
Abstract
Background:
Depression commonly coexists with chronic medical illness and is associated with impaired self-management, poor adherence, increased healthcare utilization, and higher mortality.
Objective:
To synthesize evidence published between 2000 and late 2025 on the effectiveness of the Collaborative Care Model (CoCM) for depression in adults with chronic medical illness, with particular attention to contemporary U.S. implementation, policy, and equity considerations.
Methods:
A narrative review of randomized controlled trials, pragmatic and implementation studies, systematic reviews, and policy analyses was conducted using PubMed, PsycINFO, and Scopus. Evidence addressing collaborative care for depression in adults with chronic medical illness was identified and synthesized thematically in accordance with best practices for narrative reviews.
Results:
Landmark trials and meta-analyses demonstrate that collaborative care consistently improves depression outcomes across chronic disease populations. More recent studies indicate that CoCM remains effective in real-world settings using digital registries, telepsychiatry, and population health workflows, although implementation remains uneven due to workforce and access constraints.
Conclusions:
Collaborative care represents a durable, evidence-based approach for integrating depression management into chronic illness care. Sustaining effectiveness as systems scale will require preserving core model components while addressing persistent workforce, digital, and equity barriers.
Keywords
Introduction
Depression commonly coexists with chronic medical illness and affects up to 1 in 5 adults with conditions such as diabetes, cardiovascular disease, and chronic kidney disease, contributing to higher mortality, impaired self-management, and increased healthcare utilization.1-4 Beyond symptom burden, comorbid depression undermines adherence to medical treatment and amplifies functional disability across disease contexts.5-7 Despite this well-established impact, depression in patients with chronic illness remains inconsistently identified and inadequately managed in routine care, in part because traditional primary care systems are not designed for sustained behavioral health follow-up.8,9
The Collaborative Care Model (CoCM) was developed to address this gap by integrating behavioral health management directly into chronic care delivery. In this model, a designated care manager conducts systematic symptom monitoring using validated instruments such as the Patient Health Questionnaire-9 (PHQ-9), coordinates treatment with the primary clinician, and participates in regular psychiatric caseload review to guide stepped-care adjustments. Landmark randomized trials and subsequent meta-analyses have demonstrated that CoCM improves depression outcomes and is cost-effective across a range of chronic medical conditions.10-12
Several systematic and narrative reviews have previously synthesized the effectiveness of collaborative care for depression.12,13 However, much of this literature predates recent shifts in health system organization, reimbursement policy, and digital infrastructure that now shape how CoCM is implemented in real-world practice. Since 2022, expanded reimbursement through the Centers for Medicare and Medicaid Services (CMS), broader Medicaid adoption, and increased reliance on telepsychiatry and digital registries have altered both the feasibility and scale of collaborative care delivery in the United States.14-19 At the same time, growing attention to health equity has highlighted persistent disparities in access to integrated behavioral health care among rural populations and racial and ethnic minoritized groups.20-25
Accordingly, the purpose of this narrative review is to synthesize evidence on the effectiveness of CoCM for depression in adults with chronic medical illness while situating this evidence within the context of contemporary U.S. implementation, policy, and equity considerations. International trials are included to establish the clinical effectiveness of collaborative care, whereas implementation and policy evidence is examined primarily through a U.S. lens to reflect current delivery environments relevant to primary and community health practice.
Methods
This manuscript follows the Scale for the Assessment of Narrative Review Articles (SANRA) framework for narrative reviews, emphasizing clearly defined aims, transparent literature identification, balanced referencing, and structured interpretive synthesis. 26 As a narrative review, the approach prioritizes conceptual integration and clinical relevance over systematic enumeration or exhaustive study tabulation.
A structured approach to evidence identification was employed. Searches were conducted in PubMed, PsycINFO, and Scopus, and literature published between 2000 and late 2025 was considered. Search strategies combined keywords and controlled vocabulary related to collaborative care and chronic illness, including collaborative care, integrated care, depression, primary care, and chronic disease categories (eg, diabetes, cardiovascular disease, and chronic kidney disease). Representative search combinations included: (“collaborative care” OR “integrated care” OR “behavioral health integration”) AND (“depression” OR “major depressive disorder”) AND (“chronic disease” OR “diabetes” OR “cardiovascular disease” OR “chronic kidney disease” OR “chronic pain”) using database-specific controlled vocabulary (eg, MeSH terms in PubMed). Searches were limited to English-language publications from January 1, 2000 through October 2025.
Eligible studies included randomized controlled trials, pragmatic and implementation studies, systematic reviews, and policy analyses addressing the Collaborative Care Model for depression in adults with chronic medical illness. To ensure conceptual consistency, included interventions were required to meet an operational definition of CoCM, comprising: (1) a designated behavioral health care manager embedded within primary or integrated care; (2) systematic symptom monitoring using validated instruments (eg, PHQ-9); (3) regular psychiatric caseload review to guide treatment recommendations; and (4) stepped-care treatment adjustment based on measured outcomes.27,28 Studies lacking these core components were excluded, even if described as “integrated” or “collaborative” care.
