
Abstract
Introduction:
Integrated Behavioral Health (IBH) clinics in primary care offer cost-effective options for receiving mental health (MH) support for Black patients. By tracking specific aspects of social determinants of health (SDOH), more commonly assessed in primary care, IBH programs can provide helpful insights to both MH and primary care providers.
Methods:
This retrospective study examined the impact of IBH care delivery on MH and social needs variables in a Black adult patient population. MH outcomes were assessed using the PHQ9 and GAD7, with a positive score being greater than 5.
Results:
There were N = 119 Black patients included in analysis. The sample was 83% female and the average age at first visit was 41. There was a significant reduction in both GAD7 (change = −1.8, P < .001) and PHQ9 (change = −2.3, P < .001) scores for patients receiving IBH services. There were no significant differences between those who had a SDOH screen and having an initial elevated GAD7/PHQ9 score.
Conclusion:
More culturally inclusive research on the impact of IBH implementation where Black patients receive their primary care is needed to maximize treatment possibilities among this group.
Introduction
Integrated Behavioral Health (IBH) programs in primary care have offered cost-effective options for receiving mental health support for Black adults in the US.1,2 IBH, in this context, occurs when patients are able to receive care for their mental health, psychosocial health, life stress, and primary care from a practice team of mental health specialists and primary care doctors. 3 While many minoritized groups experience a high prevalence of unmet outpatient mental health needs, Black adults in the US are impacted to a greater extent.4,5 IBH programs offer viable solutions to improve support, improve access to mental health professionals, and reduce the costs of accessing the health care system. 6 These programs have been associated with shorter treatment wait-times, higher likelihood of treatment engagement, and more visits attended by patients. 7
In general, mental health outcomes improve significantly for all racial and ethnic groups when mental treatment is initiated in primary care 16 ; however, mental health care utilization among Black adults is much lower than that of their White counterparts, and barriers to care for these individuals may include financial, geographic, cultural, and linguistic obstacles.8,9 IBH programs may provide effective ways to navigate these obstacles for racial and ethnic minority groups.10,11 Although there is limited research on mental health outcomes specifically for Black patients in IBH programs, supporting literature calls for leveraging integrated care as a priority objective for meeting mental health needs of underserved groups.1,12 Black patients consistently report trusting their primary care doctors with their mental health concerns more than any other clinician.1,13,14 Furthermore, in a randomized controlled trial comparing collaborative care (a form of IBH) to usual care that included Black adults, patients in the collaborative care group had a more significant reduction in Patient Health Questionnaire-9 (PHQ-9) scores compared to those in the usual care group. 15 Over 60% of the US population will initiate mental health care through primary care settings, making accessibility a high priority when addressing mental health and health disparities.17,18 Within some IBH practices, patients are able to access interventions for acute mental health concerns on the same day of a medical visit or receive collaborative support from an interdisciplinary team over time. 1 Having the opportunity to receive behavioral health care within one’s primary practice has been shown to decrease stigma surrounding mental health treatment. 6 Given that mental health stigma has been reported as higher in Black communities, 19 IBH programs can offer de-stigmatizing support with trusted providers even though treatment may be of a briefer duration than other mental health models.7,16 Patients may be more likely to seek IBH services because of established rapport with their treatment team and comfort within their environment, which also reduces the need to pursue specialty behavioral health services.6,20
Mental Health Disparities for Black Adults
