
Abstract
Introduction:
This participatory action research was conducted by the collaborative health-related team in a district, in Thailand. The community network jointly developed a care model for diabetic patients in primary care using the Chronic Care Model (CCM) and evaluated the effectiveness of implemented model.
Methods:
Data was collected between October 2021 and March 2022 and involved 2 groups: 1) a community network of 25 people including representatives of the community hospital, primary care hospital, Sub-district administrative organization, community leaders, community representatives, representatives of diabetic patients, and representatives of caregivers of diabetic patients, and 2) 41 people with type 2 diabetes and 41 of their family caregivers. The research was conducted in 4 stages: planning, action, observation, and reflection.
Results:
Both quantitative and qualitative data were collected, and the overall average knowledge scores of diabetic patients, family caregivers, and community representatives significantly increased from before (6.07 ± 2.11, 7.07 ± 1.98, P = .024, 5.74 ± 1.88, 7.37 ± 2.25, P < .001, 7.47 ± 2.44, 8.99 ± 1.72, P = .010) respectively. For satisfaction, diabetic patients were most satisfied with family caregiver support, while the community network representatives were most satisfied with their participation in planning a model for diabetic patients in primary care. After model implementation, the blood sugar-controlled patients (HbA1c < 7 mg%) significantly increased (0 and 9.76%, P = .045), although the fasting blood sugar (FBS) of diabetic patients did not improve.
Conclusion:
The development and implementation of diabetes care based on CCM, promoted community participation and involvement in diabetes care. This model mainly affected diabetic patients who could control their HbA1c level and the satisfaction of the community network.
Introduction
Diabetes is a chronic non-communicable disease that accounts for two-thirds of all deaths and disabilities worldwide. According to the World Health Organization (2021), the global number of people with diabetes increased from 108 million in 1980 to 422 million in 2014. 1 The Ministry of Public Health has reported that in Thailand, the number of diabetes patients is expected to increase from 3.02 million in 2020 to 3.17 million in 2021. 2 The elderly is more likely to have diabetes than other age groups and those whose disease is uncontrolled, are at a higher risk of developing long-term complications such as nephropathy, neuropathy, heart disease, and stroke. 3 These complications can significantly impact their health, decrease their quality of life, and increase their risk of death. 4 According to the American Diabetes Association (ADA) 2021 Treatment Guidelines, effective diabetes management requires controlling the level of HbA1c to a target of <7 mg%. 5
Effective management of diabetes requires continuous and systematic care especially having network that connects health facilities to the community to collaboratively improve patient health, reduce hospitalization rates, improve clinical outcomes, and reduce the incidence of complications. 6 The 2017 Guidelines on Clinical Practice for Diabetes 7 recommend the use of Wagner’s Chronic Care Model (CCM) or WHO’s Chronic Care Model concept for chronic care. 8 The concept encompasses 6 key principles, including: (1) having community resources and policies that focus on safety and quality of care, such as elderly or diabetes clubs; (2) establishing a health service agency with good relationships between patients, primary care hospitals, and village health volunteers (VHVs) to facilitate access to health services; (3) providing self-care support to patients aimed at empowering them to take care of themselves, such as collaborating with caregivers or family members on dietary and exercise practices and monitoring for adverse drug events; (4) designing services that help diabetic patients receive timely referrals through collaboration with the Sub-district Administrative Organization; (5) facilitating decision-making about the treatment of patients, including the provision of specialist consultations when needed; and (6) using clinical information to inform patient care, allowing healthcare providers to better understand individual patients and plan personalized care for them. To achieve the objectives of the 6 principles of the CCM, it is necessary to establish a collaborative network among healthcare services, patients, and communities to deliver comprehensive care. This patient-centered approach can engage communities to enhance the quality of life of patients.9,10
Diabetes care in primary care settings of Thailand, only 29.59% of patients were able to achieve the target HbA1c level control. 11 The current situation of diabetes patient care as usual practice in health care system in Thailand, it is fragment work with the long-time coordination among all related stakeholders. These cause the lack of continuous follow-up and patient’s awareness of their own health care is not as good as they should be. Additionally, most of the diabetes care is carried out by health professionals and no clear connection to the community. Therefore, the researcher aims to develop a primary care model for diabetic patients in a primary care setting, which incorporates community networks and follows the Chronic Care Model. The ultimate goal is to enable diabetic patients to better control their condition and support 1 another in the community for the long term (Figure 1).
