
Abstract
Objectives:
Many behavioral health providers (BHPs) in primary care practices spend a majority of their time addressing mental health rather than behavior change. We wanted to better understand the practice of BHPs in integrated primary care.
Methods:
Survey of BHPs from practices participating in the Colorado State Innovation Model (SIM) initiative. The survey measured what diagnoses BHPs receive referrals to treat, what they treat regardless of referral reason, which techniques they use, and think are most effective for mental health diagnoses and behavior change/weight management support, and their interest in providing support for weight management. Results were analyzed using descriptive statistics and Spearman correlations.
Results:
We received 79 surveys representing 64 out of 248 SIM practices (practice response rate of 26%). BHPs reported addressing health-related behaviors with patients referred to them for mental health diagnoses. They expressed interest in health behavior and believed the techniques they use for traditional mental health diagnoses also support behavior change. Most reported using cognitive behavioral therapy (89%), mindfulness (94%), and relaxation/stress management (94%). Time in practice was associated with receiving more referrals for weight management (rho(76) = .271, P = .018) and with addressing diet (rho(75) = .339, P = .003) and weight management (rho(75) = .323, P = .005). BHPs in practices that had care managers were more likely to report receiving referrals for weight management than BHPs in practices that did not employ a case manager (
Conclusions:
BHPs are interested in and frequently address health related behavior. Formalizing health behavior services from BHPs in primary care may provide opportunities to better support patients with behavior change and subsequently improve health outcomes.
Introduction
Behavioral health care, when integrated into primary care services, is defined as “care for patients around mental health, substance abuse conditions, health behavior change, life stresses and crises, as well as stress-related physical symptoms.”1,2 Although many people report having mental, behavioral, and substance related needs, lack of access to care remains a problem in the US.3,4 Partly due to lack of access, there has been significant effort to integrate behavioral health services into primary care settings. Early evidence indicates that integrated behavioral health care increases access to behavioral health care and leads to equivalent or improved outcomes including improved identification and treatment of mental health diagnoses such as depression, improved use of self-management plans, and decreased healthcare expenditures.5-8
In the primary care setting, Behavioral Health Providers (BHPs) are often licensed clinical master’s or doctoral level professionals, trained in social work or psychology. BHPs in primary care settings can also include licensed professional counselors or licensed marriage and family therapists and occasionally psychiatrists or psychiatric nurse practitioners. BHPs in primary care can treat mental or behavioral health issues such as depression, anxiety, substance related issues, as well as issues around health behavior including managing chronic pain, smoking cessation or weight management support.6,9 The literature suggests they often focus on mental health conditions rather than health behavior issues.10-12 However, health behavior is linked to the onset and outcomes for many chronic health problems commonly encountered in primary care such as obesity, diabetes, hypertension, lung disease, liver disease, and osteoarthritis. There is strong evidence that interventions for obesity and chronic disease prevention and treatment that include BHPs in supporting patients are associated with improved outcomes such as weight reduction and improved glycemia for people with diabetes.13-16
Although BHP help could improve patient outcomes for many chronic conditions, the literature indicates that BHPs in integrated settings primarily treat patients for traditional mental health diagnoses such as depression and anxiety and do not as frequently work with patients on behavior change.17-21 It doesn’t seem that the issue is lack of patient interest in behavior change help. Specific to obesity, people routinely report not receiving behavioral health interventions to support weight loss through their primary care providers (PCPs) despite being interested in such care.22-25 BHPs in integrated primary care settings bring training and skills in health behavior change that may increase practices’ capacity to address health behavior change issues that are associated with many chronic conditions. It is also posited that BHPs are overly consumed with mental health issues and are constrained by capacity. In this study, we sought to examine these issues about the BHP role: what conditions and care BHPs in integrated settings in Colorado currently provide and to what extent are they interested and available to provide assistance with behavior change, health promotion, and weight management.