Mental health concerns among Black patients are significant and multifaceted; influenced by unique factors like racism, racial discrimination, and systemic oppression which play a role in those outcomes.21 -23 Some research suggests, that despite greater exposure to stress, material hardship, and disparate physical health outcomes, Black Americans report similar or lower rates of psychiatric disorders than White Americans. 24 Access to community resources, different coping skills, and other environmental supports have been thought to buffer mental health among Black adults leading to lower rates of psychiatric disorders.25 -28 However, critical factors such as access to care as well as the likelihood to seek quality mental health care may underpin the lower rate of mental health disorders diagnosed among Black adults compared to their White counterparts.29,30 For example, Black patients are more likely to reside in underserved communities with fewer behavioral health clinicians available to provide care to such large groups with unmet needs.1,31,32 Additionally, minoritized patients are less likely to be referred for services even if they explicitly mention concerns.1,33 As such, Black patients are less likely to seek depression treatment compared to their White counterparts, a trend that is attributed to access barriers and structural and contextual factors like access, health literacy, and socioeconomic barriers.1,34,35 For individuals who do seek treatment, racial and ethnic minorities are 40-80% more likely to prematurely end care.36,37
Social Determinants of Health, Social Needs, and Mental Health Outcomes
In addition to mental health access, examining the specific impact of social determinants of health (SDOH) for Black patients is important to consider when discussing mental health outcomes. SDOH are categorized into 5 domains spanning economic stability, educational attainment, health care, neighborhood and environment, and social and community contexts and comprise the variety of conditions that people experience across their lifespan that affect their health outcomes. 38 Each domain contains a multitude of risk and protective factors impacting access to healthy foods, secure employment, and safe housing. 39 The impact of SDOH manifest as social needs like housing stability, financial needs, and employment. 40 These social needs can lead to heightened levels of distress and can negatively impact the physical health of Black patients.39,41,42 Things like weathering for Black women, heightened allostatic load for Black adults, and generational discrimination contribute to the unique levels of cumulative stress experienced by this group.43 -45
Research has established that social needs concerns that are influenced by SDOH disparities are associated with elevated risk of mental health disorders. 40 Black Americans experience institutional racism across each of the SDOH domains, further exacerbating their risk of psychological distress.42,45,46 Higher education or income do not remove the sting of racism and discrimination for Black adults given that they may experience worse mental health and may be less likely to seek treatment due to perceived discrimination and stigma.21,47
Social needs and mental health outcomes are intricately intertwined. Given that social needs are most often evaluated in primary care, IBH programs have unique positioning to assess biopsychosocial and cultural aspects of mental health and physical health. Overall, there is a significant gap in the literature with regards to the exploration of mental health and social determinants of health for Black patients being seen in IBH programs in primary care. Furthermore, less is known about the intersections of mental health outcomes and social needs for Black adults seeking support in this type of environment. The primary aim of this study was to explore the association between anxiety and depression outcomes and social determinants of health screening in a predominantly Black primary care patient population. The study hypotheses are that participation in IBH services within primary care reduces anxiety and depression symptom reporting and that reduced anxiety and depression symptom reporting is associated with reduced social needs concerns.
Methods
Study participants consisted of adult therapy patients who were seen by primary care behavioral health specialists between July of 2022 and December of 2024, at a large primary care clinic on the east coast. Institutional Review Board approval at Medstar Georgetown University Hospital was obtained. The quasi-experimental design using retroactive review of the hospital electronic medical record (EMR) accessed standard of care metrics for patients enrolled in IBH services. Patients were enrolled into the IBH program via an internal referral from a practice primary care provider (PCP). PCPs at this practice include medical residents and attending physicians. IBH providers included a Black licensed psychologist, a Black psychiatrist, 3 Black graduate level psychology trainees, and 1 white graduate trainee.
Demographic characteristics of age at first visit (years) and sex (female, male) were collected. Whether the patient was screened for social needs or social history and whether the screening was positive was recorded. Within this primary care practice, mental health screeners were provided regularly during active IBH brief psychotherapy treatment; however, for the purposes of this study, the initial and last-screened anxiety and depression outcomes while patients were receiving IBH care were examined. Additionally, a hospital SDOH/social needs screener was administered. Patients enrolled in the IBH program received social needs screening either at annual wellness visits or during other contact points with IBH staff.
