
Abstract
Introduction:
Atrial Fibrillation (AF) is common in older adults, yet guideline-recommended oral anti-coagulants (OACs) for stroke prevention are underused in this population. With a growing population of older adults at risk of AF seeking primary care, the objective of the study was to determine the management practices and perspectives of family physicians on the initiation of OACs for stroke prevention in AF patients 75 years or older, including their engagement of patients in shared decision-making.
Methods:
This was an online survey of family physicians affiliated with a Primary Care Network in Alberta, Canada.
Results:
Patient’s risk (of falls, bleeding, or stroke) was the most common factor (17/20, 85%) physicians considered when deciding to initiate OAC in older adult patients with AF. Physicians used the CHADS2VASC (13/14, 93%) and HASBLED (11/15, 73%) tools to determine stroke and bleeding risks, respectively. Majority (11/15, 73%) of the physicians agreed that they feel confident initiating OAC for AF patients ≥75, while 20% (3/15) were neutral. All physicians agreed that their patients participated in shared decision-making to initiate OAC for stroke prevention.
Conclusion:
Family physicians strongly consider patient risks and utilize risk-assessment tools when initiating OAC in older adults with AF. Despite all physicians reporting the use of shared decision-making and that their patients were educated on the indications for OAC, confidence in initiating treatment was variable. Further exploration into factors impacting physician confidence is needed.
Introduction
Worldwide, atrial fibrillation (AF) affects over 33 million people and is considered the most common type of cardiac arrhythmia. 1 Advancing age is associated with higher rates of AF with incidence and prevalence rates of almost 10% in those over the age of 80. 2 Moreover, these rates are expected to rise globally due to a growing aging population and longer life expectancies. 3 Within the Canadian context, it is estimated that 200 000 Canadians are living with AF, 4 and majority of these patients are managed within their primary care clinics.
The risks of AF are well-documented and significantly impact quality of life. Patients with AF have a 5-fold increase in the risk of ischemic stroke,2,5 as well as an increased risk of congestive heart failure, hospitalization, and mortality. 6 Not only do older adult patients experience significantly worse health outcomes following AF-associated ischemic strokes, but they are more likely to be bedridden, chronically disabled, or require constant nursing care. 7 The heightened risk of ischemic stroke, coupled with functional impairments that threaten independence, highlights the importance of appropriate management of AF in this high-risk population.
The use of oral anticoagulants (OACs) for stroke prevention is a critical therapeutic intervention in the management of AF.8,9 The benefit of administering OACs for stroke prevention, however, must be weighed against the risk of bleeding. 10 With OACs, the annual risk of stroke decreases from 2.1% to 0.7% in patients, while the risk of major bleeding increases from 0.5% to 1.0% in patients 65 years of age or older. 10 While Canadian and international guidelines suggest that most patients with AF benefit from anticoagulation for stroke prevention, these guidelines affirm that patient values and use of shared decision-making be strongly considered.6,9 Clinical tools, such as the CHAD-65 or CHADS2VASC score and the HASBLED score, are readily available to guide clinicians to weigh patient risks of stroke versus risks of major bleeding, respectively.
The decision to initiate OACs in an older adult patient is further complicated by the increased likelihood of frailty and geriatric syndromes, including dementia, falls, co-morbid medical conditions, and polypharmacy. 8 Frailty is a state of vulnerability that confers a heightened risk of adverse outcomes, and there is a growing recognition of a relationship of frailty with cardiovascular disease, including atrial fibrillation. 11 Furthermore, many clinical trials exclude patients over the age of 75, which may limit the applicability of these clinical guidelines. This creates therapeutic uncertainty for many clinicians to initiate OACs in this high-risk group of patients (older adults 75 years of age or older) despite their significantly higher incidence of stroke, systemic thromboembolism, and death compared to younger patients with AF. 12
Contrary to the recommendation of clinical practice guidelines, anticoagulants remain widely underused among eligible patients, that would otherwise benefit from OAC therapy.11,13,14 A systematic review of current treatment practices for stroke prevention in AF revealed that current practice did not align with published treatment guidelines with many studies reporting that less than 60% of high-risk patients receive treatment.13,15 The impact of this anticoagulant underuse in AF includes higher rates of preventable ischemic stroke, morbidity, and health and social care costs. 11
Given the burden of AF and the challenges of making risk-benefit analyses in the older adult patient, pragmatic understanding of the decision-making process by frontline providers on OAC initiation is needed. Acknowledging that approximately 85% of anticoagulant therapies are prescribed by family physicians, and their longitudinal doctor-patient relationships make them ideal for delivering patient-centered approaches to stroke prevention in AF,14,16 the management practices and perspectives of family physicians are of particular interest. Further, this will enable exploration of a key facet of patient-centered care known as shared decision-making (SDM), that has shown value in situations where the benefit-to-harm risks are subtle, 17 such as in stroke prevention in older patients with AF. SDM involves collaboration between clinicians and patients to make decisions that are both informed by evidence, and in line with the patients’ values. 18
The objective of this study was to determine the management practices and perspectives of family physicians on their decision-making process, including their engagement with patients in SDM, on the initiation of OACs in patients 75 years of age or older with AF.
