3 states in the United States, Idaho (n = 1), Oregon (n = 1), and Washington (n = 4). CORC PCO partners were identified through collaboration with our partner CBO and the Washington, Wyoming, Alaska, Montana, Idaho (WWAMI) region Practice and Research Network. The CBO is a Primary Care Association that provides training and technical assistance to safety-net primary care providers. 31 Each PCO has between 2 and 9 primary care clinics and are federally qualified health centers (n = 4); hospital-affiliated (n = 1), or a Critical Access Hospital with federally designated Rural Health Clinics (n = 1). The PCOs are in either rural (n = 4) or rural serving (n = 2) communities, defined using 2013 Rural-Urban Continuum Codes. 32
Interview Recruitment
We used purposive sampling and reputational case selection 33 for interview recruitment. We asked each partner organization to identify staff across a range of roles and viewpoints who could serve as key informants: PCO staff with important perspectives on local CRC screening practices, and CBO staff who would participate in the CORC program. We invited potential key informants via email, shared the aims of the research, and offered a $100 gift card incentive. All but 1 invited staff member chose to participate.
Data Collection
The semi-structured interview guides asked about partners’ inner and outer settings, potential barriers (FRAME: reasons adaptations might be needed) and related adaptations (FRAME: what could be modified and reasons to modify). 20 Interview questions are in Supplemental Materials. Two experienced qualitative researchers comprised the primary analytics team, 1 who led tailoring of the program with partners (BI) and 1 with no prior relationship to partners (KO). The analytics team conducted 45- to 60-min one-on-one interviews via video call with 2 to 9 people per organization. We conducted interviews until no new codes or new understandings of existing codes were emerging, and the analytics team had confidence that data saturation was reached. 34 Four CBO staff and 25 PCO staff participated (Table 2). Interviews were audio-recorded and professionally transcribed.
Interview Participants.
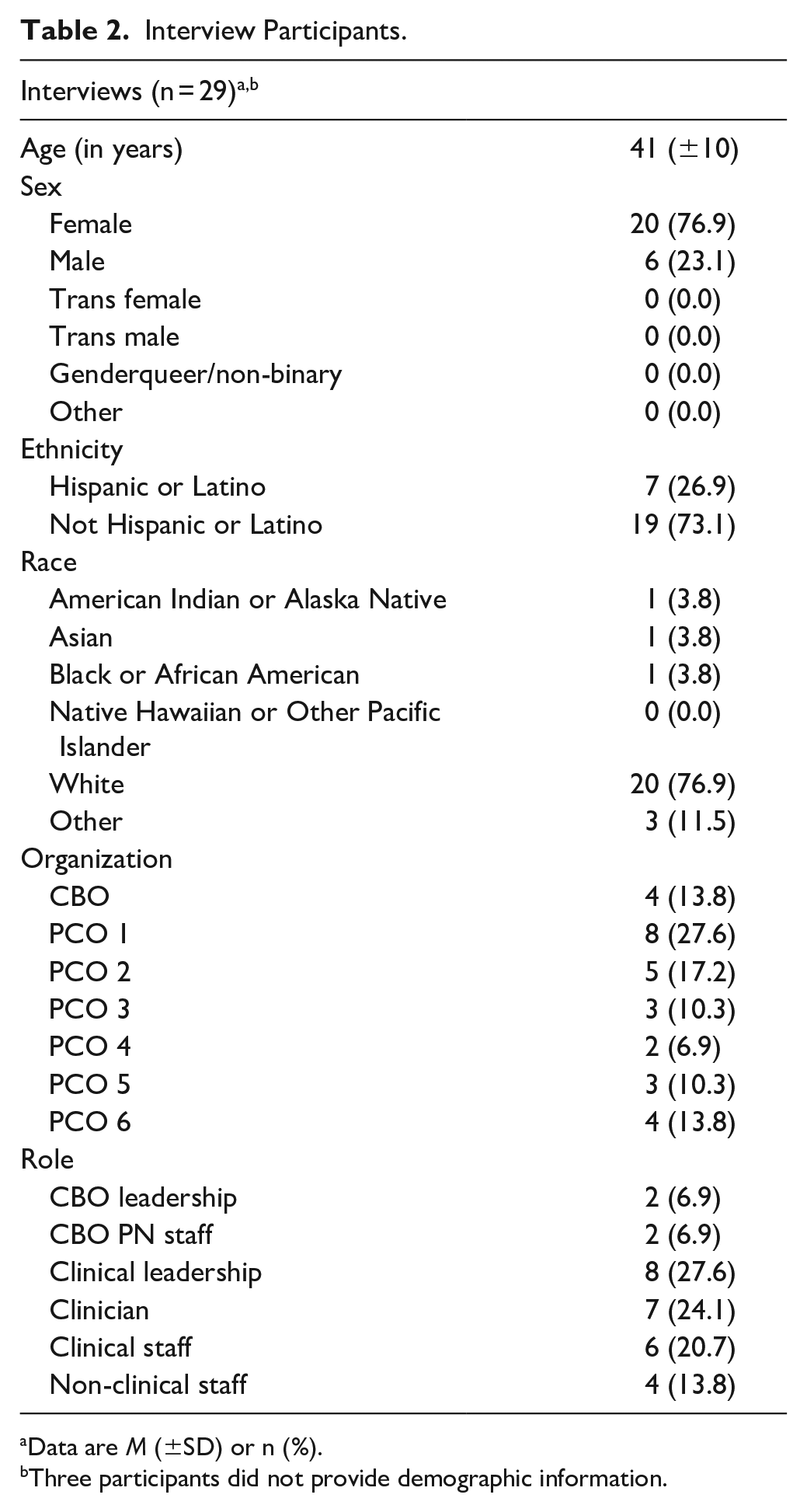
Data are M (±SD) or n (%).
Three participants did not provide demographic information.
Analysis