Measures
Anxiety, depression, and social determinants of health via social needs were assessed as patient outcomes. For each outcome, patients who had at least 1 initial and 1 follow-up anxiety and/or depression screening score that was between 5 days and 8 months apart were included in the analysis. Timing was chosen to be consistent with treatment time ranges for brief primary care mental health offerings for adults.48 -50
Generalized Anxiety Disorder
Generalized Anxiety Disorder—7 (GAD-7)
The GAD-7 is a brief, 7-item self-report scale designed to identify likely cases of generalized anxiety disorder (GAD). The GAD-7 assesses anxiety symptoms with scores ranging from zero to twenty-one with a score of ≥10 indicating moderate to severe anxiety. It was originally validated in a primary care sample, which yielded a specificity value of 0.82 in determining generalized anxiety disorder.51,52
Depression
Patient Health Questionnaire—9 (PHQ-9)
The PHQ-9 is a self-administered version of the PRIME-MD diagnostic instrument for common mental health disorders with the PHQ-9 being the scale’s 9-item depression module. 53 PHQ-9 scores range from 0 to 27 with a PHQ-9 score ≥ 10 indicating moderate to severe depression. It has been found to be a reliable (α = .89) measure of depression severity, with a sensitivity and specificity of 88% for major depression. 53
Social Determinants of Health
Social Needs Screener
The social needs screener is a modified version of the Protocol for Responding to and Assessing Patients’ Assets, Risks, and Experiences (PRAPARE) tool which is a comprehensive assessment tool designed to assess patients’ social determinants of health.54,55 The measure was created, standardized, implemented, and promoted by the National Association of Community Health Centers (NACHC), the Association of Asian Pacific Community Health Organizations (AAPCHO), the Oregon Primary Care Association (OPCA), and the Institute for Alternative Futures. PRAPARE is both a standardized patient social risk assessment tool consisting of a set of national core measures and addresses the social determinants at both the patient and population levels. 56 The original PRAPARE tool includes 21 questions categorized into 4 domains: personal characteristics, family and home, money and resources, and social and emotional health.
A modified version of the PRAPARE tool was implemented across the hospital system to address the predominant needs of the medical population served. Within the 4 domains, the hospital system prioritized the Money and Resources sub-domains for social needs screening given the significant associations of these factors across the hospital system. The primary question, “In the past 12 months, has it been hard for you to get food, housing, transportation, utilities, medical care, or employment?” was followed by 8 additional questions (see Table 1). For this study, a “Yes” response to any of these questions constituted a positive social needs screen. Systematic screening for social needs within this health system was started during the study period and was not widely adopted by the time of data collection. Therefore, patient charts were also reviewed focusing on relevant social history during their treatment period. Emphasis areas for collection were those that aligned with the PRAPARE questions, including reporting of issues with living arrangements, financial concerns, need for special services and community resources aimed at addressing food insecurity and transportation issues. The social history section is completed by any treating provider in the hospital system at the point of intake or follow up. Special attention was paid to the mental health screening timeframes that aligned with the social history entries into the EMR.
PREPARE Tool Modification: Social Needs Screening Questions.

Analytic Strategy
Patient characteristics were summarized using frequencies and percentages for categorical variables and using means and standard deviations for continuous variables. Paired t-tests were used to test the change in each score between patients’ first and last visits. Logistic regression models were used to test the association of screening for social needs/social history (not screened, screened negative, screened positive) and initially having a mild or moderate to severe mental health outcome. Odds ratios (OR), 95% confidence intervals (CI), and p-values were reported from the models. An alpha level of 0.05 was used for all tests. All analyses were performed in R version 4.3.1.