Methods
This was an online survey conducted on a purposive sample of family physicians. We selected family physicians affiliated with the Edmonton O-day’min Primary Care Network (EOPCN), previously known as Edmonton Oliver PCN. Primary Care Networks were established in Alberta in 2005 and are composed of multiple family practices that work in collaboration with allied health teams to optimize primary care. The EOPCN is recognized to serve some of the most vulnerable geriatric patients and has a dedicated senior’s program, with supports from nursing and pharmacists. Family physicians affiliated with the EOPCN thus were felt to have greater experience caring for older adult patients and potentially initiating OACs; as well as being positioned in a team-based model of care potentially more amenable to implement new processes to improve OAC prescribing dependent on our study findings.
The survey link was sent by the EOPCN administrator directly to the email addresses of 60 member family physicians in October 2019, and participation in the survey was voluntary. The survey link presented the study information letter and survey questions to the participants. Survey end date was December 2019 and completion of the survey was considered informed consent.
The self-designed 18-item online survey (Supplemental Appendix 1) consisted of multiple-choice and open-ended questions that asked about the family physician’s demographic information, factors that impact their decisions to start OAC therapy, their comfort level and type of decision-making tools, if any, they employ. Regarding shared decision-making, family physicians were asked about their patients’ roles in the decision to start OAC therapy and were asked to rank their agreement on a Likert scale regarding various statements about OAC therapies and patient perspectives.
Survey data was anonymous and descriptive statistics were used to analyze quantitative responses. Open-ended survey responses were grouped and categorized into common themes by a Research Assistant. The study was approved by the University of Alberta Health Research Ethics Board (Pro00090690).
Results
A total of 20 family physicians participated in the study, with a response rate of 33%. The average age of participants was 44.7 years (SD 1.6); 75% were females; and the average years in practice was 15 years (SD 11.5) (Table 1). When asked the percentage of their practice that consisted of patients ≥75 years of age, 7/20 (35.0%; 95% CI: 15.4-59.2) participants reported that >20% of their practice consisted of patients ≥75 years of age, while 8/20 (40.0%; 95% CI: 19.1-63.9) participants reported 10% or less of their practice consisted of patients ≥75 years of age. Nearly half of the physicians reported that 6% to 10% of their patients ≥75 years of age also had atrial fibrillation (9/19; 47.4%; 95% CI: 24.4-71.1) (Figure 1). In terms of estimation of the percentage of their patients ≥75 years of age with AF who were on anticoagulation, 8/19 (42.1%; 95% CI: 20.3-66.5) of participants estimated that >40% of their patients ≥75 years of age with AF were on anticoagulation, compared with 5/19 (26.3%; 95% CI: 9.1-51.2) of participants who estimated only 1%-5% were on anticoagulation (Figure 2). With regards to experience initiating OACs in this population within the past 3 months, 8/17 (47.1%; 95% CI: 23.0-72.2) of participants reported starting up to 3 patients, and 8/17 (47.1%; 95% CI: 23.0-72.2) of physicians had not started OACs in any patients.
Characteristics of Family Physician Participants (n = 20).


Physician reported estimates of the percentage of their patients 75 years and older who have atrial fibrillation.

Physician reported estimates of the percentage of their patients (75 years or older) who are on oral anticoagulation for atrial fibrillation.
The most reported factor that family physicians considered when deciding to start an OAC in an AF patient ≥75 years of age was a patient’s risk of falls, bleeding, or stroke (17/20, 85%; 95% CI: 62.1-96.8). Other factors physicians considered included patients’ overall health (15/20, 75%; 95% CI: 50.9-91.3), patient preference (12/20, 60%; 95% CI: 36.4-80.9), drug properties (8/20, 40.0%; 95% CI: 19.1-63.9), drug coverage (4/20, 0%), and laboratory access (4/20, 20.0%; 95% CI: 5.7-43.7). Family physicians’ rating of how often certain factors influenced their decisions to start OACs in this population is depicted in Figure 3. Moreover, to determine a patient’s risk of stroke or bleeding, family physicians reported using the CHADS2VASC (13/14, 92.9%; 95% CI: 66.1-99.8) and HASBLED (11/15, 73%; 95% CI: 44.9-92.2) tools, respectively.