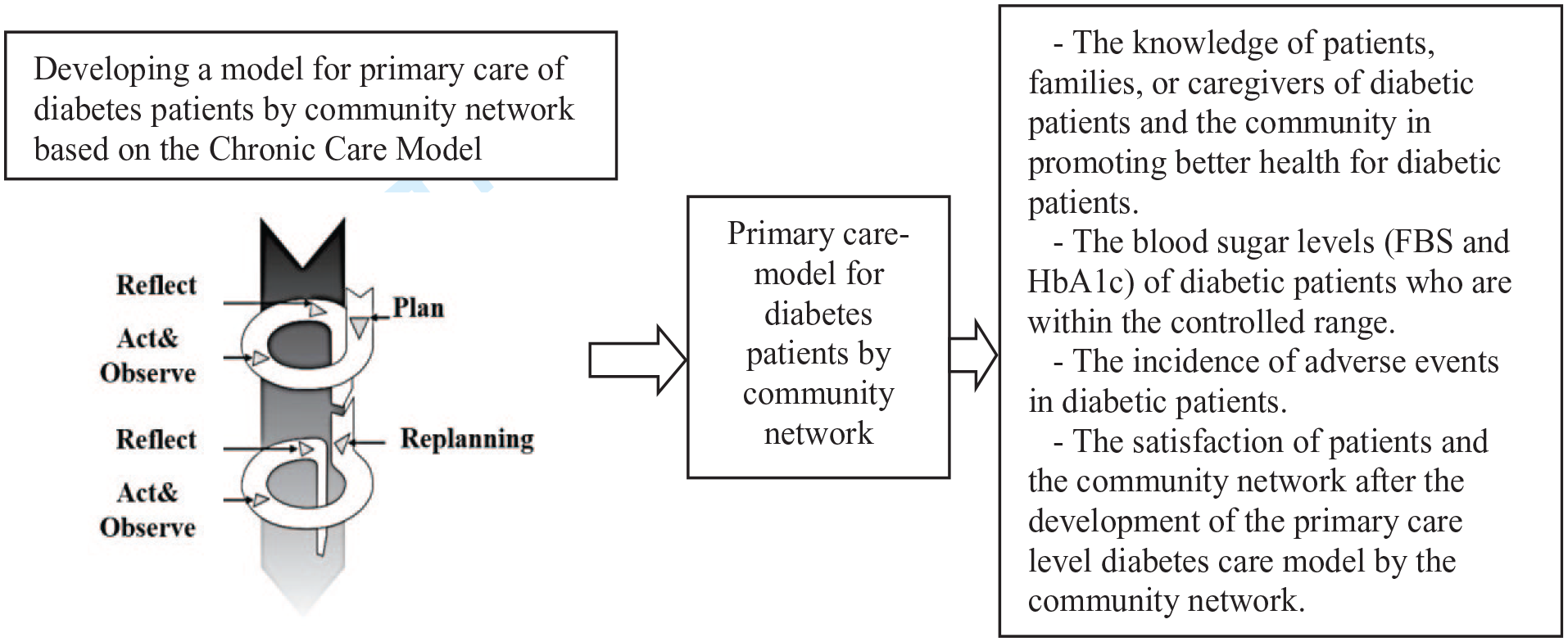
The conceptual framework of the research.
Research Method
Research design: A participatory action research, data collection took place in the primary care setting; from October 2021 to March 2022.
Samples: They were obtained through purposive sampling and consisted of 2 groups: 1) A community network consisting of representatives from community hospitals, primary care hospitals, local administrative organizations, community leaders, community representatives, representatives of diabetes patients, and representatives of families or caregivers; and 2) Type 2 diabetic patients and their families or caregivers residing in a study community.
Number of diabetic samples: confidence value (Zα/2) = 1.96, Tolerance (d) 10%, The standard deviation of the changed HbA1c value (S) = 0.98. 12 Calculated from the formula n = (Zα/2 2S2)/d2 = 37 and reserved 10% for dropouts, samples were 42. The ratio of patients per caregiver was 1:1, thus resulting in 42 families or caregivers of diabetic patient. The inclusion criteria were shown in Figure 2.

Inclusion criteria and the recruitment process of DM patients.