Methods
This study was a cross-sectional survey to understand work around mental health and behavior change by BHPs in integrated primary care, the approaches BHPs use, and whether BHPs were providing, and/or interested in weight management. We were also interested in whether provision of weight management is associated with factors such as time in practice.
Study Setting and Population
The target population for this study included licensed BHPs working in integrated primary care practices in Colorado that participated in the Colorado State Innovation Model (SIM) project. SIM was a Centers for Medicare and Medicaid Innovation-funded project supporting integration of BHPs into multidisciplinary primary care teams at a variety of primary care practices across the state. Practice locations and settings in SIM were diverse and included rural, urban, and suburban; small, medium, and large; and private practice, health system, academic, and safety-net clinics. As this survey was conducted as part of program evaluation for the Colorado State Innovation Model (SIM), it was not considered human subjects research and was deemed as exempt by the Colorado Multiple Institutional Review Board.
Survey Instrument
Because validated scales to measure the main constructs do not exist, the investigators developed the survey questions with input from practicing BHPs as well as content experts on integrated behavioral health (PhD academicians and clinicians with research and professional experience in integrated behavioral health). The survey was pilot tested and revised with practicing BHPs. The survey collected demographics, training, and work environment factors and assessed perceived PCP referral patterns to BHPs by diagnosis or health behavior. BHPs were asked whether they receive referrals for specific diagnoses or health behaviors (“multiple times daily, multiple times weekly, multiple times monthly, rarely, or never”). They were asked a similar question about the mental health or health behavior issues they treat regardless of referral reason. BHPs were given a list of possible approaches (generated by study team with assistance from practicing BHPs and content experts) and asked whether they used the approach. They were then asked to list the approaches they think are most effective for mental health diagnoses, behavior change in general, and weight management specifically. They were also asked about their interest in providing weight management interventions. As weight management generally involves addressing multiple behaviors, we chose to ask about weight management and specific health behaviors separately. The survey is appended.
Data Collection
Surveys were sent via an Internet data survey tool (Qualtrics) to both the primary contact (generally either the practice manager or director of behavioral health) and the BHP(s) at the 248 practices involved in SIM that had an integrated BHP at the completion of the project (out of the 319 practices that completed the project). For some practices, we only had contact information for a person other than the BHP; they were asked to forward the survey to the BHP rather than complete the survey themselves. If there were multiple BHPs at the practice, each was encouraged to complete the survey separately. We sent an initial email message inviting participation (N = 300 practice contacts), followed by up to 3 email reminders. Participants were not compensated. Data were collected between September and November 2019.
Statistical Analysis
Descriptive statistics (frequency distributions, proportions, means, SDs) were used to summarize results. Bivariate associations between semi-continuous (ordinal) or continuous variables were examined using Spearman’s correlations. Bivariate associations between continuous or semi-continuous (ordinal) and dichotomous variables were assessed using Kendall’s tau. All analyzes were performed using SAS 9.4 (Cary, NC).
Results
From the 248 potential practice sites, 79 BHPs from 64 unique practices completed the survey (26% practice response rate). Unfortunately, it is not known how many practice contacts forwarded the survey invitation to BHPs working at the practice and consequently how many did not answer the survey. Characteristics of the practices of the BHPs who responded are displayed in Table 1.
Practice Characteristics Total N = 64.

Respondent Characteristics
Respondents primarily identified as female (81%) and white (77%) and the majority had been practicing as a BHP in their current location for fewer than 5 years. Almost half were Licensed Clinical Social Workers. Most worked full-time, were employed rather than independent contractors, and saw an average of 19.9 patients per week. Respondent characteristics are displayed in Table 2.
Respondent Characteristics Total N = 79.

Mental Health and Health Behavior Issues BHPs Report Addressing With Patients
Respondents reported seeing patients for a broad range of mental health diagnoses with varying frequency. Figure 1 depicts frequency of referrals for common mental health diagnoses.

Reported frequency of patients referred or treated, categorized by diagnosis: mental health.
