
Abstract
Introduction:
The scope of primary care increasingly encompasses patient behavioral health problems, manifest typically through depression screening and treatment. Although substance use is highly comorbid with depression, it is not commonly identified and addressed in the primary care context. This study aimed to examine the association between the likelihood of substance use disorder and increased depression severity, both cross-sectionally and longitudinally, among a sample of 2409 patients from 41 geographically dispersed and diverse primary care clinics across the US.
Methods:
This is secondary analysis of data obtained from a multi-site parent study of integrated behavioral health in primary care, among patients with both chronic medical and behavioral health conditions. Patient reported outcome surveys were gathered from patients at 3 time points. The primary care practices were blind to which of their patients completed surveys. Included were standardized measures of depression severity (Patient Health Questionnaire—9) [PHQ-9] and substance use disorder likelihood (Global Appraisal of Individual Needs—Short Screener [GSS]).
Results:
Four percent of the study population screened positive for substance use disorder. PHQ-9 scores indicated depression among 43% of all patients. There was a significant association between the likelihood of substance use disorder and depression initially, at a 9-month follow-up, and over time. These associations remained significant after adjusting for age, gender, race, ethnicity, education, income, and other patient and contextual characteristics.
Conclusions:
The findings suggest that substance use disorder is associated with depression severity cross-sectionally and over time. Primary care clinics and health systems might consider implementing substance use screening in addition to the more common screening strategies for depression. Especially for patients with severe depression or those who do not respond to frontline depression treatments, the undermining presence of a substance use disorder should be explored.
Introduction
Among persons with depression, substance use disorders are a common comorbidity.1 -5 Patients with comorbid depression and substance use disorders suffer greater functional impairment, poorer medical outcomes, increased morbidity and mortality, and greater risk for suicide compared to patients with depression alone.6 -8 Increasingly recognized are the advantages to addressing the behavioral health concerns of both adult and pediatric patients in general health care contexts.9,10
Primary care is an optimal setting to discern and respond to behavioral health issues. There are at least 4 documented benefits: (1) behavioral health problems, like physical health problems, are more amenable to preventative interventions at earlier stages11,12; (2) patients with behavioral health problems are more likely to surface in primary care than in specialty care 13 ; (3) patients prefer having behavioral health concerns addressed by their primary care team14,15; and (4) health care costs, particularly in the use of specialty services (ED, hospital, and psychiatric care), are reduced.16,17
A cornerstone of primary care’s strategy for addressing patient behavioral health is systematic depression screening, as recommended by the US Preventative Task Force and supported by Medicare/Medicaid Incentivized Payments Systems (MIPS). 18 Approaches to integrated behavioral health in primary care (IBHPC), such as the Collaborative Care Model, have been increasingly adopted.19,20 In these models, patients are systematically screened, assessed, monitored, and treated for depression in primary care, typically with the support of embedded behavioral health expertise from clinical social workers and consulting psychiatrists.18,21
The most commonly used instrument for depression screening with established psychometric properties is the 9-item Patient Health Questionnaire-9 (PHQ-9).22,23 This measure is often used for universal (2-item version) and indicated screening (full 9-item version) and to develop care pathways based on PHQ-9 total score categories. 24 The PHQ-9 can also be used for measurement-based care purposes. 25 Although the PHQ-9 may be perceived as reductionist by psychiatry specialists, it is embraced by primary care because of its brevity, face validity, and widespread adoption.22,23,26
In contrast to depression screening, substance use disorder screening is rarely performed in routine primary care.26 -28 Despite the high comorbidity between depression and substance use disorders, few studies have examined the direct influence of substance use on depression in primary care.5,29 -32 In fact, studies focused on depression in primary care often exclude individuals with substance use problems.33,34 Yet substance use may drive severe depression initially and render frontline primary care interventions, such as anti-depressant medications, less effective.8,32,35 -37 Likewise, depressed mood may contribute to the initial use of substances to cope and eventually lead to a substance use disorder. There have been national rollouts to promote and implement substance use screening and brief interventions in primary care (eg, Screening, Brief Intervention and Referral to Treatment [SBIRT]). 38 Unfortunately, these endeavors have neither incorporated depression screening/treatment nor been widely adopted or sustained in routine healthcare operations.39,40
The current study examines the association between depression and substance use disorder cross-sectionally and longitudinally. The findings of this study may have implications regarding the benefits of systematic screening for substance use in addition to depression, particularly among patients who do not respond to frontline interventions for depression, or who have comorbid medical problems.