Research Process
Research consisted of 4 phases, based on the concept of Kemmis and McTaggart. 13 It was shown in Figure 3:
Planning Phase: this phase involved organizing a community network meeting to develop a primary care model for diabetic patients. This was done in accordance with CCM. Twenty-five community members will participate in 3 focus group discussions.
The tools used: questions used in group discussions, based on CCM. The discussion data was collected using written notes by 3 trained assistants (Table 1).
Action Phase: This phase involved implementing the diabetic care model developed in the planning phase with the collaboration of community network by the 25 representatives, 42 diabetes patients, and 42 caregivers.
The tools used: 1) The clinical practice guidelines for diabetes 2017 (Diabetes Association of Thailand under The Patronage of Her Royal Highness Princess Maha Chakri Sirindhorn) 7 and 2) an action plan, which includes details of various activities, responsible persons for each activity.
Observing Phase: This phase involved collecting and analyzing the results of the action taken during the action process. The data was collected in February 2022. All 6 components of CCM were observed, interviewed, and data recorded as detailed below. Personal interviews were conducted, and 3 trained assistants recorded the data.
The tools used: 1) patient personal data form including diabetes outcomes and adverse events 2) A blood sugar monitoring device at the fingertip (DTX), checked by a professional nurse from the primary care hospital 3) patient and community satisfaction evaluation form, Target of overall satisfaction that identified by the community network was ≥80%.
Reflecting Phase: This involved reflecting on the outcomes of diabetes care and receive feedback, suggestions for improvement and development in the next cycle. Three focus group discussions were conducted with 25 community network representatives.
The tools used: Questions used in group meetings. The data is taken by written notes of 3 assistants (Table 1).
Quality assessment tools: All forms were developed by the researchers and their content was validated by 3 experts in the diabetes care field. A patient satisfaction evaluation form and a knowledge assessment about diabetes were tested for reliability by assessing the Cronbach’s Alpha Coefficient of 0.92 and KR-20 of 0.70 respectively in a sample of 30 nearby community patients. The community network satisfaction evaluation was tested for reliability with a Cronbach’s Alpha Coefficient of 0.92 in a sample of 25 nearby community members.


Diabetes care model development and implementation cycle by community network.
Questions Used for Group Meetings in Planning Phase and Reflecting Phase.

Data Analysis and Statistics
Inferential statistics were used to compare the results before and after using the diabetes care model. These outcomes were compared before and after (1) Fasting blood sugar (FBS) and glycated hemoglobin (HbA1c) levels for 3 months. The difference of HbA1c level was analyzed using the paired t-test, while the FBS level was analyzed using the Wilcoxon signed ranks test. (2) Incidence of adverse events, and well-controlled patient were compared before and after 6 months using the McNemar Chi-square. (3) Knowledge scores on diabetes care of the caregiver and community network before and after for 3 months using the paired t-test. For qualitative data from group discussion, content analysis was done by researchers.
Study Results
The study results consisted of 4 phases as follows:
Phase I: Planning phase, the results of the development and implementation are summarized as follows:
The situation of type 2 diabetes in a primary care setting, Nakhon Ratchasima province is as follows: The target indicators for Nakhon Ratchasima Province is the percentage of controlled diabetic patients of 40% or above.

Talaad Sai, primary care setting was chosen with the reasons of 1) there are patients with diabetes whose HbA1c cannot be controlled according to the national KPI targets and 2) it is an area with a context where CCM is likely to be undertaken, that is, there are staff from the primary care hospital and the Sub-district Administrative Organization could work together in a strong way.
During the group discussions of 25 community network representatives, they identified 3 main issues of the current diabetic care: 1) Passive care approach by health personnel alone, causing delays in addressing patients’ health problems. 2) Insufficient decision support information for practitioners to provide optimal patient care. 3) Lack of a clear system for surveillance, follow-up, and patient care in the community. Figure 4 showed a new care model for patients with type 2 diabetes based on CCM was developed and done by 7 parts (Colored) of community network.