An initial screening identified 53 potentially relevant articles, of which 38 met inclusion criteria and informed the narrative synthesis. Evidence was synthesized thematically across 4 domains: (1) effectiveness across chronic disease contexts; (2) implementation strategies and barriers; (3) workforce and digital adaptations; and (4) equity considerations. Table 1 presents selected landmark and contemporary studies to illustrate foundational and recent evidence, while the remaining studies informed the broader interpretive synthesis across sections.
Selected Landmark and Contemporary Studies Illustrating the Effectiveness of Collaborative Care Across Chronic Illness Contexts.

This table presents illustrative landmark and recent studies highlighting the evolution and breadth of evidence supporting collaborative care. It is not intended as an exhaustive or systematic summary of all included studies.
Methodological rigor and clinical relevance were considered during interpretation, with greater weight given to randomized controlled trials, large pragmatic studies, and high-quality systematic reviews. Evidence on clinical effectiveness was drawn from both U.S. and international studies, whereas implementation, policy, and equity analyses were intentionally focused on the United States. Formal risk-of-bias scoring was not performed, consistent with narrative review methodology.
Results
Evidence Evolution
Across the 38 included studies, collaborative care has been associated with improvements in depression outcomes among adults with chronic medical illness across diverse disease contexts and care settings. Interpretation emphasized recurring patterns across disease categories, care settings, and study designs rather than exhaustive enumeration of individual trials.
Early randomized controlled trials established foundational efficacy, while subsequent pragmatic and implementation studies demonstrated durability under real-world conditions. Landmark trials such as IMPACT and TEAMcare showed that structured, team-based depression management improved both mood and disease-related outcomes.5,10 These findings were reinforced by systematic reviews and meta-analyses demonstrating superior remission, improved adherence, and favorable cost-effectiveness.9,11-13 Selected landmark and contemporary studies informing this evidence base are summarized in Table 1.
More recent studies (2022-2025) indicate that CoCM remains effective when supported by digital registries, telepsychiatry consultation, and population health workflows.14,15,30-32 Observed benefits consistently appear to arise from structured measurement, accountability, and iterative treatment adjustment rather than specific technologies or medication strategies.
Condition-Specific Findings
Diabetes
Collaborative care improves both depression outcomes and glycemic control. TEAMcare and the Pathways Study demonstrated significant reductions in PHQ-9 scores alongside improved HbA1c.5,27 Sustained benefit was most closely associated with systematic symptom tracking and stepped-care adjustment.14,32
Cardiovascular Disease
Among patients with coronary artery disease and recent cardiac events, collaborative care improves depressive symptoms and medication adherence, even when physiologic changes are modest.29,33,34
Chronic Pain and Musculoskeletal Conditions
Integrated behavioral activation and stepped pharmacologic management improve function, depression severity, and reduce opioid reliance.13,30,35
Chronic Kidney Disease
Telepsychiatry-enabled and hybrid CoCM models demonstrate meaningful improvements in depressive symptoms and treatment adherence.15,30
Implementation Evidence
Programs embedding CoCM within population health or primary care teams demonstrated greater sustainability than stand-alone initiatives, particularly when supported by structured registries and regular psychiatric case review.5,15,33,36 Standardized PHQ-9 tracking and registries were associated with higher remission rates and improved continuity.34,35 Automated prompts and structured case-review meetings increased adherence to stepped-care protocols.27,29 Hybrid telepsychiatry models achieved outcomes comparable to traditional models while expanding access.31,32
Key implementation barriers and illustrative strategies identified across recent U.S.-focused studies and policy guidance are summarized in Table 2.
Common Implementation Barriers and Illustrative Strategies for Collaborative Care Adoption in U.S. Practice (2022-2025).
