
Abstract
Introduction
The literature offers abundant evidence of the importance of primary care in improving the management of people’s health.1-4 Studies have increasingly highlighted nurses’ and particularly registered nurses’ fundamental role in patient management and follow-up.5-10 In primary care, nurses’ activities can be grouped into several sets of activities.11-13 Intermittent activities are performed in response to occasional needs and are often procedural. Examples are patient triage and support to physicians’ clinical activities. Integrative activities, on the other hand, favour optimal use of nurse competencies. Among these are the systematic follow-up of patients.8,14 Systematic patient follow-up is a care provision model geared toward specific patients that is intended to improve clinical outcomes and is based on deep knowledge of these patients’ needs. 15 In this type of follow-up, the nurse assesses a patient’s health status and then plans care and interventions based on what the patient needs. The nurse acts as a coordinator of the care process 15 and guides the patient toward other resources in the health care services network. Systematic follow-up of patients favours optimal use of nurse competencies. In Quebec, systematic patient follow-up by nurses has been implemented since the mid-1990s.
Several studies have shown that the management of patients by nurses in primary care has a positive effect on patients’ satisfaction, experience of care, and care outcomes.16-19 However, most of these studies have compared nursing practice with that of physicians at a global level, without taking into account the different activities carried out by nurses, and have concentrated mainly on primary care nurse practitioners.20-23 Few studies have analyzed patients’ experience of care while taking into account registered nurses’ role in primary care. More particularly, no study has analyzed patients’ experience of care from the standpoint of accessibility, continuity, comprehensiveness, responsiveness, and care outcomes, in relation to systematic follow-up by registered nurses.
Aim of the Study
The objective of this study was to evaluate patients’ experience of care in primary care as it pertained to the nursing role. The aim was to test the hypothesis that, in primary health care organizations where patients are systematically followed by a registered nurse, and where nursing competencies are therefore optimally used, patients’ experience of care is better.
Methods
Study Design
This cross-sectional study was a secondary analysis of data coming out of a large study evaluating primary care performance with regard to patients’ experience of care in Quebec in 2010. 24 In that large study, two surveys were conducted in Quebec’s two most populated regions, Montreal and Montérégie, which account for more than 40% of Quebec’s total population 24 ; these regions are divided into 23 health and social services center (HSSC) territories. The first was a population-based telephone survey of 9180 randomly selected adults (aged 18 years or older). The sample, nonproportionally stratified, consisted of approximately 400 respondents from each HSSC territory. Response rate was 56%.25,26 The second was a mail survey sent to all primary health care organizations (PHCOs) in the 2 regions (n = 606). Response rate was 62%.26,27 In each PHCO, the questionnaire was completed by a key informant, generally the physician in charge of the practice. As the study team had basic information on all the PHCOs, including nonrespondent ones, an imputation technique was applied to the latter based on probability of responses, given the region, type, and size of the practice group to which they belonged. 28 Data from the organization and population questionnaires were able to be paired because, in the population questionnaire, respondents were asked to identify their usual source of primary care.24,26
The study received approval from the research ethics committee of the Agence de la Santé et des Services sociaux de Montréal.
The Organization Questionnaire
The organization questionnaire was structured around 4 core elements: (1) vision (eg, goals, values, orientations), (2) resources (eg, availability, quantity, types of resources), (3) structure (eg, formalized rules of governance, contracts, agreements, procedures) and (4) practices (eg, coordination, administrative and professional mechanisms underlying service provision).24,29-31
The Population Questionnaire
The population questionnaire collected information on respondents’ PHCO affiliations, health services use, and experience of care.26,32 It also captured information on respondents’ sociodemographic characteristics and health status.24,26,32
Independent Variables
The organization questionnaire included the question: Are there one or more registered nurses in your organization, and if so, what activities do they perform? The response options are presented in Box 1. Respondents could check as many items as needed to describe the activities of registered nurses in their PHCO.
