
Abstract
Maternal mortality in the U.S. remains a pressing public health issue, with African American and Indigenous populations experiencing significantly higher rates. In Arizona, maternal mortality reached 30.0 deaths per 100,000 births in 2023, well above the national average. To address persistent maternal and child health (MCH) inequities, the Arizona Department of Health Services, in collaboration with a university and other strategic partners, conducted the 2025 Arizona Statewide Title V Maternal and Child Health Needs Assessment using community-engaged research (CeNR) approaches. Qualitative methods, including the River of Life (ROL) and Community Forums (CF), were employed to elevate diverse community voices, particularly from underserved rural, border, and minoritized populations. Key priorities identified included improving access to mental health care, addressing childcare shortages, expanding transportation and healthcare access, and strengthening culturally and linguistically appropriate services. The ROL approach revealed 8 social drivers of health, while CFs highlighted actionable solutions rooted in lived experience. Findings underscore the need for upstream policy investments and community-informed strategies to reduce maternal health disparities and improve statewide MCH outcomes. This participatory process demonstrates the value of engaging historically marginalized communities in shaping programs and policies that directly impact their health and well-being.
Introduction
Compared to almost all other industrialized countries, women and children in the United States experience higher rates of morbidity and mortality with evident racial and ethnic disparities. 1 Maternal mortality in the U.S. remains the highest of any high-income nation, twice as high as in the United Kingdom or Canada, with African American (AA) and Indigenous communities disproportionately affected.2 -4 In 2016, the U.S. maternal mortality ratio was approximately 16.9 deaths per 100,000 live births, with non-Hispanic AA and Indigenous women experiencing rates at least 3 times higher. 5 This trend has persisted, with recent data from 2023 indicating a maternal mortality ratio of 23.2 deaths per 100,000 live births.5,6
In Arizona, the ratio is even higher at 30.0 deaths per 100,000 births. 6 In 2023, the preterm birth rate for AA pregnant women was 13.2%, which is higher than the Arizona state rate (9.9%) and the national rate (10.4%), with chronic health conditions contributing to these rates.6,7
Maternal mortality is linked to racial, ethnic, socioeconomic, and geographic disparities, with African American women more than 3 times as likely as their white counterparts to die during pregnancy or childbirth. 1 Socioeconomic disparities lead to minority women entering pregnancy with fewer resources and often have higher rates of preexisting morbidity, such as cardiovascular conditions, obesity, and diabetes.1 As stated in the Centers for Disease Control (CDC), Maternal Mortality Prevention, more than 80% of pregnancy-related deaths are preventable. 8 One in 10 newborns is born preterm, also the highest proportion of any high-income country, with significant differences among racial and ethnic minorities. 9 Additionally, in the U.S., children and youth experience higher rates of poor health and developmental outcomes, including developmental disorders, mental health conditions, severe asthma, and obesity, than their counterparts in other countries. 10 The adverse health extends into adulthood, in which young adults aged 15 to 24 years have higher mortality rates than their counterparts in other countries. 11 The pattern continues throughout adulthood, thus shining a light on the importance of addressing the health needs of infants, children, adolescents, and young adults to improve long-term health outcomes. 1
The Arizona Statewide Title V Maternal and Child Health (MCH) Needs Assessment (Title V Assessment), led by the Arizona Department of Health Services (ADHS), is a comprehensive, community-focused assessment conducted every 5 years to determine the needs, or “gaps,” between current and desired outcomes. This paper focuses specifically on the qualitative assessment, but the ADHS-led assessment also included robust quantitative methodologies and partnerships with two tribal partners. The design and implementation of the assessment were guided by the Arizona Title V MCH Needs Assessment Steering Committee composed of MCH experts, grassroots organizations, agencies, and family and young adult advisors. The committee helped identify key community groups and locations for the forums.