We used the Miles, Huberman, and Saldana 33 analysis approach of an iterative process of evolving data collection, data reduction and display, and conclusion drawing and verification across 3 levels: the key informant, the organization, and across all partner organizations as illustrated in Figure 1. Transcripts were independently coded by the analytics team with a codebook developed deductively based on the guiding questions and adjusted inductively to capture themes that emerged beyond the a priori questions. The analytics team met after each interview to write notes on emerging pattern codes and themes, create data displays interpreting each key informant’s perspective, and modify the interview guides and codebook in response to emerging themes using a constant comparison approach. Once interviews were complete at an organization, the analytics team met to discuss the findings within that organization, interpret patterns, and create displays of themes, which were sent to the organization for member checking. The broader study team reviewed each organizational analysis and discussed the relationship between themes across all organizations, further refining the themes across organizations. The primary analyst (BI) then checked that themes across organizations cohered, verified that each final theme was distinct, and confirmed its reliability by checking transcripts for confirmatory or challenging evidence. The CORC advisory group comprised of partner representatives and cancer program staff from a state health department then reviewed findings to validate whether they were representative of their understanding of CRC screening in rural communities. We conducted analyses in Dedoose. 35

Analysis process.
To enhance the trustworthiness of our data, we used Lincoln and Guba’s 30 criteria for credibility, transferability, dependability, and confirmability. We employed prolonged engagement, analyst triangulation, negative case analysis, and member checking to increase the credibility that our findings reflected key informant perspectives. To enrich understanding of the transferability of our results, we provided descriptions of the setting and participants, and documented adaptations using FRAME standards. 29 To achieve dependability and confirmability, we kept audit trails documenting findings and decisions through Transcript Review Forms and Case Analysis Forms and through researcher reflexive memoing and regular analysis discussions between multiple researchers to provide space to illuminate and question any hidden assumptions or biases. 33
Results
Through the needs assessment and co-adaptation process, we identified potential barriers to program implementation (FRAME: reasons for modifications) and adaptations to mitigate those potential barriers (FRAME: what to modify and goals of modifications). Adaptations were at the recipient, provider, and organization levels (Table 3).
Potential Barriers and Responsive Adaptations Reporting Using FRAME.