Methods
Parent Study Description
The Integrating Behavioral Health and Primary Care for Comorbid Behavioral and Medical Problems (IBH-PC) study was a multi-site randomized trial described in detail elsewhere. 41 The IBH-PC trial collected patient-reported outcomes (PROS) at 3 timepoints in surveys of adults with co-occurring chronic medical and behavioral health conditions sampled from 41 primary care practices across 13 geographically diverse states (see Figure 1). All patients had access to primary care with co-located behavioral health services and had attended a minimum of 2 primary care visits over 24 months, including at least 1 in the last 6 months. Practices varied in geography, population density, patient panel size, specialty, and ownership and were blind to the patients who participated in the PROS data collection. Baseline and midpoint data surveys were collected pre-COVID-19 (September 2017-January 2020), while follow-up surveys were collected during the COVID-19 pandemic (March 2020-February 2021). Of the 2651 respondents that met inclusion criteria for the main study at midpoint and follow-up time points, 2409 had complete data for this sub-analysis.

Distribution of integrating behavioral health and primary care practice locations.
Measures of Outcome and Predictor Variables
The primary outcome variable was depression, measured by the PHQ-9, which is a reliable and valid self-report measure of current depression severity used by many health systems. 24 The PHQ-9 corresponds to the American Psychiatric Association Diagnostic and Statistical Manual (DSM) criteria for mood disorders and measures depressive symptom severity. 24 The PHQ-9 total score ranges from 0 to 27, with cut points for mild, moderate, and severe depression.
The primary predictor variable was the 5-item GAIN-Short Screener (GSS), which assesses the likelihood of a current substance use disorder. 42 For the GSS, “substance” includes alcohol and other drugs. The GSS was developed and validated as a brief and practical alternative to the Global Appraisal of Individual Needs (GAIN-I), a 2-hour semi-structured clinical interview designed to estimate severity based on DSM criteria. The GSS identifies the recent consequences of alcohol and drug use as a self-reported measure and is highly predictive of a substance use disorder diagnosis.42,43 For adults, GSS total scores range from 0 to 5, and are interpreted at 3 levels or categories: disorder unlikely, disorder possible, and disorder probable. For these analyses, we considered GSS total scores of 2 or more as diagnostic.42,44
Because the baseline IBH-PC surveys did not include the GSS for all study participants, we used the IBH-PC midpoint and follow-up surveys as the “initial” and “final” data points for the present analyses.
Potential Confounding Variables
To examine and isolate the influence of substance use on a change in depression scores, we conducted multivariable linear regression models adjusted for individual-level demographic and health status, as well as multiple social determinants of health care access. These factors included: age, gender, employment status (employed full-time, part-time, student or homemaker vs not), annual household income (<$30 000 vs ≥$30 000), education (associates degree or less vs college graduate or more), chronic pain (yes vs no), insecurity in food, housing or finances (yes vs no), the time between initial and final surveys, and the Social Deprivation Index (SDI). Chronic pain was one of many behavioral health conditions used as inclusion criteria for the parent trial and included headache, migraine, neuralgia, fibromyalgia, or chronic musculoskeletal pain. Medical records were reviewed to determine patient eligibility. Food, housing, and financial insecurities were collected via patient self-report. 45 The SDI is a census tract-level composite measure of deprivation derived from the American Community Survey based on income, education, employment, housing, single-parent household, and access to transportation. 46
Data Analytic Approach
Chi-square tests and Wilcoxon rank-sum tests were used to compare social, demographic, and clinical variables between those with and without a current substance use problem. There were 3 primary analyses performed for this study. First, we assessed the cross-sectional association between substance use disorder (GSS) and depression (PHQ-9) from the initial survey. Second, we assessed the cross-sectional association between GSS and PHQ-9 in the final survey. Third, we evaluated the longitudinal association between the change in GSS score and PHQ-9 score from the initial to final survey. Multivariable linear regression models were used to estimate the association between depression and likelihood of substance use disorder. Potential confounds to the association between the predictor and outcome variables were treated as covariates. If a covariate changed the coefficient of the main predictor (GSS) on the outcome (PHQ-9) by more than 10% in a model with no other covariates, it was included in the final multivariate model as a potential confounder. All tests were 2-tailed, with a threshold for statistical significance at α = .05. Stata 17 (StataCorp LP, College Station, Texas) was used for data management and analysis. The University of Vermont Institutional Review Board approved this study.