As part of a strategic planning process, the needs assessment helps pinpoint strategic goals to be accomplished and provides an opportunity for improvement within a particular process or system 12 -15 Specifically, the assessment aims to enhance understanding of emerging issues within the maternal and child health (MCH) populations across each state and to best support activities with the Title V MCH Block Grant. The sampling methods addressed constraints related to time, resources, and distance.16 -18 Arizona’s fifteen counties are spread across 113,998 square miles. 19
While the 2020 Title V assessment demonstrated (1) reducing maternal mortality, (2) decreasing infant mortality, and (3) addressing substance use among pregnant women as high-priority outcomes,12,13 there are still gaps in healthcare for hard-to-reach populations, including people residing in rural/border areas, unsheltered communities, Latinos, immigrants, and people with special needs. The literature shows that adverse maternal health outcomes are related to structural barriers such as the lack of access to reproductive healthcare, transportation, discrimination, and the physical environment.6,20 Considering these potential barriers, we employed a community-engaged participatory research approach (CeNR),21,22 that prioritizes equitable partnerships with community voices and is further described in the Methods section.21,23,24 This methodology emphasizes building trust through inclusive representation and community empowerment, facilitating effective translation of knowledge to action, and includes, community-based participatory research (CBPR). 22 These methods are advantageous in fostering partnerships and meaningful dialogues with communities and centers on shared decision-making power. Moreover, engaging directly with communities allows researchers to recognize lived experiences and ensure that unique perspectives are included to address specific issues and enhance health outcomes.25 -28
CeNR has been applied in multiple contexts to amplify sustainable health improvements and to better understand underlying issues related to social determinants of health. It has also been used to inform the development of culturally tailored interventions through direct interaction with communities.29,30 A technique within the umbrella of CeNR is the River of Life (ROL), a visual, storytelling evaluation tool used to engage individuals to discuss and learn from each other’s lived experiences.22,31 This qualitative method has been successful in identifying key themes and priorities that may not otherwise be collected. 23 In the context of the Title V MCH Assessment, it is an advantageous technique that allows community members to interact with each other and researchers in a unique way that may not otherwise be achieved.23,24
CeNR, such as community listening sessions, community forums (CF), and key interviews, are incorporated in Title V state assessments nationally to assess community priorities and key themes regarding barriers to healthcare.32 -34 However, to our knowledge, the incorporation of ROL is unique to the Arizona Title V Assessment. The integration of ROL with CFs offered an effective platform for fostering engagement within the community.
Design and Methods
Study Design
The 2025 Title V Assessment was conducted by ADHS in collaboration with the University of Arizona Mel and Enid Zuckerman College of Public Health (MEZCOPH), and other external partners. The overarching principles for the assessment were developed by Arizona’s Title V steering committee. The Arizona Title V assessment steering committee membership included representatives from multiple sectors, including representatives from local and statewide nonprofit and advocacy MCH organizations, parents, community leaders, childcare associations and providers, county and state health departments, public and private institutions of higher education, health care providers and organizations, hospitals, community health workers, community health centers, and private practices.
Steering committee members engaged in each step of the assessment process, providing input on data collection methods, data analysis, and priority setting at steering committee meetings and community data collection and priority setting events.
A CeNR approach was chosen to align the study design with the overarching principles of the assessment and inclusion of community members engaged in critical dialogue to help us better understand their health needs.35 -37 Additionally, CeNR was employed to facilitate the collection of information from diverse groups across the state while simultaneously respecting the time restrictions of both the participants and assessment deadlines. The design of the assessment methods and analysis reflected the principles of CeNR. CeNR is a continuum of community engagement, which ranges from simply informing community members to a partnership CBPR, where community members participate in every step of the process. Community participants were involved in the planning and oversight of the assessment through the Title V assessment committee, involved in reviewing the findings and interpretation, and actively participating in prioritizing and assessing the feasibility of potential interventions. 38 Furthermore, community members were involved in decision-making, and the data were collected for the mutual benefit of the community and researchers. The partnership between the participants, community, and researchers was based on long-standing collaborations and respect.
This research was guided by a constructivist/interpretivist paradigm and employed ethnographic and phenomenographic approaches. We employed three innovative qualitative research methods grounded in the community engaged participatory principles, in this paper we will only discuss two of the methods, the ROL and the CF.39 -42 The third mixed-method approach, Group Concept Mapping (GCM) was used specifically with the states Black/AA population to ensure sufficient representation given the geographic spread and size of the population and critical MCH inequities facing members of the community. The Black/AA community in Arizona experiences the highest rates of infant prematurity, low birth weight, and maternal mortality than any other group in Arizona. 6 Members of the research team are preparing a separate paper focused solely on the Black/AA community.