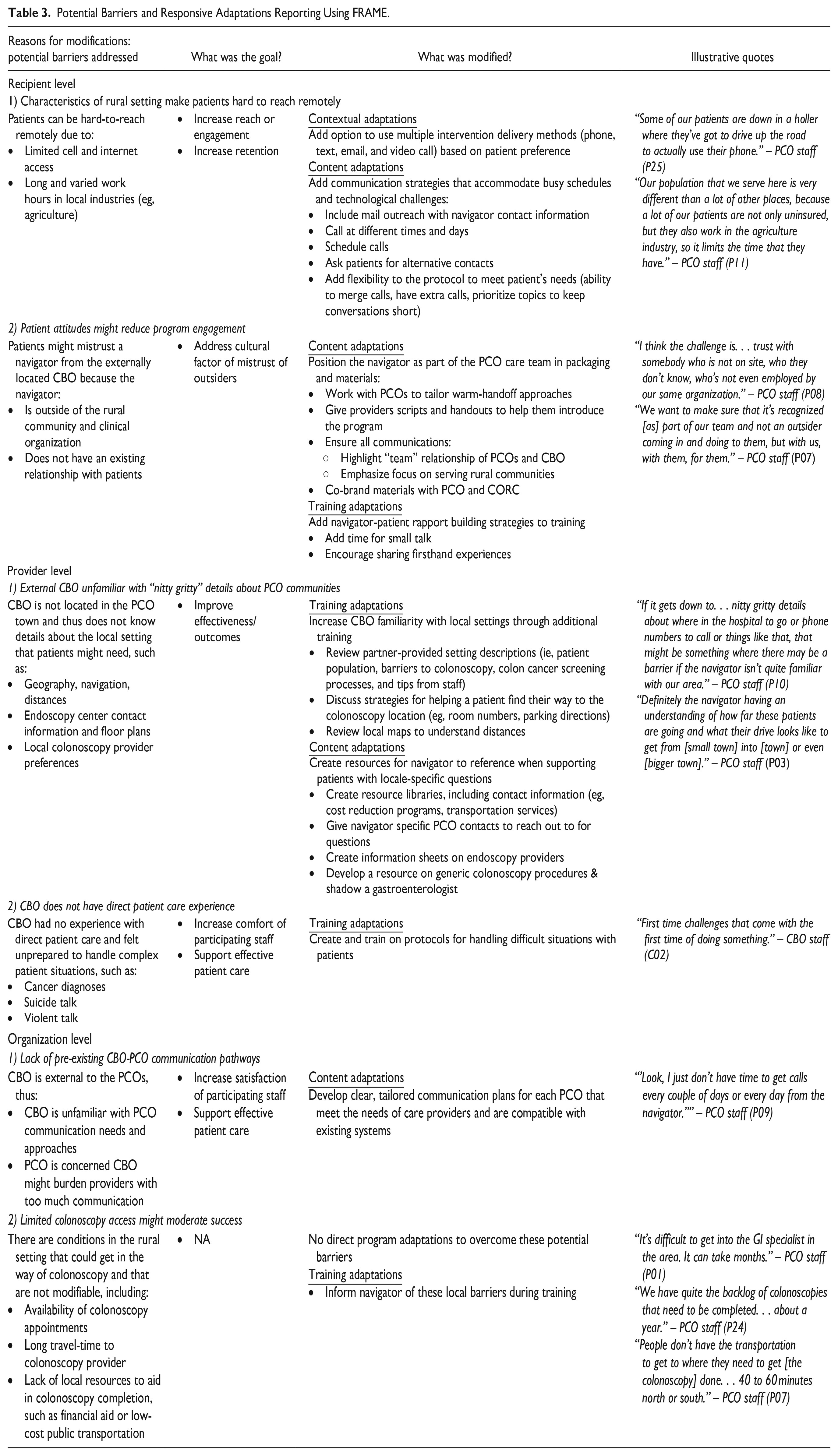
Recipient (Patient) Level Barriers and Responsive Adaptations
Characteristics of rural settings make it hard to reach patients remotely
PCO key informants shared that the long, varied work hours of local industry (eg, agriculture) and limited cell and internet access due to financial and technological challenges could be significant barriers to remote PN. To increase reach and engagement and also increase retention with hard-to-reach patients, we made contextual changes to the PN program (format) by adding the option to use multiple communication delivery methods (eg, mail, text, and phone call). We also made content changes to increase the number of communication strategies the navigator could employ to accommodate busy schedules and technological challenges (eg, asking for alternate contacts), and allowed flexibility to merge topics, add interactions, or prioritize topics to meet patient needs.