Results
Participant Characteristics
Of the 2651 respondents that met the inclusion criteria for the main study at both time points, 2409 had complete data for this sub-analysis. At the initial survey, 101 (3.8%) met criteria for a substance use disorder a (GSS substance use severity score of 2 or more). Those with substance use disorder were younger and more likely to be male, employed, without a college education, and facing food or financial insecurities. The participants with probable substance use disorders had better DASI cardiovascular capacity scores and higher PHQ-9 depression scores. There was little difference in race, ethnicity, social deprivation score, marriage status, income, chronic pain, or housing insecurity. See Table 1.
Participant Characteristics at the Initial Survey (n = 2651).
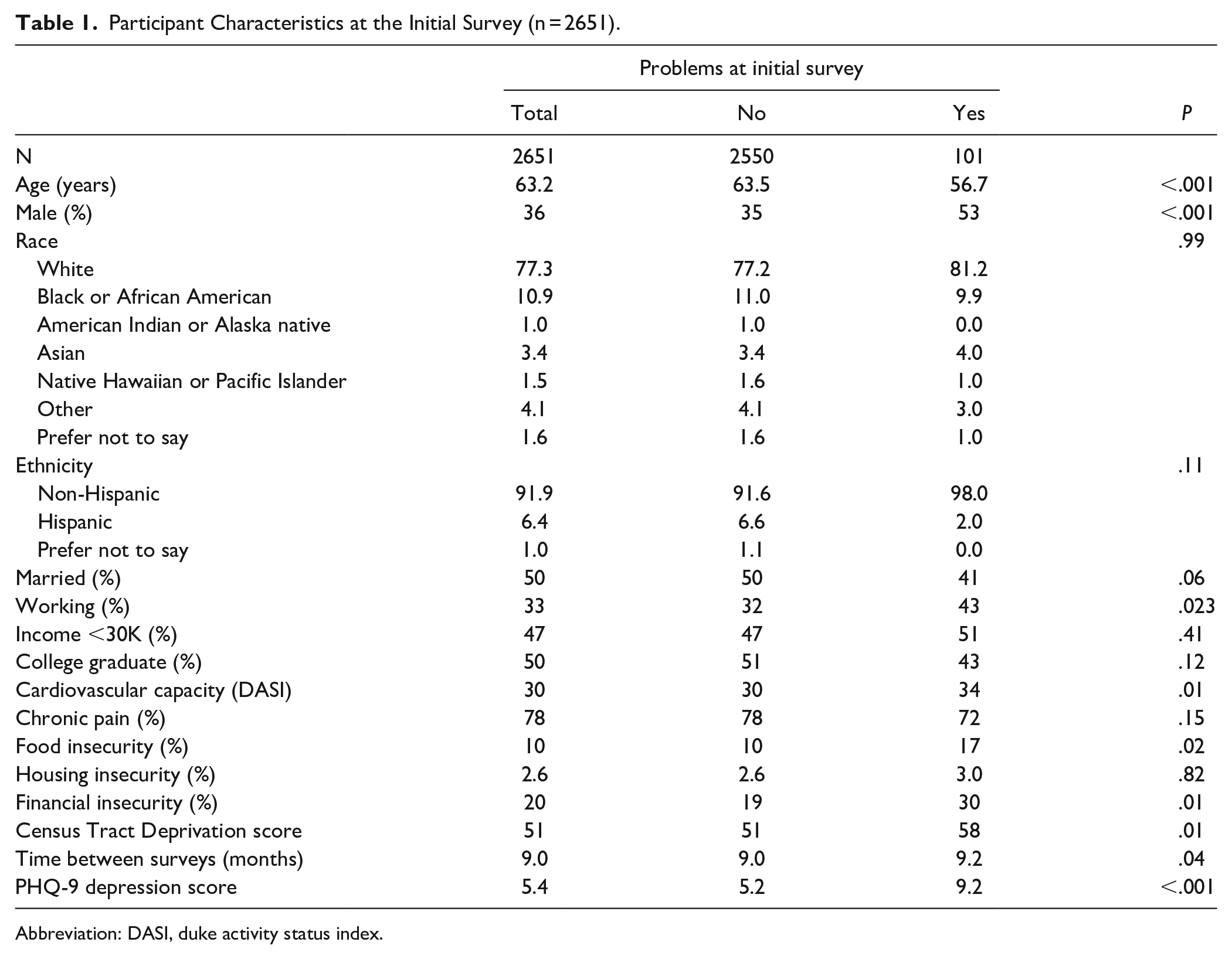
Abbreviation: DASI, duke activity status index.