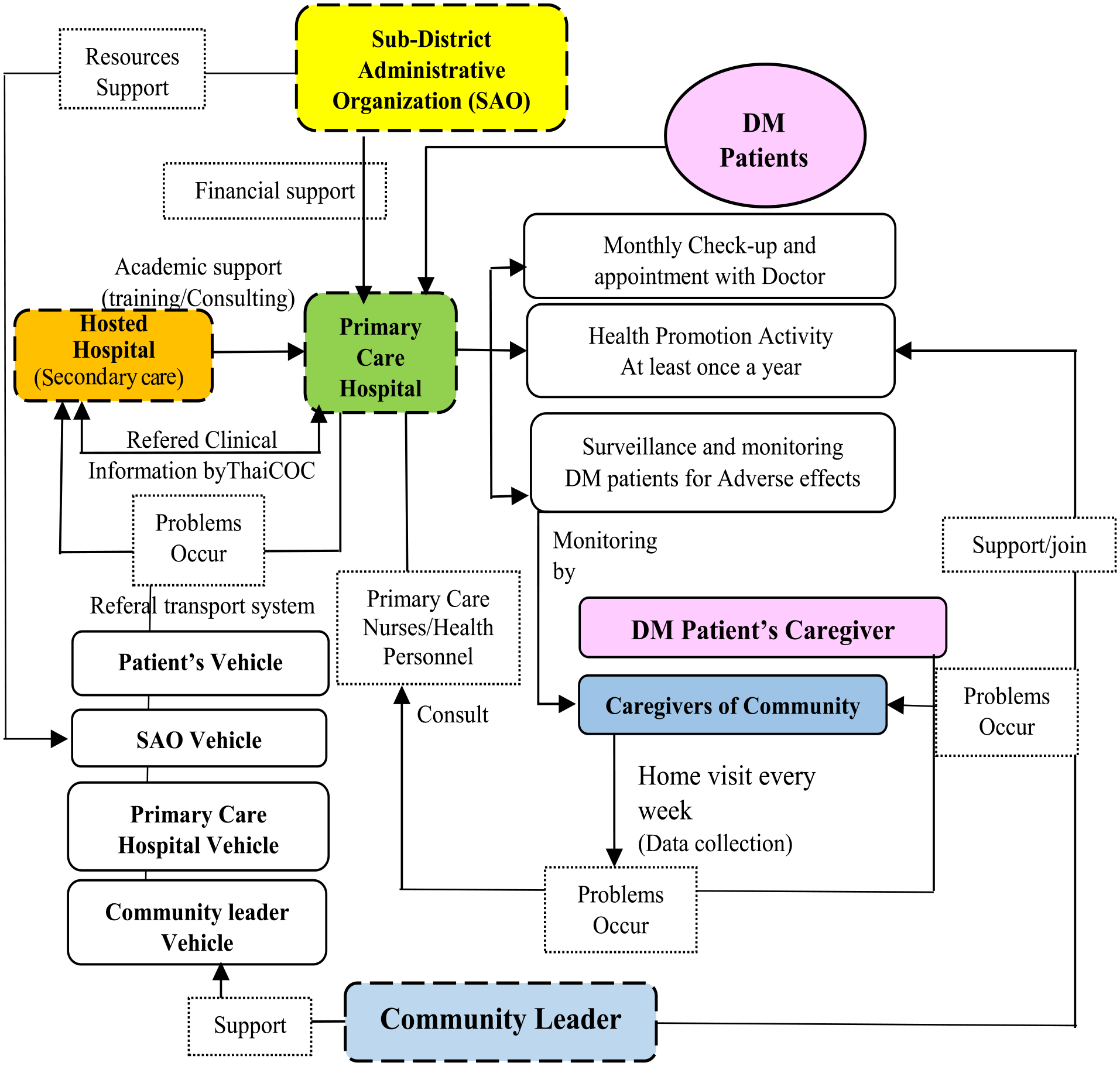
New diabetes care system in primary care based on CCM: By community network.
Phase 2: Action Phase, from a new diabetes care model in the first phase, all stakeholders of community network designed the action plan including activities, time schedule and the roles of each stakeholders. Figure 5 showed 3 main activities were performed based on CCM during November 2022 (Month 2) and January 2023 (Month 4).
Phase 3: Observation phase, the results were observed among 3 target groups: 1) diabetic patients, 2) caregivers of diabetic patients, and 3) the community representatives. The report presented 5 main findings: 1) general information, 2) the evaluated knowledge of diabetic care, 3) the satisfaction level of patients and the community network on the new diabetic care model, 4) the blood sugar levels of diabetic patients before and after the implementation of the care model, and 5) the occurrence of adverse events from diabetes before and after within 2 months.