Patient attitudes might reduce program engagement
Key informants voiced concerns that patients might mistrust an unfamiliar navigator located at a CBO external to their community. To address these cultural factors, we made content adaptations to packaging and materials in order to position the navigator as part of the PCO care team. We ensured all communications highlighted the partnership with the PCO and the program’s rural focus, and supported PCOs in doing warm-hand offs to the CORC program through the creation of scripts and handouts. We also added trust and rapport-building strategies to the navigator’s training.
Provider Level Barriers and Responsive Adaptations
External CBO unfamiliar with “nitty gritty” details about PCO communities
Key informants feared that an external CBO would not be familiar with the “nitty gritty details” of the local settings. To increase the navigator’s knowledge of the patients’ communities in order to improve program effectiveness, we adapted the training plan to include reviewing setting information provided by each PCO (ie, patient population, barriers to colonoscopy, colon cancer screening processes, and tips from staff), discussing strategies to help patients find the colonoscopy provider, and reviewing maps to understand directions, distances, and drive times. In addition, we added community-specific content by creating navigator resource libraries to provide easy access information about services available in each PCO community to overcome common barriers to colonoscopy completion.
CBO does not have direct patient care experience
Since the navigator and CBO partner do not have experience providing direct patient care, they felt unprepared to handle complex situations. To increase the comfort of CBO staff and to support effective patient care, we added trainings about how to respond to patients in the case of difficult encounters such as those involving suicide talk, violent talk, or cancer diagnoses.
Organization Barriers and Responsive Adaptations
Lack of pre-existing CBO-PCO communication pathways
Key informants reported concerns about the lack of an established clinical care relationship between the CBO and the PCOs. They wanted the CBO to communicate in useful, actionable, and effective ways and to not burden providers. To increase satisfaction among partner organizations and support effective patient care, we added defined, tailored communication protocols to the intervention content. In general, PCOs wanted to hear from the navigator when patients declined colonoscopy, had a significant barrier the navigator could not help them overcome, or had an unrelated health complaint that needed attention.
Limited colonoscopy access might moderate success
A final potential challenge concerned environmental barriers to colonoscopy found in rural communities that a navigator might not be able to help patients overcome. These barriers included extensive backlogs at endoscopy providers, long distances and travel-time between endoscopy providers and patients, and the small number of community resources to support colonoscopy completion, such as transportation and cost resources. Although we could not directly address these issues in the CORC program, we adapted the training to ensure the navigator was aware that patients might need support with these challenges.
Discussion
We interviewed key informants from CORC partner organizations to identify potential barriers to program implementation and develop responsive adaptations to address these barriers. Throughout this process, we used FRAME to ensure we understood and articulated why a modification was needed, the goals of making a modification, and what the modification entailed. Our study highlights contextual factors that might need to be accounted for before implementing a remotely delivered, centralized patient navigation program serving rural communities. The potential barriers identified by key informants related to characteristics of the rural setting and attitudes of rural populations (eg, hard to reach patients and mistrust), and challenges of an outside non-clinical organization delivering the PN program (eg, lack of familiarity and interorganizational communication). While the literature supports patient satisfaction with patient navigation, 36 mistrust in public health and healthcare among rural residents is prevalent.37,38 Overcoming mistrust is essential in addressing disparities in use of preventive health services, 39 and collaboratively built approaches may be particularly important in addressing rural health disparities. 38 The needs assessment and collaborative adaptation highlighted the necessity of providing specific types of training for the navigator, and clearly outlining communication channels between each PCO and the CBO in order to overcome challenges inherent in using a centralized model and a lay navigator without clinical expertise. Ensuring appropriate training, resources, and triage were available for dealing with complex clinical needs that might arise while working with the navigator was an important adaptation to ensure patient safety and a successful relationship between project partners. Some rural-specific barriers (eg, limited resources to overcome barriers to colonoscopy completion) could not be addressed through adaptations to the CORC program. It will be important to consider the impact of those barriers when assessing the effectiveness and implementation of the CORC program.