We held eleven ROL sessions (ten in-person and one online) and eight CFs (six in-person and two online) across the state in both English and Spanish.
River of Life
ROL is an arts-based, equitable approach that provides a space for collaborative inquiry for participants from diverse linguistic, cultural, and socioeconomic backgrounds. ROL validates individual, community, provider, and other stakeholders’ expertise. The ROL exercise divides participants into small groups, and each group draws a river and symbols at the end of the river representing their goals (health outcomes) for MCH in their community and state (see Figure 1). Symbols drawn within the river represent the assets and barriers (social and political determinants of health) that impact their desired MCH outcomes.43 -45 The process transcends barriers related to social class, differential access to power and resources, educational attainment, and language barriers, through the creation of an equitable collaborative space. The arts-based nature of the method breaks down silos related to language, status, and educational attainment, as it does not require sophisticated communication skills, resulting in raising voices and honoring the expertise of all participants. The method has a broad reach and adapts well to different contexts and settings. 46 We met people where they were, from small groups of clients participating as they waited to receive services at large workshop sessions of more than 60 people. The ROL working groups ranged in size from two to six, allowing for self-facilitation. The self-facilitation component is a strength, expediting analysis as themes emerge organically through group discussions, symbols, and notes. The ROL methodology used in the state’s 2020 MCH Title V assessment was well received by participants and allowed the assessment to collect qualitative data from diverse groups. 13

River of life approach: (a) river of life methodological approach 47 and (b) example of river of life session.
Community Forums
CFs were held between September and November 2025 by a public health consultant hired by ADHS to share preliminary results collected by the health department and the University of Arizona Mel and Enid Zuckerman College of Public Health (MEZCOPH) with local service providers and stakeholders. CFs enable many individuals concerned about a situation to connect, share perspectives, and develop context-sensitive and sustainable solutions to the problem. 48 CFs also encourage original suggestions and concrete solutions for action. 48 After ADHS and the MEZCOPH shared preliminary findings, attendees worked in sub-groups to add, modify, or expand on the issues raised during the results section of the CF on sticky notes. Later, the consultant led an open discussion centered on the sticky notes, university and health department members helped to arrange the sticky notes following the community participants direction on the prioritization matrix. This prioritization matrix helps inform future programs, policies, and quality improvement of Arizona’s MCH services. 49
The data collection and analysis took a staged approach starting with the ROL data collection events. The preliminary data from the ROL events, once analyzed, were presented at the CFs along with quantitative data collected by the health department. Participants in the CFs reviewed and discussed both sets of data, providing feedback on the accuracy of the findings, identifying gaps, and offering additional information. After the initial discussion, they participated in activities that consolidated, prioritized, and assessed the relative “importance and changeability” of interventions (policy and programming).
Recruitment and Sampling
For ROL, participants were identified and invited to participate through purposeful and convenience sampling methods. 16 Combining sampling techniques made it possible to reach and engage members of vulnerable communities impacted by critical MCH issues and the related social and political determinants. The recruitment period for the ROL began in June 2024 and concluded in October 2024. Inclusion criteria for ROL included any English or Spanish-speaking adults over the age of 18 years as well as youth between 14 and 17 years of age from any race or ethnicity. With our recruitment strategy, we were able to recruit a total of 118 participants over 11 ROL sessions.
The locations for CFs were selected by the MCH Steering Community, who wanted to ensure representation from urban (n = 1), rural (n = 3), and border (n = 2) communities. The state health department spearheaded recruitment via email, social media, and word-of-mouth to local businesses and community partners’ social networks, ensuring they were open to the public and initiating a snowball sampling process. There were 130 participants across all CFs. Sectors represented in the CFs included CHWs, non-governmental organizations (NGOs), state and county health department employees, healthcare workers, community members, and agency/organizational leaders.
Procedure
Ethical Approval
Ethical approval for the study was obtained from the Institutional Review Board (IRB) of the University of Arizona, USA (STUD 00005052). The IRB determined that the proposed activity was not research involving human subjects as defined by DHHS and FDA regulations.