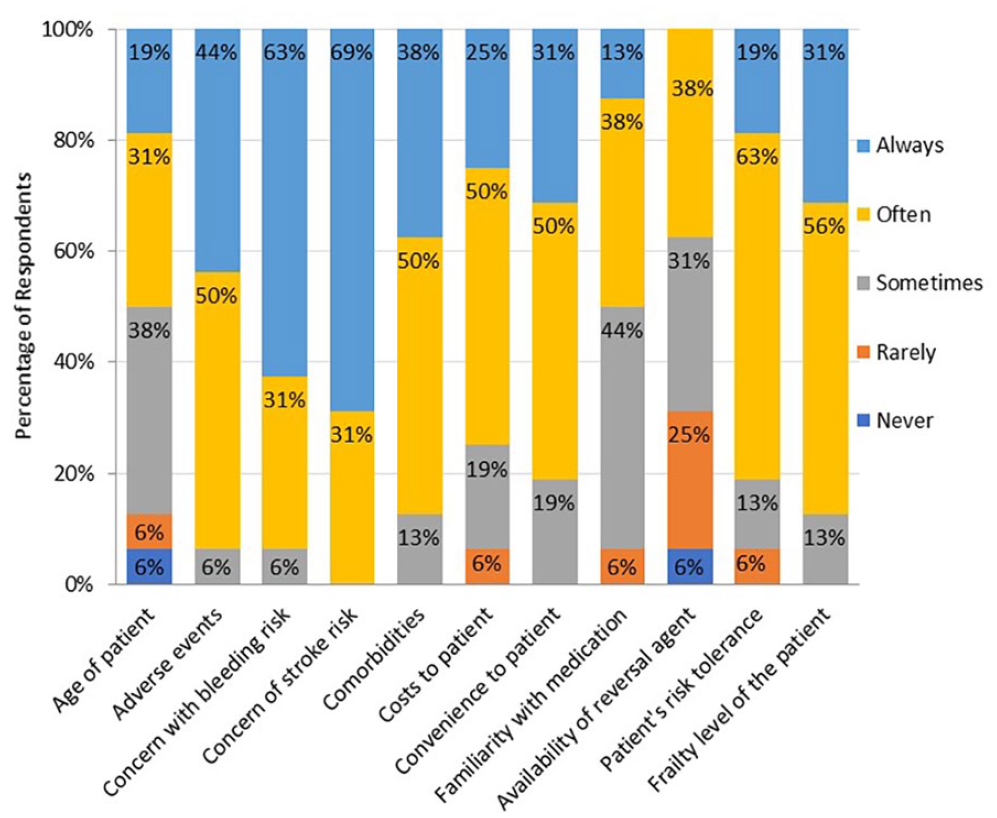
Factors influencing family physician’s initiation of OAC in patients 75 years of age and older with atrial fibrillation.
When asked whether they felt confident initiating OAC for patients 75 years of age and older with AF, 11/15 (73%; 95% CI: 44.9-92.2) of family physicians agreed or strongly agreed that they do feel confident. In contrast, 3/15 (20%; 95% CI: 4.3-48.1) neither agreed nor disagreed with the statement, and 1 (6.7%; 95% CI: 1.7-31.9) disagreed (Figure 4). However, all participants agreed or strongly agreed that their patients participated in SDM to initiate OAC for stroke prevention. All family physicians felt that their patients were well-educated on the indications for OAC for stoke prevention in AF, and that they understood treatment options, benefits and risks associated with anticoagulation (Figure 5).

Physician confidence initiating OAC therapy for stroke prevention in AF patients 75 and older.

Physician perception on the use of shared decision-making when initiating OAC for AF patients aged 75 and older.
With regards to building confidence in initiating OAC in their patients ≥75 years of age with AF, more than half of the physicians (9/15, 60%; 95% CI: 32.3-83.7) reported that an increase in some form of education was needed. In addition, 2/15 physicians (13.3%; 95% CI: 1.7-40.5) stated more clinical experience was required, and 2/15 (13.3%; 95% CI: 1.7-40.5) physicians reported enhanced knowledge of scoring tools would help build confidence, while 1 (6.7%; 95% CI: 0.2-31.9) was unsure what was needed, and another (6.7%; 95% CI: 0.2-31.9) stated that increasing coverage for direct oral anticoagulants would increase their confidence in initiating therapy.