Substance Use Disorder
The mean GSS score was 0.3 (SD = 0.7) at both time points (P = .5). At the final survey, 109 patients (4.1%) scored 2 or more and met criteria for a substance use disorder. While the sample of patients with substance use disorders was slightly different at the 2 time periods (about one-third of the patients met criteria at both time points, one-third met criteria at initial survey only and one-third met criteria at final survey only), the demographic attributes of the patients with likely substance use disorder at the final survey did not differ from those in the initial survey.
Depression Severity
In the initial survey, the mean PHQ-9 depression score was 5.4 (SD = 5.6), and in the final survey 5.3 (SD = 5.6) (P = .52) (See Table 2).At the initial survey, 1146 of the 2651 (43%) of patients scored in the mild depression or worse categories. See Table 2 for the distribution of PHQ-9 scores.
Distribution of PHQ-9 Total Scores by Timepoint (n = 2651).

As seen in Figure 2, each box plot represents the distribution of PHQ-9 scores for patients with the indicated GSS score.

Distribution of the relationship between depression severity (PHQ-9) and substance use severity (GSS) at each timepoint.
At baseline, the linear regression showed strong evidence for a relationship between higher GSS scores and higher PHQ-9 scores. For each one-point increase in the GSS score, the PHQ-9 score increased by 0.61 points (95% confidence interval (CI) 0.29, 0.92; P < .001). After adjustment for potential confounders, the effect size was 0.77 (CI 0.49, 1.05; P < .001) (Table 3). In the final survey, the unadjusted regression showed a 0.8-point increase in PHQ-9 score for every unit increase in GSS score (CI 0.50, 1.09; P < .001). The adjusted effect was 0.91 (CI 0.65, 1.18; P < .001).
Final PHQ-9 (Depression) Score as a Function of GSS (Substance Use Severity) Score.

Least-squares linear regression; β = regression coefficient; CI = 95% confidence interval. Variables with (reference group) include: for race (White), Married (never married, separated, divorced, widowed), sex (female).
Longitudinal Analyses Assessing Change in Depression as a Function of Change in Substance Use Over Time
This final analysis modeled change in PHQ-9 from the initial survey to follow-up as a function of change in GSS, while adjusting for initial PHQ-9 score and potential confounders. There was a 0.44 point increase in the PHQ-9 score for every one-point increase in the GSS score. This suggests a significant association of substance use and depression severity over time, even after adjusting for confounding factors. (CI 0.22, 0.66; P < .001).
Discussion
Four percent of a large and diverse sample of primary care patients met criteria for a likely substance use disorder based on a standardized self-report screening measure (GSS). On a widely adopted standardized self-report screening measure for depression, 43% met criteria for at least mild depression. There was a significant association between substance use disorder and depression severity both cross-sectionally and over time. The associations were significant after adjusting for both patient and contextual characteristics. Although the relationship between substance use disorder and depression severity has been documented in prior studies, this is the first and only study to examine this relationship longitudinally in a large sample of patients from geographically diverse primary care practice setttings.5,8 On a much smaller scale, a quality improvement project in a primary care clinic by Watkins et al, similarly found substance use prolonged mood disorder symptoms despite provision of depression treatment. 5
Limitations
The non-experimental nature of this study inhibits inferences about cause and effect. The study does not discern whether substance use precipitates depression or the reverse. Nor can we infer a common etiological pathway to both substance use and mood-related disorders.