Results
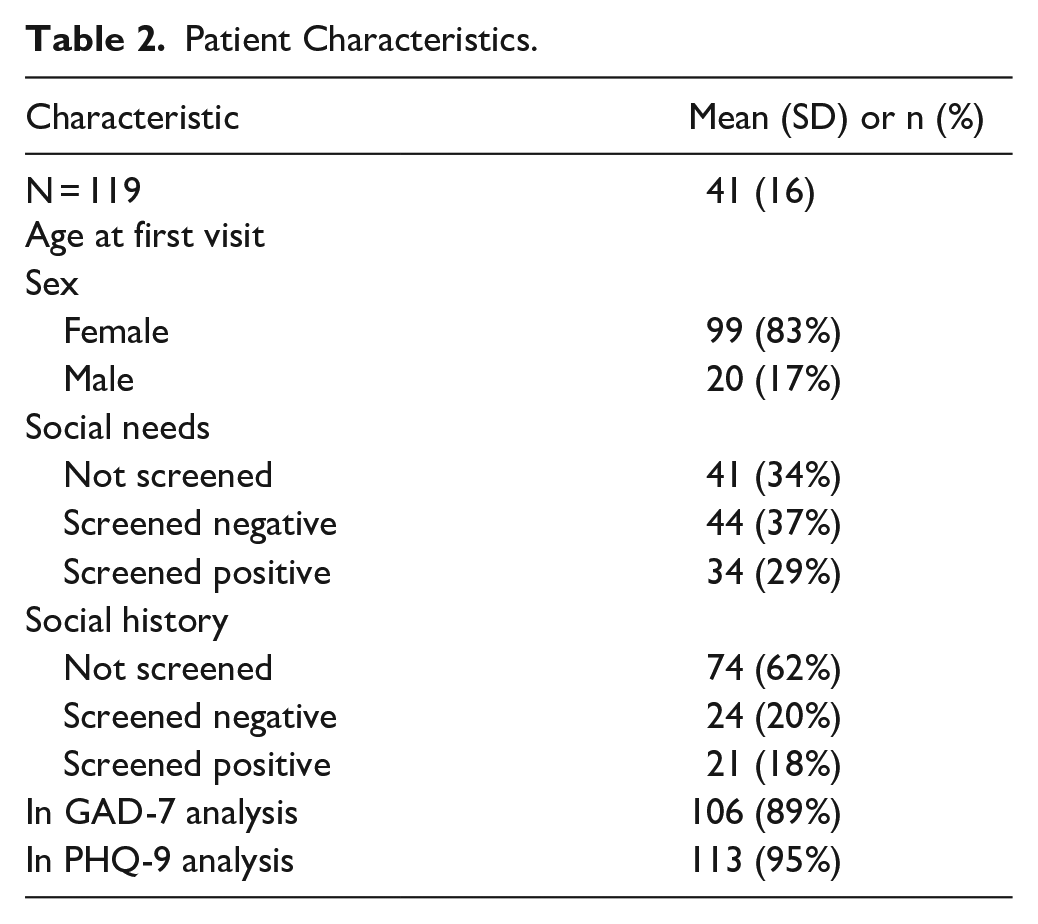
Table 2 shows patient characteristics for N = 119 Black adult patients. The average age at first visit in the sample was 41 (SD = 16) years old. Overall, 83% were female. Forty-one patients (34%) were not screened for social needs, 44 (37%) screened negative, and 34 (29%) screened positive. At the time of assessment, 74 patients (62%) had not been screened for social history, 24 (20%) screened negative, and 21 (18%) screened positive.
Patient Characteristics.
GAD-7 Outcomes
There were N = 106 patients who had GAD-7 scores at least 5 days apart and within 8 months (243 days). Average visit count was 4 (SD = 2) visits with 101 (SD = 79) days between their first and last visits. Patients had an average GAD-7 score of 10.3 (SD = 5.7) at their first visit and 8.5 (SD = 6.0) at their last visit (Table 3). The average change in scores from first to last visit was −1.8 points, (95% CI [-2.9, -0.8]). IBH patients’ GAD-7 scores were significantly lower at their last visit compared to their first visit (t[105] = −3.50, P < .001, d = −0.34).
Visit Characteristics for Patients With Pre/post GAD-7 and PHQ9 Scores at Least 5 days Apart and Within 8 Months.

There was not a significant difference in the odds of having an initial GAD-7 score ≥ 5 for those who screened negative for social needs compared to those who were not screened (OR = 1.03, 95% CI [0.32, 3.22], P > 0.9). Additionally, there was not a significant difference in the odds of having an initial GAD-7 score ≥ 5 for those who screened positive for social needs compared to those who were not screened (OR = 1.00, 95% CI [0.29, 3.50], P > .9; Table 4).
Logistic Regression Models for Social Needs and Social History Outcomes by GAD-7 and PHQ-9 Scores.

Similarly, there was not a significant difference in the odds of having an initial GAD-7 score ≥ 10 for those who screened negative for social needs compared to those who were not screened (OR = 0.59, 95% CI [0.23, 1.45], P = .3), or for those who screened positive for social needs compared to those who were not screened (OR = 0.75, 95% CI [0.28, 2.00], P = .6) (Table 4).