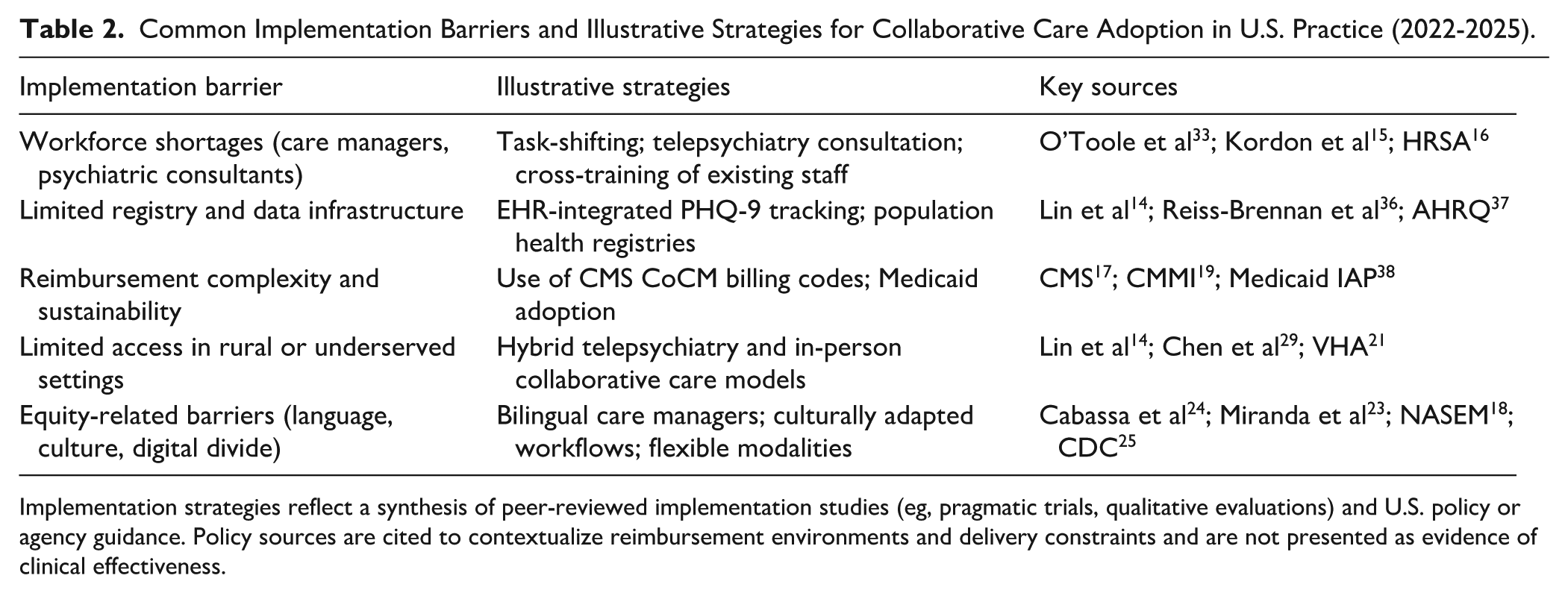
Implementation strategies reflect a synthesis of peer-reviewed implementation studies (eg, pragmatic trials, qualitative evaluations) and U.S. policy or agency guidance. Policy sources are cited to contextualize reimbursement environments and delivery constraints and are not presented as evidence of clinical effectiveness.
Discussion
Interpretation of the Evidence
Evidence consistently demonstrates that collaborative care improves depression outcomes across chronic medical conditions. Early trials established efficacy, and later meta-analyses confirmed robustness across heterogeneous populations.5,9,13 Contemporary studies indicate that effectiveness persists in safety-net, rural, and digitally enabled settings.14,15,30,33
Policy Context and System-Level Expansion
Policy documents cited here contextualize implementation environments rather than serve as evidence of clinical effectiveness. Expanded reimbursement through CMS, Medicaid, and the Veterans Health Administration has facilitated scale.17,19-22,38 However, implementation research indicates that reimbursement alone is insufficient without organizational capacity and protected infrastructure.15,33,36
Equity, Access, and Structural Constraints
Disparities in access persist among rural and minoritized populations.22,23,31 Culturally adapted models improve engagement while preserving fidelity.20,21 Technology alone does not mitigate inequities without broadband and workforce investment.18,25
Implications for Practice
Collaborative care represents best practice for depression in chronic illness. Early identification, standardized tracking, and team-based adjustment improve outcomes and adherence.5,10,34 These principles support continuity across care transitions.30,31,38
Research Priorities
Future work should address sustainability, cost-effectiveness, and mechanisms of benefit. Registry use, supervision frequency, and stepped-care intensity are key mediators.14,15,31 Emerging evidence extends CoCM’s role to suicide prevention and digital adaptation.39,40
Conclusions
Collaborative care consistently improves depression outcomes among adults with chronic medical illness across clinical contexts.5,13 Structured symptom monitoring, psychiatric consultation, and stepped treatment adjustment embedded in routine care are associated with durable improvements in depressive symptoms and continuity of care.10,31,34
Effectiveness appears to derive from structured accountability and measurement-based care rather than any single technological component.31,34 Across disease categories, benefit arises from sustained accountability and team-based decision-making.5,29,30,35
Recent U.S. evidence indicates that collaborative care has transitioned from an efficacious intervention to a scalable delivery model, supported by reimbursement and digital infrastructure.15,17,19,33 Ongoing workforce shortages and funding instability continue to shape access.15,16,18,25
Preserving core components as systems scale will be essential. When implemented with fidelity and contextual sensitivity, collaborative care offers a pragmatic pathway for integrating mental and physical health in primary and community care.
Footnotes
Acknowledgements
The authors thank Tropical Texas Behavioral Health for institutional support and access to integrated behavioral health data resources that informed this narrative review.
Ethical Considerations
Not applicable. This article is a narrative review and does not involve human participants or identifiable data.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
No datasets were generated or analyzed during this study.