Coding and Analysis
Two data analysis strategies for the ROL results and CFs were employed in response to differences in the structure and purpose of the data collection sessions. Conventional content analysis was used for the ROL, and thematic analysis for the CF. Both coding strategies began with the data analysis steps common to both approaches. 50
Gained familiarity with the data and context. Including images and notes
Developed codes based on discovering noteworthy, key ideas/concepts in the data through visiting and revisiting the data.
Developed codes from first impressions and notes.
Organized the data into categories, creating themes and subthemes.
Refined categories using examples from the participant images and notes.
The data was reviewed and re-reviewed across data collection sessions and common data elements were integrated into the appropriate themes and subthemes.
Both content and thematic analysis can take an inductive approach and use similar coding processes. Content analysis, used for the ROL data, provide a broad, surface view, which was helpful in creating specific categories and is suitable for large data sets. Thematic analysis, used for the CF data, requires the researchers to immerse themselves in the data, providing a deeper understanding of the participants’ experience. 43
The ROL provided an overview of the participant’s MCH goals, objectives, and the related assets and barriers to attaining those goals. Once the ROL themes and subthemes were developed the themes were placed in the social drivers of health categories (SDOH). The ROL sessions were large and provided a broad understanding of the health issues and related assets and barriers to attaining MCH outcomes for their communities.
The results of the ROL sessions, along with the quantitative results from ADHS were presented at the CF, where participants discussed the issues in depth, prioritized, and assessed the feasibility of developing interventions. The CF required a richer discussion of the context and issues to meet the CF objectives; thus, thematic analysis was more suitable.
Validity-Trustworthiness and Reliability
Validity in qualitative studies refers to the portions of the study design substantiating the rigor and thoroughness of the research. Approaches used to ensure the validity of the findings were built into the study design and assessment process. For example, we used member checking, triangulation, and rich thick description to validate the results.51 -53 Member checking and triangulation were integrated into the ROL sessions through discussions within individual groups, and whole group, presentations and discussions. The reliability of the analysis for both methods was established and confirmed through scheduled research team meetings where the analysis and the coding schemes were reviewed and discussed. Members of the research team cross-checked the coding schemes. The CF review served as an addional peer review assessing the validity of the data analysis. 51
Results
We reached all fifteen counties in Arizona, and community members representing historically underserved and rural communities. Participants in the data collection sessions included service providers or people with lived experiences in one or more of the following areas: pregnancy, children with special health care needs, housing insecurity or unsheltered, low-income, domestic violence, involvement with the justice system, recovery from substance use or alcohol disorder, uninsured or underinsured, mental illness or behavioral health disorders, seeking asylum, undocumented, or mixed immigration status households.
The mental health sub-themes arising from the CF included increasing awareness about services, reducing stigma, increasing funding for programs, and increasing access to services, funding, providers, and treatment.
ROL Results
Pictures and notes are the primary data source for the ROL. Each group entered their group’s basic de-identified demographic information, stakeholder type, community, and county via a QR code. We used content analysis to refine and merge the themes and subthemes. Each collection event was analyzed separately and later combined.51,52 Eight themes related to the social drivers of health (see Figure 2 and Table 1) emerged from the ROL sessions. The assets were grounded in community integration, family, community health workers (CHWs), non-profit community, and government safety net resources and services. The barriers were in part related to upstream factors, including a lack of awareness of and limited resources needed to reinforce the social safety net and address the social determinants of health and health equity.54,55 The Political determinants of health mentioned included policy related to immigration status eligibility, social and health resources, and access to services. The need for additional investment in improving food system shealthcare, childcare, and housing infrastructure was emphasized.

Social drivers identified by The River of Life Sessions and Community Forums.
Identified Themes and Participants Quotes from ROL.