3.1. General information of 3 sample groups (n = 107) was shown in Table 2.
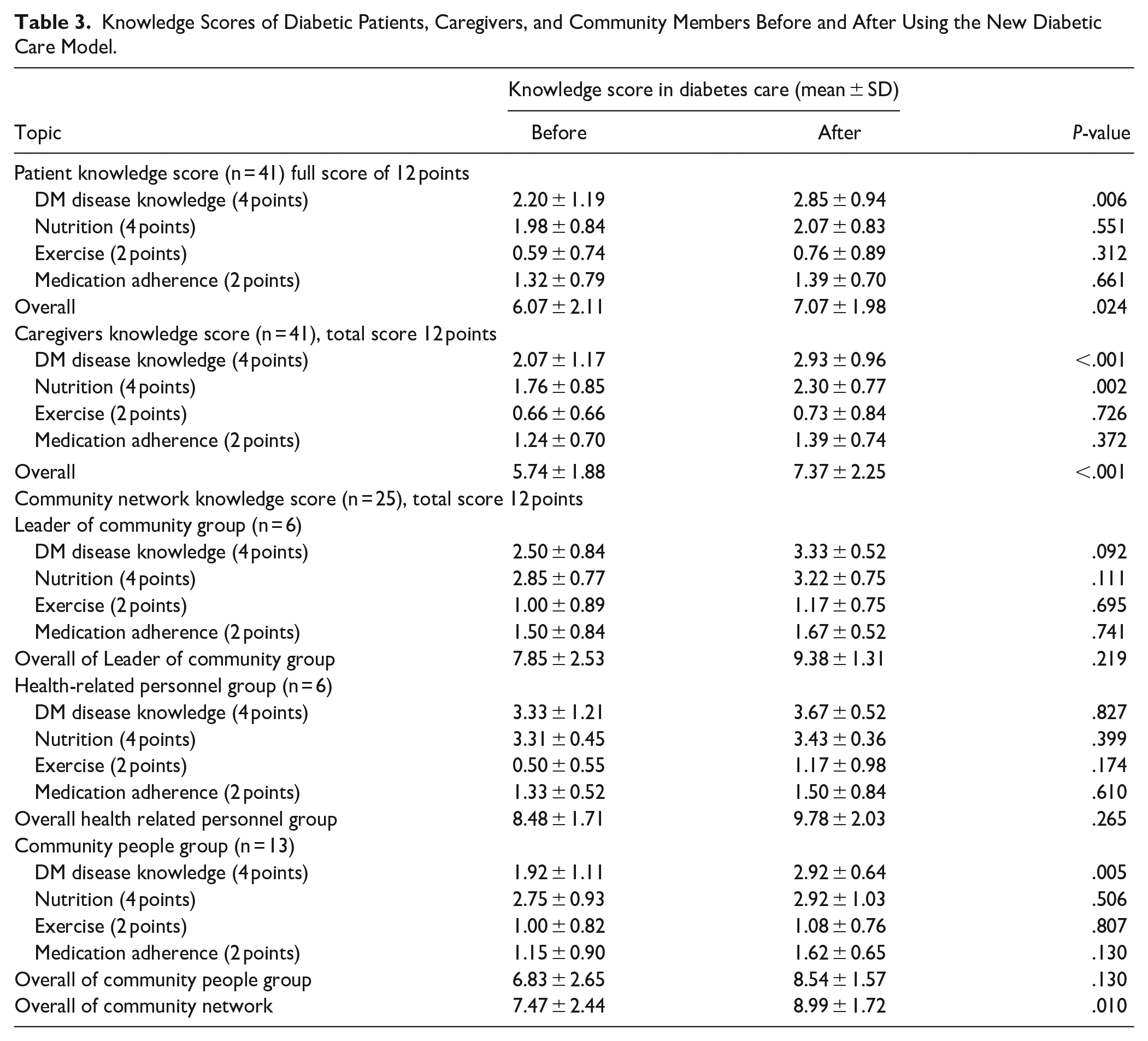
3.2 The results of knowledge score in diabetic care before and after using the new diabetic care model of 3 sample groups (Table 3): 1) Diabetic patients: the overall knowledge of diabetes before and after using the new diabetes care model was significantly different (6.07 ± 2.11, 7.07 ± 1.98, P = .024, respectively). However, there was no significant difference in knowledge about diet, exercise, and medication before and after. 2) Caregivers: the overall knowledge, before and after was significantly different (5.74 ± 1.88, 7.37 ± 2.25, P < .001, respectively). However, there was no significant difference in knowledge about exercise and medication. 3) Community network: the overall knowledge was significantly different before and after using the new model (7.47 ± 2.44, 8.99 ± 1.72, P = .010, respectively).