Box 1. Nurses’ Activities in Primary Health Care Organizations
Triage of walk-in patients
Counseling regarding smoking cessation, nutrition, and physical activity
Patient education
Counseling regarding sexually transmitted infections
Liaison and coordination with other health organizations
Support to physicians’ clinical activities
Involvement in clinical decision making
Clinical activities performed as part of a collective order
Systematic follow-up of certain patients
Dependent Variables
Based on results from the population questionnaire, five indicators for experience of care were constructed: accessibility, continuity, comprehensiveness, responsiveness, and care outcomes. The construction of indicators is detailed elsewhere. 26
Control Variables
With regard to patients, the following control variables were used: age, gender, education, financial status, perceived health status, and presence of morbidities. For PHCOs, type of organization was used as the control variable. In Quebec, there are several types of PHCOs, differentiated mainly based on their financing model, physician remuneration model, and number of physicians and other health professionals. As such, the variable “type of organization” combined into one variable all the organizational characteristics of each PHCO. Family medicine groups (FMGs) are private medical clinics consisting of a minimum of 6 physicians, 1 registered nurse, and possibly other health professionals. They receive infrastructure funding from the government. Network clinics (NCs) are private medical clinics that include several professionals besides physicians. They offer extended hours (evenings and weekends), have direct access to technological platforms (imaging and laboratories), and also receive infrastructure funding from the government. FMG-NCs have dual accreditation as both FMGs and NCs. Local community health centres (CLSCs) are public organizations that provide primary care where physicians, registered nurses, and other health professionals are on salary. Family medicine units (FMUs) are public clinics devoted primarily to the training of family medicine residents in primary care.
Construction of Study Groups
Two groups were constructed. The first group consisted of all PHCOs that reported having a registered nurse who, among the activities listed, performed systematic follow-up of patients. PHCOs in the first group could also have reported other activities performed by their registered nurses, in addition to patient follow-up. The second group consisted of all other organizations that reported having a registered nurse who performed one or more of the activities listed, but not systematic follow-up. PHCOs that reported having no registered nurse were excluded from the study.
Analyses
After the groups were constructed, linear mixed models with random intercepts and with patients nested within were used to analyze the indicators for patients’ experience of care in the 2 groups. Linear mixed models were first constructed without adjustment variables (bivariate analyses) and then with adjustment variables relating to patients and organizations (multivariate analyses).
Results
Of the 606 PHCOs surveyed, 154 reported having a registered nurse who performed systematic follow-up; these constituted the first group (n = 2670 patients). The second group consisted of the 106 PHCOs that reported having a registered nurse, but where the registered nurse did not perform systematic follow-up (n = 1694 patients). The remaining 346 PHCOs without registered nurses were excluded from the study. Table 1 presents the different types of PHCOs by group. More than 70% of the FMGs, FMG-NCs, and CLSCs reported having a registered nurse who performed systematic follow-up. The characteristics of the patients followed in the 2 groups of PHCOs showed no significant differences (results not presented).
Prevalence of Nurses Performing Systematic Follow-up by Type of PHCO.

Abbreviations: PHCO, primary health care organization; FMG-NC, family medicine group–network clinic; NC, network clinic; CLSC, local community health centre; FMU, family medicine unit.
Figure 1 presents the activities performed by registered nurses in both groups. PHCOs in the first group reported more activities performed by registered nurses than did those in the second group. For instance, in the first group, 92.2% of PHCOs reported that registered nurses engaged in patient education, whereas that proportion was only 58.5% in the second group. Likewise, in the first group, nearly three-quarters of the PHCOs reported that registered nurses looked after liaisons with other health organizations, while that proportion was less than one-third in the second group.