Policy and action recommendations progressed naturally from the rich discussions among the participants during the ROL, including but not limited to (1) focus on results and action, (2) fostering an inclusive, collaborative process, and (3) valuing the expertise of the community, effectively integrated into the research and community engagement methods.20,39,45,56 Figure 3 presents the policy recommendations stemming from the ROL discussions. The recommendations focus on the upstream social and political determinants impacting the barriers and building on the assets identified in the discussions. The recommendations include short- and long-term policy solutions to increase access to service, such as providing non-traditional clinic hours to better accommodate patients’ work schedules, increasing federal funding for safety net programs, and increasing employee benefits. The policy and action recommendations align and build upon the community assets, including increasing the availability of home visiting programs, increasing funding for community resources, and better reimbursement for Doulas. The participants suggested more long-term investments in MCH and communities, such as increased support in rural areas, improving transportation systems, and accessible housing and preschool education. Additional action and policy recommendations included affordable transportation for rural and urban communities, increased access to services, childcare, food, housing, and increased support for families and communities (see Figure 3).
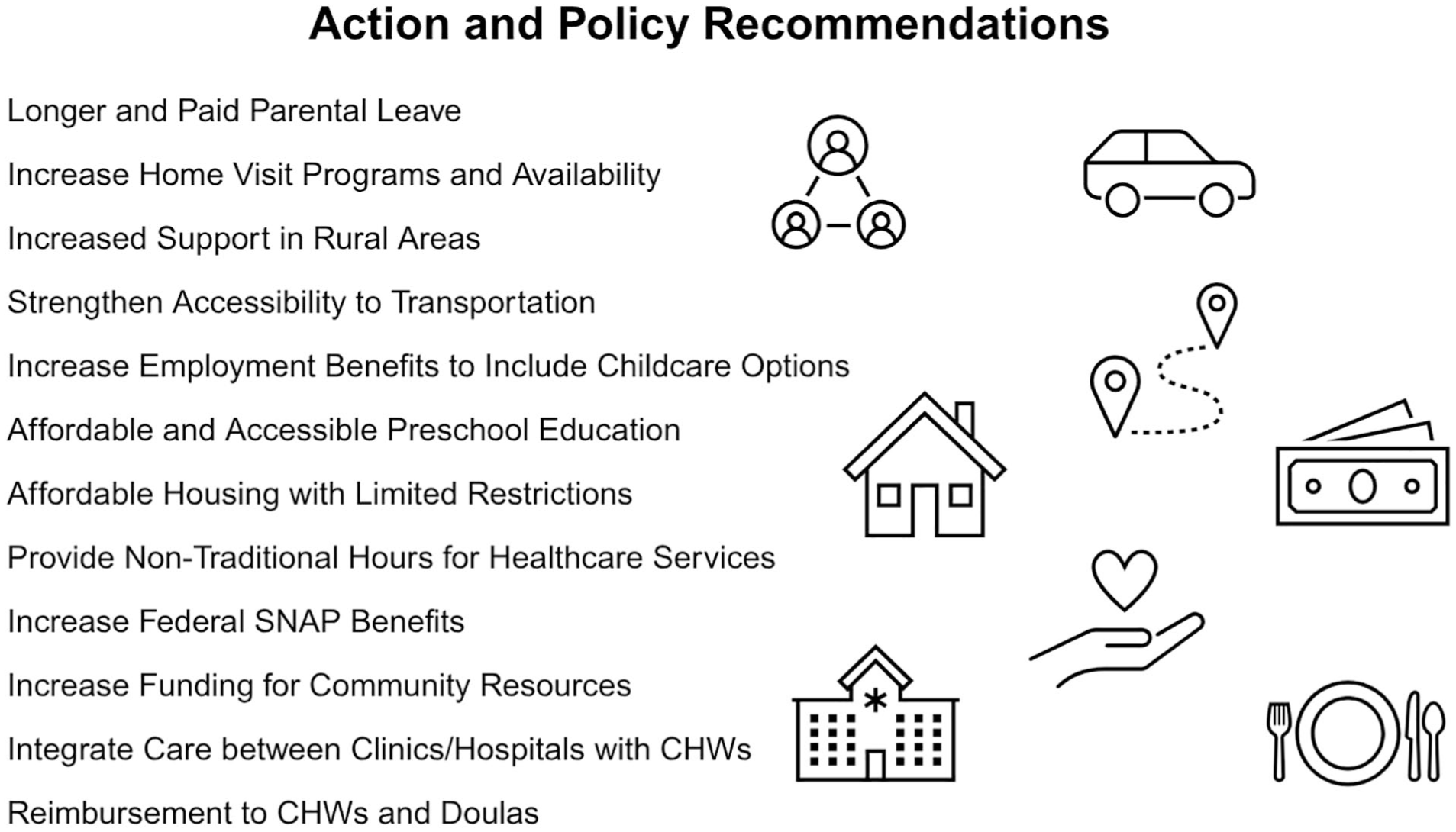
Policy recommendations based on ROL.