There was not a significant difference in the odds of having an initial GAD-7 score ≥ 5 for those who screened negative for social history compared to those who were not screened (OR = 0.96, 95% CI [0.29, 3.78], P > .9). Additionally, there was not a significant difference in the odds of having an initial GAD-7 score ≥ 5 for those who screened positive for social history compared to those who were not screened (OR = 0.90, 95% CI [0.27, 3.56], P = .9; Table 4).
Similarly, there was not a significant difference in the odds of having an initial GAD-7 score ≥ 10 for those who screened negative for social history compared to those who were not screened (OR = 1.34, 95% CI [0.49, 3.72], P = .6), or for those who screened positive compared to those who were not screened (OR = 1.22, 95% CI [0.44, 3.43], P = .7; Table 4).
PHQ-9 Outcomes
There were N = 113 patients who had PHQ-9 scores at least 5 days apart and within 8 months (243 days). Average visit count was 4 (SD = 2) visits with 104 (SD = 78) days between their first and last visits. For depression screenings, patients had an average PHQ-9 score of 11.4 (SD = 6.1) at their first visit and 9.1 (SD = 6.5) at their last visit. The average change in scores from first to last visit was −2.3 points, (95% CI [−3.4, −1.1]). Therapy patients’ PHQ-9 scores were significantly lower at their last visit compared to their first visit (t[112] = −3.92, P < .001, d = −0.37).
There was not a significant difference in the odds of having an initial PHQ-9 score ≥ 5 for those who screened negative for social needs compared to those who were not screened (OR = 1.68, 95% CI [0.44, 7.07], P = .5). Additionally, there was not a significant difference in the odds of having an initial PHQ-9 score ≥ 5 for those who screened positive for social needs compared to those who were not screened (OR = 0.57, 95% CI [0.17, 1.84], P = .3).
There was not a significant difference in the odds of having an initial PHQ-9 score ≥10 for those who screened negative for social needs compared to those who were not screened (OR = 1.51, 95% CI [0.60, 3.89], P = .4), or for those who screened positive for social needs compared to those who were not screened (OR = 0.59, 95% CI [0.23, 1.50], P = .3; Table 4).
Similarly, there was not a significant difference in the odds of having an initial PHQ-9 score ≥ 5 for those who screened negative for social history compared to those who were not screened (OR = 0.63, 95% CI [0.20, 2.24], P = .5). Additionally, there was not a significant difference in the odds of having an initial PHQ-9 score ≥ 5 for those who screened positive for social history compared to those who were not screened (OR = 1.77, 95% CI [0.43, 12.1], P = .5; Table 4).
Lastly, there was not a significant difference in the odds of having an initial PHQ-9 score ≥ 10 for those who screened negative for social history compared to those who were not screened (OR = 0.85, 95% CI [0.32, 2.33], P = .8), or for those who screened positive for social history compared to those who were not screened (OR = 0.79, 95% CI [0.29, 2.17], P = .6).
Discussion
Integrated behavioral health programs may be an effective approach to improve mental health outcomes for Black adult primary care patients. Supporting the primary hypothesis, after participating in the IBH program, patients experienced significant reductions in symptoms of both anxiety and depression as measured by the GAD-7 and PHQ-9. Importantly, these improvements were seen within an average of only 4 visits with a mental health care provider over the course of about 3 months. These findings support prior research that IBH programs may be an effective way to address access to gaps in mental healthcare for Black adults and improve mental health outcomes among this group. Additionally, these programs can be cost-effective strategies by providing individualized and targeted therapy, which can be accomplished in briefer time frames than traditional outpatient psychotherapy.57,58
Significant decline in both GAD7 and PHQ-9 scores may have been a result of several different factors, including access to mental health treatment within a short timeframe once a concern was identified by a PCP, familiarity with the health care system where their primary care was supported, and cultural relevance of the intervention approaches. It is important to note that 5 out of 6 IBH providers identified as Black and the White graduate trainee was supervised by a Black supervisor who met with all patients during treatment. Research has shown that therapy matching has benefits for Black patients, 31 and it is possible that patients felt comfortable engaging in treatment given that the providers and the treatment was representative and inclusive of their lived identities. Given that stress, depression, or anxiety may present differently among Black patients than in other race/ethnicity groups, it can be challenging for Black patients to identify with some diagnostic mental health symptoms or for providers to accurately assess what these patients are communicating.31,59 -61 For example, providers are less likely to detect depression and administer culturally adapted treatment for Black women and instead have mistaken depression for other serious mental illnesses.36,62 -64 Given these reasons, some Black families may prioritize managing mental health symptoms without professional help via familial and community support.65,70 Leveraging inclusivity in IBH settings may provide unique opportunities to reach Black patients in settings where they feel most comfortable.