Discussion
Atrial fibrillation is the most common sustained cardiac arrhythmia and considered a public health crisis due to its increased prevalence in an aging population and high healthcare costs from adverse outcomes. 19 The mainstay therapy of AF for stroke risk prevention remains oral anticoagulants (OACs). While rates of OAC use in elderly patients have increased significantly following the introduction of novel direct oral anticoagulants (NOACs), 18 OACs are still underused in elderly patients, particularly those 75 years of age and older. In this population, there remains discordance between guideline recommendations and clinical practice, whereby OACs are underused in older adult patients, particularly those 75 years of age and older. For our study, we did not make distinctions between older OAC agents such as warfarin, or newer agents like dabigatran, apixaban or rivaroxaban (NOACs), as we aimed to understand family physician’s perspectives in initiating any OACs in their older adult patient group. Even though our study did not directly investigate reasons for under prescribing of OACs in older adults, the strength of our study is the recognition that most anticoagulant therapies are prescribed by family physicians and thus inquiring about their practice habits regarding the use of OACs in patients ≥75 years of age with AF provided opportunity to gain insights that can inform future management strategies.
Our study found that the risk of stroke, bleeding, and falls had the strongest influence on family physicians’ decision to start OACs in patients 75 years of age and older with AF. To weigh the risks of stroke and bleeding, physicians reported using risk stratification tools like the CHADS2VASC and HASBLED scores respectively. In a recent update, the Canadian Cardiovascular Society (CCS) guideline recommended the use of CHADS-65 score, rather than CHADS2VASC, to ascertain which older adult patients warrant anticoagulation. 20 Regardless of whether CHADS2VASC or CHADS-65 scoring systems are applied to patients aged 75 and older, both tools recommend the use of OACs based on a heightened stroke risk in this age group. Interestingly, a study by Cullen et al of community-based outpatients with AF, noted that stroke risk significantly affected OAC use among those with low bleeding risk versus those with high bleeding risk where there was consistently lower use of OAC regardless of stroke risk. 21 The decision to withhold OAC in patients with higher bleeding risk is especially important in the elderly population, as elderly patients do have a higher risk of bleeding but often derive the greatest benefit from anticoagulation for stroke prevention in AF. 22 Increasing age was also recently found to be an independent risk factor for the development of ischemic stroke in patients with AF, 23 reinforcing the importance of appropriate use of OAC in elderly patients with AF.
In terms of bleeding risk, the HASBLED score considers 9 factors which are individually scored to determine a patient’s overall risk of major bleeding while on OAC for stroke prevention in patients with AF. Fall risk or number of falls is not taken into consideration in the HASBLED score but was reported commonly by participants in our study to be a factor that strongly influences their decision to initiate OAC in older adults with AF. Falls are a common geriatric syndrome impacting quality of life, morbidity, and mortality; but in a 12-month study of 515 adult patients on oral anticoagulation, the incidence of major bleeding was not significantly different between patients at high risk for falls and those at low risk. 24 This suggested that being at high risk for falls may not be a justification to defer anticoagulation, which contradicts common belief among family physicians in our study. Another study had reported that a patient would need to experience 295 falls in 1 year for the risk of intracranial hemorrhage to outweigh the risk of initiating warfarin for stroke prevention in AF. 25 Current literature and data do not support withholding anticoagulation based on a patient’s risk of falls, and this highlights a potential gap in physician knowledge and a need for further education. Given the limited sample size of our study, generalization that the same emphasis of fall risk amongst older adult patients may exist in a larger proportion of family physicians is limited and could be an avenue of future study.
In our study, patient frailty was also found to influence the decision to initiate OACs in elderly patients. A systematic review in 2018 evaluating the association between frailty and AF found up to a 4-fold increase in frailty among AF patients, particularly with increasing age. 26 Frail older patients are less likely to receive anticoagulation with warfarin in both inpatient and outpatient settings, are significantly more likely to experience embolic stroke and have higher mortality rates; but do not have a significantly increased risk of major hemorrhage. 27 In a recent large cohort study of AF patients, the clinical benefit of OAC was maintained in AF patients with varying levels of frailty, including those with moderate to high levels of frailty but not in end-stage frailty. 28 It is therefore important to recognize that frailty alone should not preclude the use of OACs in elderly patients with AF.