Community Forum Results
The qualitative data collection for the CF came from notetaker summaries and participant comments from diverse sectors and counties across the state. The CFs were not recorded; thus, only some direct quotes are shared below. Three research team members independently reviewed the forum notes, followed by group discussions to develop a shared coding tree and preliminary theme definitions through consensus. Mental health, childcare, family support, transportation, food assistance, financial resources, culturally and linguistically appropriate services, and promotion of available health resources were among the top health-related priorities (Figure 2).
Mental Health
Community members repeatedly emphasized the urgent need for mental and behavioral health promotion services and programs. Suggested initiatives included support groups, suicide prevention efforts, stigma reduction strategies, and broader mental health awareness campaigns. Participants advocated services tailored to specific populations, including youth, adults, pregnant and postpartum individuals, and maternal and paternal mental health support. Youth-focused programming, particularly within school settings, was highlighted as a critical strategy for suicide prevention and early intervention.
In addition to identifying needs, participants described significant barriers to accessing care. These included the unaffordability of mental and behavioral health services, a shortage of qualified mental health providers, particularly in rural, border, and underserved urban areas, and a lack of culturally and linguistically appropriate care. Community-driven solutions proposed during the forums included increased funding for mental and behavioral health programs, enhanced access to postpartum depression education and screening, expanded treatment options for individuals with substance use disorders, particularly pregnant people, coupled with stigma-reducing education, and improved access to and availability of treatment facilities for substance use disorders.
Yo sí creo, que salud mental, para mí, está más difícil de cambiar. Porque creo que traen esos cambios grandes, como al nivel gobierno. Porque va junto con los servicios personas que califican para seguro médico o no. Por eso no tienen salud mental, el tratamiento. No es nada más conciencia o buscando recursos. Para mí es un cambio más grande. [Translation: I believe that mental health, for me, is more difficult to change. Because it is a large change at the government level. Because it goes together with medical services for people who qualify. That is why they do not have mental health treatment. It is more than awareness and finding resources]. Virtual Group, Spanish.
Childcare
Like mental health, childcare was a consistently raised concern across all CFs. Participants described limited childcare options within their towns and cities, with some noting that even when facilities were available, they often lacked qualified caregivers. Others expressed frustration that facilities with more qualified staff were unaffordable for many working families. In rural communities primarily, the scarcity of formal childcare services has led families to rely on informal networks. One participant shared that she regularly saw community members posting on Facebook to ask who might be available to watch their children. Representing a local organization, she explained they were informally tracking families in their area who were actively seeking childcare, highlighting a grassroots response to a systemic service gap. Participants emphasized that the shortage of affordable, quality health care as a critical public health issue. 57 The lack of affordable, quality childcare has not received sufficient recognition or attention as a public health issue from policy makers and researchers. The inability to access childcare impacts parental mental health and renders healthcare inaccessible, contributing to poor health outcomes. Utilizing CenR methods in community health assessments creates an equitable and inclusive space where community voices/perspectives contribute to the policy development process.
In reference to the lack of childcare and provider shortage: the lack of childcare “feeds into the provider issue,”
I talk to women and men who say they miss appointments due to childcare. I brought it up and was told that it is not our issue, but it is. Childcare is a public health issue. Maricopa County Health Center Behavioral Health Provider
Primary and Specialty Care Shortage
The concern over shortages in primary and specialty care providers was a recurring theme due to the challenge of retaining providers in underserved communities. One participant from a remote region stated, “There are no incentives for providers to stay . . . nothing they want for their families in our town.” Many also discussed how loan repayment programs, while helpful in recruiting providers temporarily, contributed to high turnover. Once providers completed the required service hours for student loan forgiveness, they often left, resulting in a lack of continuity in care. The CF believed this cycle harms community trust and long-term health planning.