Adapting interventions to the local setting and site-specific barriers is important to successfully implementing interventions,24,40 -43 and might be even more so for a virtual, centrally delivered program model due to its myriad diverse settings, remote communication methods, and new partnerships between CBOs and PCOs. Additionally, as evidence-based interventions are often tested in urban settings,44,45 and rural settings are heterogenous, collaboratively adapting interventions when implementing in rural environments is a critical step. FRAME provided a structure to support reflection on and documentation of the what and why of the modifications that emerged through the co-adaptation process.28,29 We anticipate that using FRAME to outline modifications to the CORC program will also support examining the success of these adaptations during the third phase of our study: evaluating implementation to inform future refinements and provide guidance for scalability. 28 In addition to the original goals for adaptation that we developed by applying FRAME, we found a need to add additional adaptation goals to FRAME to fully capture the reasons for adaptations. For example, it became apparent that increasing partner comfort was an important concept not included in FRAME and this study’s novel use of a CBO necessitated finding ways to make the organization comfortable with their new role. Without careful consideration of the goals of adaptation using FRAME, we may not have identified these potential barriers and addressed them.
There are several limitations to our study. CORC partner PCOs may not be representative of rural PCOs more generally. In addition, we did not include very small rural practices in the study as they had insufficient patient volume to practically partner on the study. These very small practices might greatly benefit from the shared patient navigator model, and it would be important to understand if they have different barriers and adaptation needs. We also did not include patients in the co-adaptation, and thus missed the opportunity to understand patients’ perspectives on program barriers. The data about the effectiveness of the adapted intervention is not yet available.
Conclusion
Partner engaged co-adaptation can lead to understanding of local needs and ensure CBOs and rural-serving PCOs can successfully partner to implement PN for cancer screening. Applying FRAME to our collaborative adaptation process aided us in discovering potential barriers and adaptation strategies. The collaborative process led to intervention adaptations intended to mitigate potential barriers identified by CORC partners and increase acceptability of the program across 6 different rural communities while leaving the core components of the evidence-based intervention intact.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319241288025 – Supplemental material for Adapting a Remotely Delivered Patient Navigation Program for Colorectal Cancer Screening in Primary Care: Important Considerations for Rural Contexts
Supplemental material, sj-docx-1-jpc-10.1177_21501319241288025 for Adapting a Remotely Delivered Patient Navigation Program for Colorectal Cancer Screening in Primary Care: Important Considerations for Rural Contexts by Brooke Ike, Gina A. Keppel, Katie P. Osterhage, Linda K. Ko and Allison Cole in Journal of Primary Care & Community Health
Supplemental Material
sj-docx-2-jpc-10.1177_21501319241288025 – Supplemental material for Adapting a Remotely Delivered Patient Navigation Program for Colorectal Cancer Screening in Primary Care: Important Considerations for Rural Contexts
Supplemental material, sj-docx-2-jpc-10.1177_21501319241288025 for Adapting a Remotely Delivered Patient Navigation Program for Colorectal Cancer Screening in Primary Care: Important Considerations for Rural Contexts by Brooke Ike, Gina A. Keppel, Katie P. Osterhage, Linda K. Ko and Allison Cole in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
The authors would like to sincerely thank our community partners for their insightful contributions to collaboratively adapting the CORC patient navigation program. The project is supported by National Cancer Institute of the National Institutes of Health under award number R01CA254515. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Author Contributions
AC conceived the original research idea. BI, KO, and LK contributed to the design and development of the study. BI and KO conducted the interviews and initial analyses, with additional interpretation input from GK, LK, and AC. BI drafted the manuscript with significant input from GK. All authors read, edited, and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project is supported by National Cancer Institute of the National Institutes of Health under award number R01CA254515.
Ethical Approval and Informed Consent Statements
Study procedures were reviewed by the University of Washington Human Subjects Division and determined to be exempt research (#00011808). Participants provided informed consent prior to participation.
Consent to Participate
Participants provided verbal informed consent prior to participation.
Consent for Publication
Not applicable.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.