Shared decision-making can be especially valuable in situations where some uncertainty may exist in reference to the risk-to-benefit ratio or in the applicability of clinical guidelines, such as initiation of OAC for stroke prevention in older persons living with AF. Given the trusted, longitudinal relationships that family physicians have with their patients, family physicians may develop a greater understanding of patient context, preferences, and values. Most patients would prefer to be active participants in the decision-making process and may use different values for decision making than the values considered to be important by their physicians. 29 In fact, there can also be considerable variability between physician and patient perspectives on the outcomes of AF prophylaxis, rendering shared decision-making a crucial part of the process. For example, a study showed when considering stroke prevention therapies in AF, physicians are more concerned about avoiding bleeding, while patients are more averse of stroke. 30 These incongruities highlight the importance of not only considering, but also ascertaining patient preferences when considering the initiation of OAC for stroke prevention in AF. Results from our study revealed that all physicians felt they used SDM and agreed that their patients were educated on the use of OAC for stroke prevention in AF. While all physicians perceived the use of SDM, patient perception itself was not studied and may differ from that of the physician. An American study examining the use of shared decision-making amongst patients with newly diagnosed AF found that half of all patient’s felt decisions were made entirely by their health care providers. 31 While not examined in this study, a future study could attempt to correlate physician perception and patient perception regarding the use of shared decision-making to identify any discrepancies, and to further evaluate barriers to involving patients in their own care.
Results showed that family physicians lack confidence in initiating OACs, despite awareness of validated risk assessment tools and use of SDM. Increased education was the most reported factor needed to increase physician confidence, but further exploration is warranted to determine other factors influencing their confidence. Pharmacist intervention in the care of patients with AF may improve the identification of patients with AF and assist in ensuring patients are on appropriate OAC regimens 32 ultimately reducing the risk of strokes in at-risk patients with AF. Therefore, promoting greater collaboration between pharmacists and family physicians, ideally through pre-established primary care networks where this collaboration is already available, may be one avenue to enhance physician confidence.
Study Limitations
There are some limitations within this study. The small sample size may limit the generalizability of the findings. However, despite the small sample size, the participating physicians represented an experienced cohort of family physicians, working within a primary care network, averaging 15 years in clinical practice, and with a significant proportion of older adult patients in their practice. Another limitation may be the study survey design. Family physicians are a challenging group of participants to solicit their views and though the mixed multiple-choice and open-ended survey design permitted participants to efficiently share their unique insight, it limited the depth and statistical analysis of the findings. Regardless, the results of this study do provide insights into prescribing practices and preferences of family physicians concerning the use of OAC in elderly patients with AF, an understudied area in the literature, and generates several avenues for future investigation.
Conclusions
This exploratory study of family physician’s management practice and perspectives, confirm that family physicians contemplate several factors, including patient’s risk but also other geriatric health and social complexities, when prescribing OACs in patients 75 years of age and older. Our findings indicate that despite awareness of risk assessment tools and reported engagement of shared decision-making with their patients, family physicians admit to a lack of confidence in prescribing OACs in this high-risk group. This highlights potential areas of future research including patient perspectives on the SDM process, understanding barriers and enablers of clinician’s guideline-adherent prescribing of OACs for stroke prevention, research into long term safety on the use of novel OACs in older adults, and educational needs including effective communication strategies/knowledge translation between patients and family physicians.
Supplemental Material
sj-pdf-1-jpc-10.1177_21501319231164060 – Supplemental material for Family Physician Prescribing Practices and Perspectives on Shared Decision-Making Regarding the Use of Oral Anticoagulants for Stroke Prevention in Patients 75 Years or Older With Atrial Fibrillation
Supplemental material, sj-pdf-1-jpc-10.1177_21501319231164060 for Family Physician Prescribing Practices and Perspectives on Shared Decision-Making Regarding the Use of Oral Anticoagulants for Stroke Prevention in Patients 75 Years or Older With Atrial Fibrillation by Jahaan Ali, Reza Abbasi-Dezfouly, Sheny Khera, Paul Kivi and Peter George Jaminal Tian in Journal of Primary Care & Community Health
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project received funding from the Northern Alberta Academic Family Medicine Fund, an internal grant in the Department of Family Medicine, University of Alberta.
Ethics Approval
This project received ethics approval from the University of Alberta’s Health Research Ethics Board (Study ID Number Pro00090690).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.