Transportation
Transportation continues to be a significant barrier to accessing healthcare and other critical services. Participants noted the complete lack of public transportation infrastructure, particularly in rural areas. When individuals needed to travel for medical procedures or specialty services, they were often required to drive several hours to the nearest metropolitan center. This option is not feasible for many without a reliable vehicle or flexible work schedule. This challenge extended beyond healthcare, impacting access to education, employment, and healthy food. Participants reinforced the urgent need for community-based transportation solutions that are affordable and accessible. The participants highlighted the impact of insufficient and differential access to transportation.“Us in programming have money for transportation but limited”, “We have transportation, but ends at 5 pm”.
Access to Quality and Affordable Healthcare
Across all forums, participants emphasized the limited availability and high cost of healthcare services. Many expressed frustrations with eligibility restrictions for public insurance or sliding-scale clinics. Several participants shared that income thresholds were unreasonably low, forcing families to make impossible choices. One participant explained, “You must quit your job to qualify.” Another stated, “It is a broken system.” Participants also voiced concern over the inconsistency in quality of care and long waiting times, particularly for specialty services. Many mentioned that food insecurity is seasonal/conditional: “Fluctuates due to primary industry of produce, seasonal work in the area that affects food insecurity.” A lack of cultural and language alignment between providers and patients often compounds these barriers.
Community Education and Awareness of Resources
Forum participants acknowledged a lack of awareness and health education as barriers to care and prevention. Many community members were unfamiliar with existing programs or unsure how to navigate the healthcare system. Despite these challenges, participants also pointed to community strengths, particularly collaboration between local organizations. One participant from a border community remarked, “We work really well as a community. We all come to the table and work together.” These collaborative efforts are assets and offer the opportunity to improve outreach and service coordination. CHWs were identified as important assets for accessing health resources. “CHWs make a difference.” “We work with family, we know how to connect people.” The value of CHWs to improving health outcomes was mentioned across the state “Strong CHW programs, they are the boots on the ground.”
Access to Healthy and Affordable Food
Participants identified urban and rural food deserts as another concern with limited access to affordable, nutritious food, especially for low-income families and individuals living far from grocery stores. Participants noted that they were often priced out of reach, even when healthy food options were available. These conditions contributed to diet-related chronic diseases and highlighted the need for localized food systems, subsidies, and culturally relevant nutrition education.
Culturally and Linguistically Appropriate Services (CLAS)
Across all regions, participants stressed the need for culturally and linguistically appropriate healthcare services. Many noted the lack of bilingual providers and culturally relevant materials as a critical barrier to equitable care. In the Spanish-speaking forums, participants expressed concern about the limited number of Spanish-speaking mental health professionals. The participants highlighted the importance of bilingual providers and culturally relevant services given the demographics of our state, “Most of the workforce here is bilingual. We are bicultural. We navigate two countries, and this changes pathways that people can take. They have different cultural values, different beliefs, and they may be getting care in some other country.
One participant summed up the need for bilingual and culturally relevant services
También estoy de acuerdo con [participant]. Necesitamos muchos trabajadores de salud mental que hablen español. Casi no hay en nuestras comunidades que sean bilingües. Es alta necesidad y además es difícil. Va tomar tiempo y un proceso para tener más psicólogos, trabajadores sociales, consejeros capacitados en los dos idiomas. Para poder llevar esto a la comunidad, especialmente a la habla Hispana. [Translation: I agree with the other participant. We need many more mental health workers who speak Spanish. There are hardly any bilingual people in our communities. It is a high need, and it will take time and a process to have more psychologists, social workers, and counselors trained in both languages. We must bring this to the community, especially the Spanish-speaking community].
Dental and Oral Health
Dental and oral health emerged as another critical area of concern. Participants reported few options for dental care in their communities, with affordability and insurance coverage as significant barriers. A common sentiment was that “Dental plans do not take insurance,” and many providers did not accept Medicaid or discounted plans. Families with young children were particularly affected. One participant shared, “Our local dentist will not take the little ones,” highlighting the limited pediatric dental care options, particularly in rural and low-income areas.