We have limited information on factors that may mediate change in depression or substance use between time points. Significant omissions could include the use of anti-depressant or addiction medications, behavioral therapies, and peer recovery support groups. IBH-PC approaches, Collaborative Care Model, or similar integrated interventions might have directly addressed either substance use, mood disorders or the both. Although the PHQ-9 is a common measure of depression in medical contexts, the GSS is not. More typical measures of substance use disorder likelihood could have been used for greater generalizability. These measures include instruments such as the CAGE, the Alcohol Use Disorder Identification Test, the Drug Use Disorder Identification Test, or more recent measures such as the TAPS and TAPS2.47,48 Furthermore, the GSS does not specify the type of substance(s) that drive the substance-related diagnosis. There could be a differential relationship with depression by substances such as alcohol, cannabis, opioids, benzodiazepines, and/or stimulants.49 -51
Nonetheless, the GSS assesses the likelihood of a substance use disorder with a high level of reliability and validity. 43 The GSS balanced accuracy with a low respondent burden to achieve the study purposes. However, all self-reported measures of substance use in general health care settings likely provide under-estimates of actual substance use disorder.52,53
Conclusions
These findings suggest increasing the capacity of primary care providers, clinics, and systems to at least screen for and potentially address both depression and substance use. 54 Presently, depression screening is common in primary care practice settings, 55 whereas screening for substance use is not widely implemented.26,28 Yet there are multiple examples of primary care having an encouraging impact on substance use problems among patients.13,56 -59 These include: primary care use of addiction medications for opioid use disorder, SBIRT approach to alcohol use disorders; and, adaptations of the Collaborative Care Model to address a broader range of behavioral health issues beyond only depression.38,56,60,61
The present findings underscore the strong relationship between depression and substance use, independent of salient patient and environmental characteristics, and may challenge provider biases.62 -64 Although those with substance use problems were statistically more likely to be younger, male, employed, without a college education, and facing food or financial insecurities, there was little to no difference in race, ethnicity, social deprivation score, marital status, income, chronic pain, or housing insecurity. These findings suggest that primary care providers might consider any patient at potential risk for substance use problems, regardless of demographic factors.65,66
Future research might address some of the limitations inherent in the present study. Enhancements would feature a prospectively designed study of primary care patients with depression, substance use, or both disorders; more systematic tracking of mood and substance use symptoms over multiple timepoints; and, measuring outcomes of interventions that target both types of problems among complex chronic patients.
To summarize, these findings suggest that substance use disorder complicates depression initially and over time. Primary care clinics and health systems might consider implementing substance use screening in addition to the more common strategies for depression. For patients with either severe depression or who do not respond to frontline depression treatments, the undermining presence of a substance use disorder should be explored.
Footnotes
Acknowledgements
The authors are grateful to the patients and staff of the 41 primary care practices who participated in this study. In addition, the following individual contributors were key to the study’s execution: Jessica Clifton PhD, Abigail M. Crocker PhD, Laura-Mae Baldwin MD, MPH, MD, Ryan E. Breshears PhD, Peter Callas PhD, Prama Chakravarti PhD, Kelly Clark/Keefe, Deborah J. Cohen PhD, Frank de Gruy MD, Lauren Eidt-Pearson MSW LICSW, William Elder PhD, Chet Fox MD, Sylvie Frisbie, Katie Hekman RN, Juvena Hitt MPH, Jennifer Jewiss EdD, David C. Kaelber MD PhD MPH, Rodger Kessler PhD, Jennifer B. O’Rourke-Lavoie, C.R. Macchi PhD, Matthew P. Martin PhD, Brenda Mollis MPH MPA MA, Daniel Mullin PsyD MPH, Zsolt Nagykaldi PhD, Lisa W. Natkin PhD, Wilson Pace MD, Richard G. Pinckney MD MPH, Douglas Pomeroy, Paula Reynolds, Sarah Hudson Scholle DrPH MPH, Jeni Soucie MS, William J. Sieber PhD, TerryStancin PhD, Kurt C. Stange MD PhD, Kari A. Stephens PhD, Kathryn Teng MD and Constance van Eeghen DrPH MHSA MBA. Lastly, We would like to acknowledge the many contributions of key stakeholders for their explicit efforts to guide us in patient-centered research: Andrea Auxier, Sarah Bartlett, Dana Basiliere, Andrew Bertagnolli, Georgia Brown, Anne Donahue, Florence Fee, Walter Grant, James Hester, Gene (Rusty) Kallenberg, Katie MacDonald, Susan McDaniel, Ricka McNaughton, John Muench, and Andrew Pomerantz.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded through a Patient-Centered Outcomes Research Institute (PCORI) Award (PCS-1409-24372). The views, statements, and opinions presented are solely the responsibility of the authors and do not necessarily represent the views of PCORI, its Board of Governors or Methodology Committee.