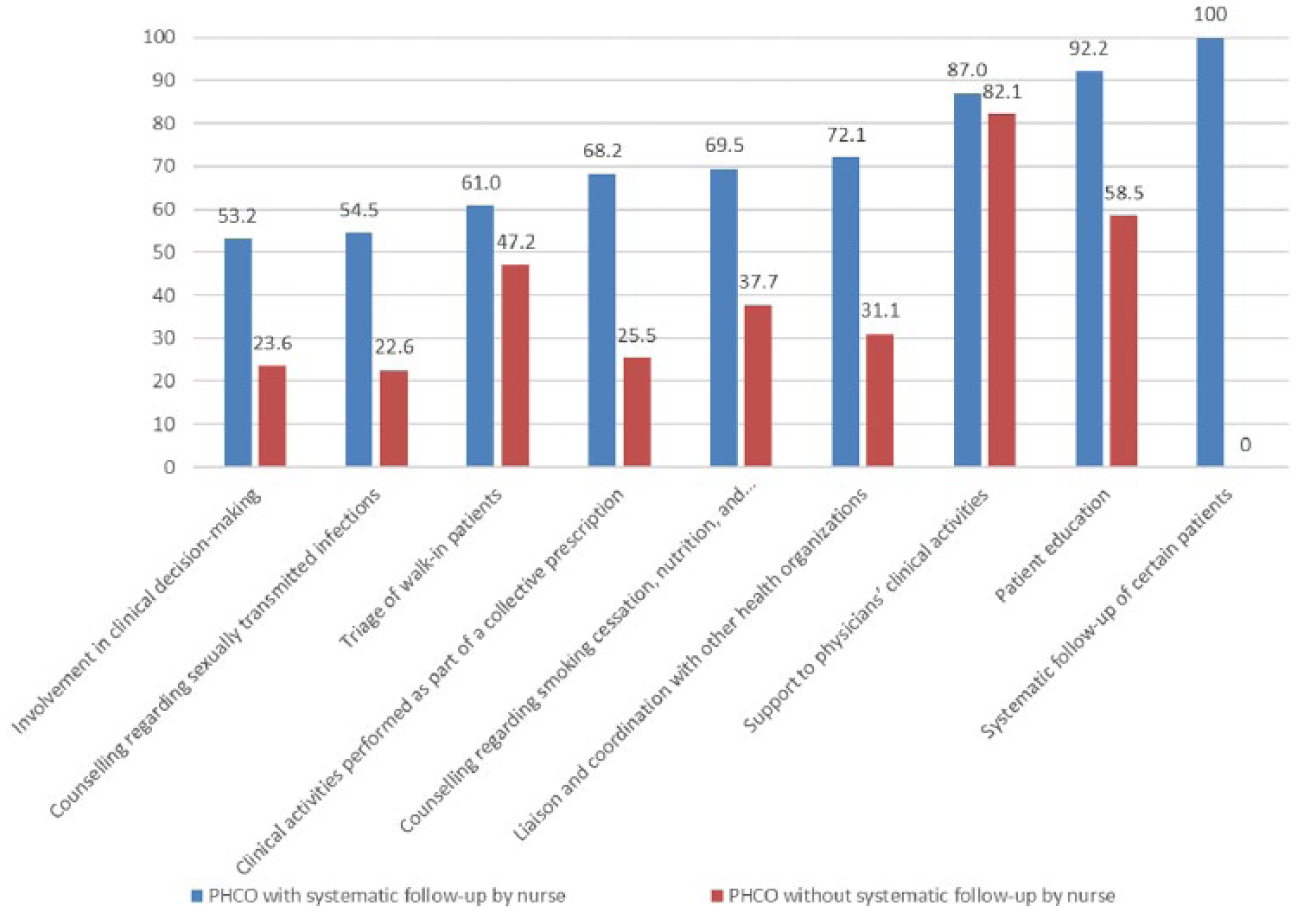
Activities performed by nurses according to primary health care organization (PHCO) group (%).
Table 2 presents the results of bivariate analyses of the indicators for patients’ experience of care by group. All indicators presented a significant difference between the two groups of PHCOs. The first group, made up of PHCOs with registered nurses who performed systematic follow-up, showed better results on all indicators for experience of care.
Mean Scores for Patients’ Experience of Care by Group.

Abbreviation: PHCO, primary health care organization.
T test (two-sample using groups).
Table 3 presents the results of the multilevel regression models constructed for each experience of care indicator. In all models, the PHCOs’ group assignment (first or second) was the independent variable. The clinic types and patient characteristics presented above were used as adjustment variables. Accessibility was the only experience of care indicator whose result was significant, remaining higher in PHCOs that reported having a registered nurse who performed systematic follow-up, as compared with those that did not.
Regression Models on Experience of Care Indicators.