Discussion and Conclusion
Despite national and state efforts, maternal mortality and preterm birth disparities remain severe. ROL and CF participants consistently identified barriers such as lack of access to reproductive and prenatal care, transportation, systemic discrimination, and culturally competent providers, contributing to adverse MCH outcomes. ROL and CF demonstrated that art-based and participatory methods are powerful tools for engaging communities often excluded from traditional assessments. The strengths of this study were that the methods validated lived experiences and drew out nuanced, locally grounded priorities. In addition, we engaged the community through trusted social networks and successfully reduced barriers like mistrust and stigma. Using these engagement strategies is important for reaching historically excluded populations or those who experience discrimination. Primary ROL results highlight community-defined goals such as increased culturally responsive care, expanded maternal mental health services, more robust CHW involvement, tailored outreach for families with children with special healthcare needs, and policy and system change around reproductive justice. CF confirmed findings from ROL sessions and allowed communities to prioritize action areas.
Addressing inequities related to the lack of accessible community and culturally relevant services requires an upstream approach, given the magnitude of the problem. In both ROL and CF, we heard from families about the gaps in their community. In some cases, families offered solutions to the problems identified. While at other times, they expressed feelings of defeat. Utilizing these two methods allowed community members to share their thoughts about assets and barriers. During the prioritization, the participants highlighted the issues they felt that the state health department should heavily consider. It is also important to note the participants’ acknowledgement and gratitude for the CHWs and local programs that directly fill urgent needs. Demonstrating how effective community-based programs and CHWs know how to best reach and address problems is a strategy that larger organizations and agencies might consider adopting. It is also important to highlight the intersection of the needs, for example, how the lack of quality childcare can impact a provider’s decision whether or not to stay in smaller rural communities.
Limitations of the Study
Although the teams reached all 15 counties, we could not truly get a deep understanding of the individuals’ lived experiences from each county. While the point of qualitative research is not to quantify experiences, we also understand that assessments aim for greater representation. Another limitation was time and funding; we had a short time period to complete the assessment and to present findings to the state health department and MCH steering committee. Our core team had to develop strategies for how we would plan, recruit, and implement ROL rapidly. However, without the inclusion of MHU staff, we would have had a much smaller team. Lastly, we consider that some viewpoints and suggestions provided a year ago may have changed. We suggest for those trying to implement these methods in a needs assessment, to ensure that researchers secure additional funds to support a larger team with sufficient time to complete the assessment.
Using CeNR methods enables more equitable representation in the needs assessment process and captures the realities of MCH disparities in the state. Using these methods with the proper engagement infrastructure allows marginalized populations to meaningfully contribute to statewide health planning in an even playing field. The data collected will inform the state’s MCH priorities in a culturally competent and community-driven manner, ensuring that resources target the issues that matter most to the communities. These methods may serve as a framework for other states seeking to incorporate CeNR into their Title V assessments or public health planning efforts. The researcher’s future directions include building long-term partnerships with communities, integrating our findings into program design and funding decisions, evaluating long-term outcomes, and disseminating findings to communities to maintain accountability and transparency.
Footnotes
Acknowledgements
We want to acknowledge the valuable contributions of community members and stakeholders who participated in this assessment and shared their insights/perspectives. We also extend our appreciation to the students in the University of Arizona HPS Directed Research Course and the Primary Prevention Mobile Health Unit team who assisted with this project. Additionally, we thank our partner organizations and facilitators whose collaboration was essential throughout the process.
ORCID iDs
Ethical Approval
The University of Arizona IRB determined that the proposed activity is not research involving human subjects as defined by DHHS and FDA regulations.
Consent to Participate Statements
Before the start of any data collection session, we explained the purpose and objectives of the study to the participants and how the information would be used. The participants were informed that their participation was entirely voluntary, and they were free to leave at any time. We informed them that the final results from all of the data collection events would be shared widely through both virtual and in-person community presentations. Thus participation in the study was voluntary.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Arizona Department of Health Services, Arizona, USA, through InterAgency Service Agreement (ISA) No: CTR069432 (J. Ehiri, PI). The views expressed in this publication are those of the authors and do not necessarily reflect the official policies or positions of the Arizona Department of Health Services.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Requests for de-identified data can be made to the corresponding author, who will need to obtain permission from the UA and ADHS.