Only 32.9% of respondents indicated that the majority of their time as a BHP is spent addressing mental health issues rather than behavior change and reported commonly receiving referrals for health behavior issues. They reported the most referrals for health behavior related concerns for stress management, followed by sleep concerns, and diet change (see Figure 2).

Reported frequency of patients referred or treated, categorized by diagnosis: health behavior.
However, BHPs often reported identifying and addressing both mental health diagnoses and health related behavior and weight management issues with patients who were referred for other concerns or diagnoses (see both Figures 1 and 2).
Techniques and Approaches BHPs Use With Patients
In response to the question that presented 12 techniques with directions to select “yes” next to those used in situations when helping patients with mental health issues, nearly all respondents endorsed cognitive behavioral therapy, mindfulness, and relaxation/stress management. Solution-focused therapy and motivational interviewing were close behind, with group endorsement rates of 90% or more for each. For treatments involving health behavior changes, BHPs reported almost unanimous endorsement of mindfulness, motivational interviewing (MI), and relaxation technique items (see Figure 3).
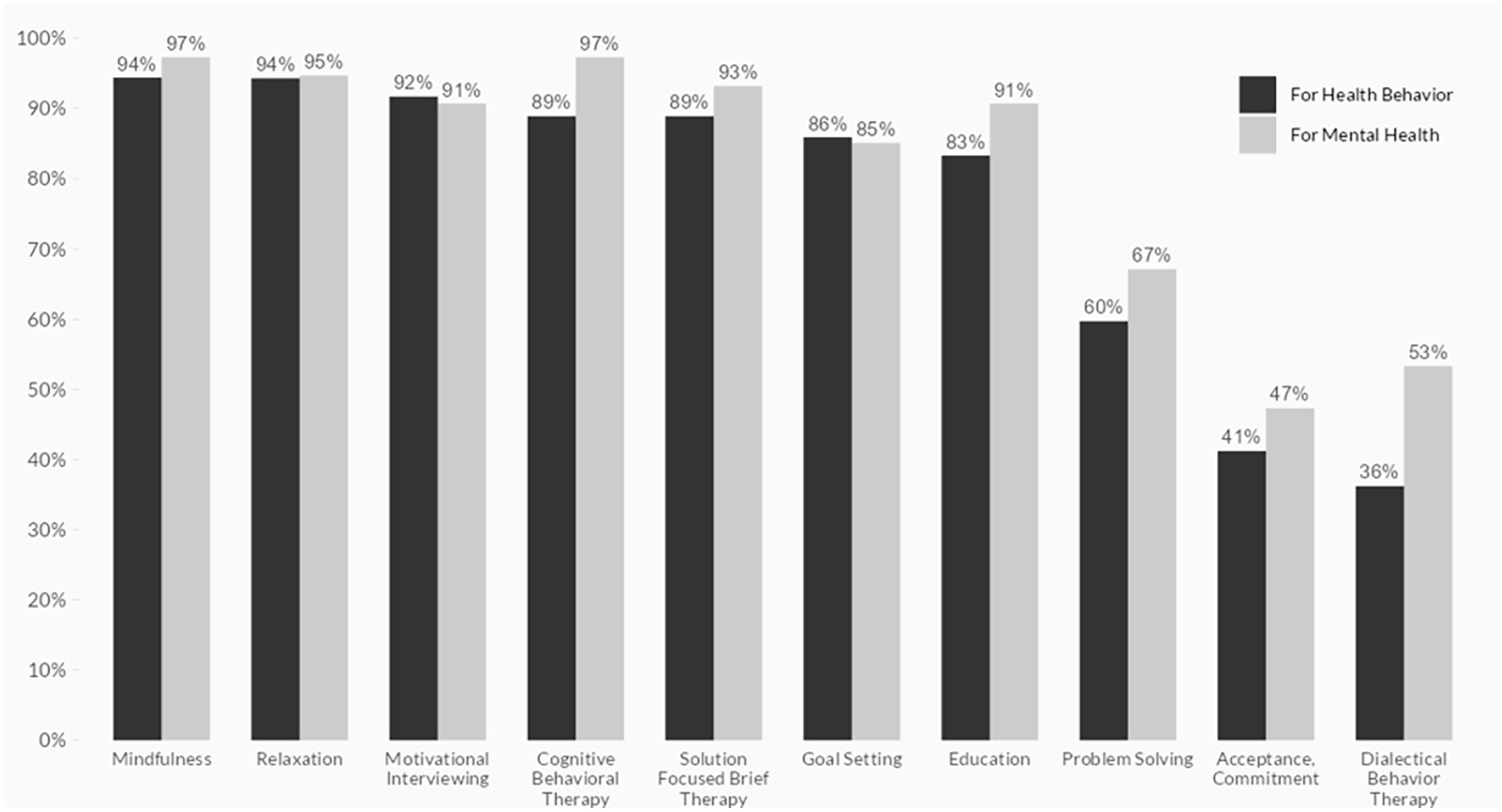
Reported frequency of use of specific techniques for mental health and health behavior.