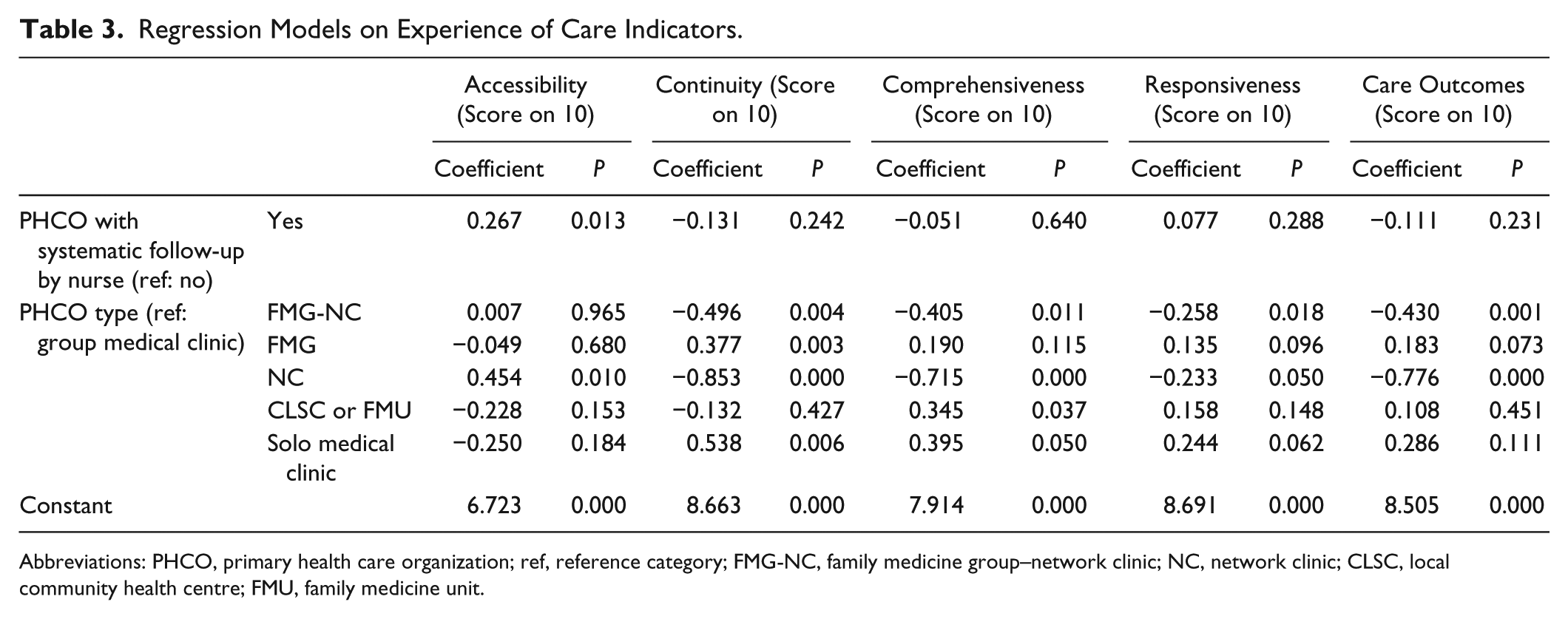
Abbreviations: PHCO, primary health care organization; ref, reference category; FMG-NC, family medicine group–network clinic; NC, network clinic; CLSC, local community health centre; FMU, family medicine unit.
Discussion
The objective of this study was to analyze patients’ experience of care in PHCOs as it pertained to activities performed by the registered nurses in those organizations. We wished to test the hypothesis that, in PHCOs where patients are systematically followed by a registered nurse, patients’ experience of care is better.
In the bivariate analyses, PHCOs that reported having a registered nurse who performed systematic follow-up obtained better results on all experience of care indicators. However, in multivariate models incorporating control variables, only the result for accessibility remained significant. PHCOs with registered nurses whose competencies were used optimally in systematic follow-up of patients thus provided better accessibility to health services for their patients. The fact that the other indicators produced nonsignificant results is due to the adjustment variable, type of PHCO, which carried a large portion of the explanatory power of the models. This is explained by the strong association between PHCO’s organizational characteristics and PHCO’s types. Presence of nurses in PHCO is one of the strong organizational characteristics. It also suggests that the organizational context plays an important role in providing conditions for an expanded role of the nurse. This finding has policy implications. Expanding the role of nurses will likely be enhanced when other favorable organizational conditions are met. Among the PHCOs that reported having a registered nurse who performed systematic follow-up of patients, most were either public PHCOs (CLSCs) or received infrastructure funding from government (FMGs, NCs, or FMG-NCs). Type of PHCO was strongly associated with certain experience of care indicators. Depending on their type, for instance, various PHCOs were associated with high indicator scores for continuity or for accessibility. 26 The strength of the relationship between type of PHCO and experience of care indicators was greater than that between having a registered nurse who performs systematic follow-up and those indicators.
The second group was made up of 41% of the PHCOs that had a registered nurse, that is, those that reported activities performed by registered nurses, other than systematic follow-up. In that group, registered nurses generally had a more limited role based on procedural competencies such as support to physicians’ activities, triage, vaccination, or follow-up of diagnostic testing. 14 In primary care, registered nurses’ involvement is often limited to procedural techniques despite the potential they represent for much greater involvement in care.6,8 In this group, accessibility was demonstrably lower. When registered nurses’ role is more procedural, accessibility seems to not be improved. PHCOs could therefore benefit from widening registered nurses’ scope of practice and using their competencies optimally in primary care to enhance access to services for patients with recurrent health care needs, such as those with chronic illnesses.