Additionally, Black patients may feel more comfortable in spaces where they feel seen and supported, which can be influenced by patient-provider race matching or being treated by non-White providers.66-68 Of the roughly 28 PCPs (17 residents, 11 attendings) who referred patients to IBH services over the study period, 23 identified as Black, Hispanic, Asian-American, or Middle-Eastern American. Enhancement of culturally relevant care has also been shown to improve outcomes for Black patients in medical settings. 69 In the current study, the entire physician team is routinely trained on culturally relevant primary care service delivery, which may have also increased the likelihood of treatment buy-in at the time of the referral; therefore, potentially increasing the likelihood and success of IBH treatment.
Furthermore, among this group of patients, roughly 29% screened positive for social needs and 18% screened positive for social history, suggesting that social determinants of health affect a large portion of this population. Although no significant differences in depression or anxiety symptoms were observed between those screening positive and those screening negative for both social needs and social history, this may suggest that the services provided focused more on general mental health rather than the social needs that impact mental health overall. Higher levels of social need may not have increased the likelihood of an individual seeking or being linked to care from the IBH team. However, given the prevalence of social needs among this group, which are linked to worse health outcomes, this further supports prior research for the need for standardized social needs screening for primary care patients. 71
Examining anxiety, depression, and social needs outcomes specifically for Black patients in a primary care setting supports existing research around the benefits of IBH programs for this group.17,18 However, this study was not without limitation. Small sample size may have impacted the data outcomes and future generalizability. Additionally, not having a control group limits overall conclusions about the impact of the intervention. Findings from this study may not generalize to other mental health settings outside of integrated behavioral health in primary care.
Assessing a newly administered social needs screening among IBH patients may have limited SDOH results on the current sample of patients. Future iterations of this study will proceed with more robust social needs data and comparative analyses in relation to mental health outcomes. Furthermore, the modified PRAPARE tool may not have fully captured additional social needs that may have been more closely associated with individual mental health outcomes (e.g., social and emotional domain). In addition to the small sample size, not collecting the social and emotional domain may have rendered the modified PRAPARE tool ineffective in the current study.
Conclusion
Overall, this study sought to provide critical evidence for the need for IBH programs in areas with a high concentration of mental health need for Black communities. The significant reduction in mental health symptoms over a short duration may support the need for more IBH programs in predominantly Black communities. Future studies looking to enhance IBH services for Black patients should focus on appropriate social needs screening. Additionally, randomized trials that include mental and physical health comparisons between patients in primary care who received IBH services and those who did not would address gaps in IBH care delivery for Black adults. Lastly, comparison of standardized IBH programs across sites would further inform the necessity of offering and funding IBH programs in areas of greatest biological, psychological, and social need for Black adults.
Footnotes
Acknowledgements
We would like to acknowledge Dr. Aronica Cotton, Dr. Flavia DeSouza, Dr. Nina Axiotakis, and the many residents, attendings, and staff who all made immeasurable contributions to the lives of our patients.
Authors’ Note
Ms. Splain, Mr. Daniel, and Ms. Warren began research with this project as graduate trainees at MGUH while attending their home institutions.
Ethical Considerations
Institutional Review Board Approval was obtained through MedStar Health Research Institute # STUDY00004187.
Consent to Participate
This is an IRB-approved retrospective study, all patient information was de-identified and patient consent was not required. Patient data will not be shared with third parties.
Consent for Publication
Not applicable.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the A. James & Alice B. Clark Foundation as part of DC Safe Babies, Safe Moms.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets analyzed during the current study are available from the corresponding author on reasonable request and require additional permission from Medstar Health Research Institute.