An open-ended response item asking which they found most effective for mental health diagnoses immediately followed. The top responses were cognitive behavioral therapy (CBT), mindfulness, and solution focused brief therapy (SFBT). Respondents were then asked in another open-ended item to submit techniques they consider most effective when managing health behavior in general and also specifically for weight management. The top responses for health behavior in general were CBT, MI, and SFBT. Specific to weight management, MI was reported as the most effective most frequently, followed by goal setting, and CBT. The 5 most frequent responses for mental health diagnoses, health behavior, and weight management are displayed in Figure 4.

Top 5 techniques considered most effective for mental health, health behaviors, and weight management.
When asked whether they work with patients around weight management, 65% of BHPs (48 of 74) answered positively. Of the 26 who were not, 57% (15) expressed either definite or possible interest in providing this type of care.
***Associations between 2 ordinal or semi-continuous variables were assessed using Spearman’s correlation coefficients (n = 74 to n = 76 for all correlations). Time in practice overall (not just in their current job) was also associated with receiving more referrals for weight management (rho = .271, P = .018) and with addressing diet (rho = .339, P = .003) and weight management (rho = .324, P = .005), regardless of referral reason. Regarding what BHPs treat beyond referrals, seeing more patients per week was associated with more frequent reports of addressing diet (rho = .233, P = .046) and weight management (rho = .233, P = .046). BHPs in practices that had care managers were more likely to report receiving referrals for weight management than BHPs in practices that did not employ a care manager (
Discussion
Our findings offer new insight into how BHPs integrated in primary care settings are currently supporting patients with behavior change and their interest in providing these services. BHPs in this sample primarily receive referrals to treat patients for traditional mental health diagnoses such as anxiety and depression, but spend a significant amount of time addressing behavior change. In fact, in this sample, the majority of BHPs report NOT spending most of their time addressing traditional mental health diagnoses, conflicting with other literature.10-12 BHPs report that they identify and address health behavior change issues with patients, as health behavior issues often arise while treating patients for a mental health related referral. The BHPs in this study reported using the same treatment approaches to address both mental and health behavior issues, although they more frequently identified using MI and goal setting for behavior change and weight management and believe these techniques are the most effective for these concerns.
We also learned that BHPs who had been in practice longer were more likely to address weight management and diet change with patients. We speculate that increased time in practice and additional training and competency development leads to more comfort with a wide range of treatment areas. In addition, BHPs who worked in practices with care managers were more likely to receive referrals for weight management, while those working in practices employing a health coach were more likely to receive referrals for physical activity support; possibly related to care being provided by a more diverse team that is able to identify additional ways in which BHPs could help patients. The literature suggests that team approaches to weight management in primary care are more effective than those delivered by individual providers,26,27 and perhaps this finding demonstrates that teams are also more able to identify the need for behavioral interventions and refer to other team members for care. When such individuals are employed by the practice, it could also indicate a practice environment supportive of addressing a wide variety of health behavior and behavior related health issues such as obesity.