3.3 Satisfaction on the action or intervention in each group of 3 samples:

The integration of CCM into activities (interventions) of the action phase.
General Information of 3 Sample Groups (n = 107).

Knowledge Scores of Diabetic Patients, Caregivers, and Community Members Before and After Using the New Diabetic Care Model.
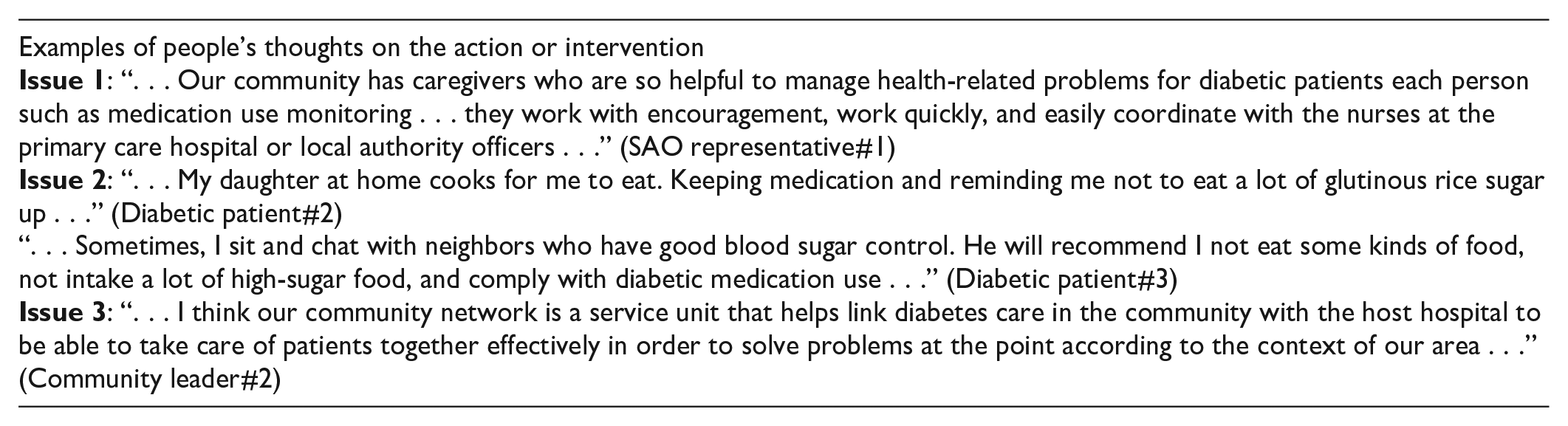
The overall satisfaction of diabetic patients was 4.03 ± 0.70, with the highest satisfaction on the help and care from their family or caregivers (4.22 ± 0.79), and the lowest score on the ability to control treatment outcomes (3.78 ± 0.85) (Table 4). From the qualitative data of interviews, 3 main issues were identified: 1) The importance of having knowledgeable and supportive caregivers to help patients manage their medication use and food intake, and provide encouragement to continue living with diabetes; 2) The significance of having supportive neighbors or siblings, inspire patients to better control their blood sugar and maintain a healthier body; and 3) The value of having a community network that helps taking care of the community health, providing a sense of security and saving time and travel expenses for hospital visits.
Satisfaction Levels of Diabetic Patients and Community Network on a New Diabetic Care Model.

3.4. The treatment clinical outcome of diabetic patients: The percentage of patients who were able to control their accumulated blood sugar (well controlled = HbA1c < 7 mg%) before and after the action plan showed a statistically significant difference (0 and 9.76%, P = .045, respectively). However, there was no difference in the level of HbA1C, number of patients who were able to control their FBS (Table 5).
3.5. Diabetes-related adverse events were investigated, there was no significant difference in the occurrence of adverse events before and after implementing the new model, including emergency room visits and hospital admissions. There is no cases of metformin-associated lactic acidosis (MALA) were found (Table 6).