Systematic follow-up enables registered nurses to act as a case manager and to manage patients with recurrent needs. In a study on the experience of care of patients with chronic illnesses, conducted using the same data set, the authors concluded that all experience of care indicators were high for this type of patient, except accessibility. 33 By isolating the effect of registered nurses’ systematic follow-up on experience of care, our study has shown that, in PHCOs where registered nurses perform systematic follow-up, accessibility is enhanced.
In PHCOs that reported having registered nurses who performed systematic follow-up of patients (the first group), accessibility was greater than in the PHCOs of the second group. Systematic follow-up of patients is an activity that allows registered nurses’ competencies to be used optimally in their scope of practice. Many authors have stressed the importance of having multidisciplinary teams in primary care and of using registered nurses’ scope of practice to its full potential to enhance patients’ experience of care and improve health services efficiency.8,11,34,35 Sharing care between RNs and GPs could enhance primary care access but requires a paradigm change in services provision.36,37
Primary care accessibility is a key issue for health systems. In Quebec, according to the 2013 Commonwealth Fund survey, 48% of the population reported having to wait 6 days or longer to be seen by a physician or nurse; this is one of the worst results among the countries that participated in the survey. 38 Likewise, 38% of the population reported having used the emergency room in the past 2 years. Greater involvement of registered nurses would improve accessibility to health care services, thereby reducing the use of emergency services and improving health system efficiency.6,36,37
Limitations and Strengths
This study was a secondary analysis of data from surveys carried out to analyze the performance of PHCOs with regard to patients’ experience of care. For the organization questionnaire, respondents were generally the physician in charge of the PHCO or the administrative director. Thus, the activities performed by registered nurses were reported by clinic administrators and not by registered nurses themselves. As the registered nurses’ role was not the primary focus of the survey, the questions did not capture as much information as might have been obtained from a questionnaire specifically intended for registered nurses. The multivariate analyses produced a significant result for the accessibility indicator for patients’ experience of health. Sensitivity analyses for items within the other indicators confirmed the results obtained.
To our knowledge, this is the first study to shed light on the effect of registered nurses’ activities on patients’ experience of care in PHCOs. Further studies using questionnaires focused more specifically on registered nurses’ scope of practice would be needed for a deeper understanding of the links between the various activities performed by registered nurses in primary care and patients’ experience of care.
Conclusion
This study analyzed registered nurses’ contribution to primary health care. When they take on a role in systematically following patients with recurrent health needs, such as those with chronic illnesses, patients’ experience of care, in terms of health services accessibility, is enhanced. With the growing prevalence of chronic illnesses and population aging, the pressure on primary care is increasing. Involving registered nurses in primary care and using their scope of practice to its full potential is a solution that should be advanced to improve the experience of care and health system efficiency.
Footnotes
Acknowledgements
The authors acknowledge Dr Sylvie Provost who contributed to the design of the study and Odile Lemaire for the linguistic revision.
Authors’ Note
This study has been presented in French in 2 conferences: (1) Borgès Da Silva R, Brault I, Pineault R, D’Amour D, Provost S, Fournier M, Prud’homme A. Expérience de soins des patients et pratique infirmière dans les soins de santé primaires. Congrès de l’Association latine pour l’analyse des systèmes de santé. Brasilia, Brazil, July 21-23, 2016. (2) Borgès Da Silva R, Brault I, Pineault R, D’Amour D, Provost S, Fournier M, Prud’homme A. Expérience de soins des patients et pratique infirmière dans les soins de santé primaires. Conférence de l’Association Canadienne pour la Recherche sur les Services et les Politiques de la Santé/Canadian Association for Health Services and Policy Research Conference, CAHSPR. Montréal, Canada, May 28, 2015.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Our study was a secondary analysis of data coming out of a very large study evaluating primary care performance with regard to patients’ experience of care in Quebec in 2010, which was funded by the Canadian Institutes of Health Research. Roxane Borges Da Silva is funded by a Research Scholar Career Award from the Fonds de recherche du Québec - Santé. The authors wish to acknowledge the financial support of the Quebec Nursing Intervention Research Network for this research.