Our findings also lead to reflection on whether PCPs recognize the support BHPs can provide for patients around health behavior change. PCPs face multiple barriers in addressing health behavior change themselves with patients, including insufficient time, 28 lack of familiarity with or skills in behavior change interventions, 29 practice structural barriers,30,31 or lack of reimbursement. 32 In addition, evidence supports that PCPs often miss opportunities for behavior change counseling 33 and may believe that mental health diagnoses take precedence over behavior change. Our results indicate that even though BHPs do not receive as many referrals from PCPs for the primary issues of behavior change, BHPs often identify these issues while evaluating other diagnoses and work with patients around management. However, there are likely many missed opportunities to address such behavioral issues in the broader group of patients not referred initially for mental health issues.
While this survey was not designed to investigate patient outcomes, the literature suggests through clinical studies on behavior change interventions that involvement of a BHP in health behavior change leads to improved outcomes.6,8,13 Specific to weight management, given the prevalence of obesity and the resulting effects on health outcomes, extensive effort and funding have been put into developing more effective approaches to behavior change including weight management in primary care. Indeed, guidelines recommend that PCPs identify obesity and offer evidence-based treatments, including intensive behavioral therapy, to patients with obesity. 34 However, based on the literature, it appears this happens infrequently. 35 What can be done to increase BHP involvement in health behavior change is an area for future exploration and intervention, particularly around increasing PCPs’ understanding of the support and treatment BHPs can offer patients. Our results show that BHPs recognize that they can provide support for patients around behavior change. Determining how to increase their interactions with patients in this area is an important next step. For example, educating PCPs about the impact of BHP involvement on health behavior could provide new opportunities for supporting health behavior related change, especially for patients who otherwise would not have access to behavioral health care for geographic or economic reasons.
There are several limitations to this work. The response rate and sample size are small. Related to this, these results are reported only from practices in Colorado that participated in a project related to improving behavioral health care. Thus, the results are highly biased toward practices interested in this topic. Also, we did not receive responses from all the practices surveyed and do not know if this was due to the practice having lost their BHP, a BHP not receiving the survey, or the BHP not responding. Also, the questions in this survey were not validated nor tested for reliability; thus, the responses produced may, or may not represent the true intent of the questions.
Conclusion
This study indicates that BHPs in integrated primary care settings identify the need for interventions around health behavior, often supporting behavior change in patients despite PCPs not always recognizing this need and importantly, that they are interested in this work. This finding may open up opportunities for more health behavior change interventions in practice as integrated behavioral health becomes more prevalent. Patients thus are likely to benefit from having access to behavior change-trained professionals to address these issues, which may prevent or address chronic health conditions so prevalent in primary care. Primary care behavioral health integration has increased access. Developing feasible pathways and increasing provider awareness of what BHPs can do may improve weight management in primary care. More research about the potential of expanding the role of BHPs to address health behavior issues in this setting may lead to improved integration of BHPs into chronic care management and ultimately, improved patient outcomes.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319231172039 – Supplemental material for Integrated Primary Care and Health Behavior Support: A Survey of Behavioral Health Providers
Supplemental material, sj-docx-1-jpc-10.1177_21501319231172039 for Integrated Primary Care and Health Behavior Support: A Survey of Behavioral Health Providers by Andrea Nederveld, Kimberly Wiggins, Linda Miriam Dickinson, Perry W Dickinson, Lauren Woodward Tolle and Jodi Summers Holtrop in Journal of Primary Care & Community Health
Footnotes
Author Contributions
We would like to thank Dr. Kyle Knierim, Ms. Lauren Shviraga, and Ms. Dionisia De La Cerda for their support in developing, administering and analyzing the survey.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported in part by a cooperative agreement from the U.S Department of Health and Human Services, Center for Medicare & Medicaid Innovation—Funding Opportunity Number CMS-1G1-14-001.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.