4. Reflection phase: Community network had 3 meetings to reflect about 1) implementation results, 2) Strengths, weaknesses, problems, and obstacles for improvement, and 3) Summarized reflection idea. Figure 6 showed the main data from 3 meetings that were reflected by the community network for making the improvement plan.
Treatment Clinical Outcomes of Diabetes Patients Before and After Using the 3-Month Diabetes Patient Care.

Using McNemar Chi-square test.
Using paired t-test.
Statistical significance at P < .05
Adverse Events From Diabetes Before and After Using the Diabetes Patient Care Model (n = 41).


Results of the reflection phase.
Conclusion and Discussion
From the 4-component PAR process: planning a new diabetes care model that emphasizes network within the community based on CCM. CCM was used as the grounded idea of designing a plan, assigning the responsible persons, pooling resources, and planning the main activities among the community network. Three-month implementing the action plan, observing the outcomes and reflecting the results were done. Effectiveness of the diabetes care model, patients revealed the most satisfied on assistance and care from family or caregivers, which is consistent with qualitative data that suggests having family help care for the patient resulted in improved motivation for disease self-control. The community network also showed the highest satisfaction being on their participation to plan the diabetes care. In terms of clinical outcomes, follow-up on blood sugar levels showed that patients were able to control their cumulative blood sugar levels well (HbA1c < 7 mg%) which was statistically significantly different. Reflection phase showed that the recommendations on diabetes care such as enhancing the capacity of primary care hospital staff, community leaders, diabetes patients, and caregivers in the areas of nutrition and developing the operating system of the community caregivers to enable them to provide more efficient care to the community members.
In terms of Diabetes care model development and implementation in the previous studies, those conducted by Pannongpon et al 14 using practical action research, and Thumthaew et al 15 using an action research, employed process similar to this study. Both found that the results of knowledge scores on diabetes self-care after receiving care in the new model were significantly higher than before. This reflects that additional knowledge-enhancing activities, practical skill-building, and family members’ involvement in patient care contribute to the patient’s increased knowledge and understanding of self-care. In term of the effectiveness of diabetes care on controlled blood sugar level, the longer-term interventions (1-3 years) by Nuckols et al 16 and 8-month intervention by Doupis et al 17 showed better results. Thumthaew et al 15 conducted a study with a 3-month intervention, similar to this study, but collected data at different times, which may have resulted in different results. Providing the diabetes care, the community network has to concern on intervention period, seasonal effects and treatment regimens change. In this study, the data collection period did coincide with the New Year festival, during which many families gathered together to celebrate, often affecting their dietary habits. Additionally, the period also coincided with the COVID-19 pandemic, during which people were understandably more concerned about viral infection and may not have been as mindful of their dietary habits as they could have been. This highlights on the importance of dietary behavior in controlling the accumulation of blood sugar of patients, as seen in the study by Thumthaew et al, 15 which found that improving dietary behavior can help control blood sugar levels and having family members involved in care and showing more concern for patients helps patients control their blood sugar better.
The development of a primary care on diabetes using CCM, incorporating all 6 components, has fostered collaboration among various community sectors to provide holistic and comprehensive care team and to encourage diabetic patients to reach the treatment target. This finding is consistent with the study by Baptista et al, 18 which emphasizes the importance of network teamwork in producing the most effective patient care.
Limitations and Suggestions
There were some limitations of this study included that the intervention period of this study was only 3 months, which may be considered too short for effective diabetes care. Future studies should consider extending the intervention period to focus on the long-term approach of enhancing community members’ ability to take care of themselves. This research was burden by the COVID-19 pandemic, which caused delays in the project due to difficulty accessing the community and a shortage of personnel, the periodically reviewing the plan and continuous keeping the progress by each unit of the community could maximize feasibility of the project in that situation.
The participation from various sectors was crucial to providing holistic care for patients in the community, CCM with a primary focus on the community is a good framework. Therefore, it is recommended to use this research approach for continuous development and involve community members in the care program to ensure long-term sustainability.
Footnotes
Data Availability Statement
The data presented in this study are the part of the master degree of primary care pharmacy. They are approved by Faculty of Pharmacy, Mahasarakham University, Thailand.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was financially supported by Mahasarakham University. The funder had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Institutional Review Board Statement
This study was approved by the Ethics Committee of Mahasarakham University with an approval number of 109-047/2564.
Patient Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the patients and caregivers.