
Abstract
To meet both current and future competence needs, improved and updated understanding of nurses’ scope of practice when working in remote communities is needed. The aim was to describe and analyze the characteristics of nursing encounters in primary healthcare in remote areas. The setting for the study was an island community in Finland. Nurses’ patient record documentation and self-reports on patient encounters were surveyed (n = 1062). Patients aged ≥65 years accounted for most encounters. Great variety in the encounters was seen, though some nursing tasks and patient conditions were overrepresented. For patient safety reasons, it is important to review how nurses maintain competence regarding those tasks and conditions encountered less often. Primary healthcare services should focus on the broader determinants of health. However, a more disease-oriented focus was seen. To ensure quality of care in primary healthcare in remote areas, there is a need for standardized routines for monitoring patients and documenting findings and performed interventions.
Introduction
It can be challenging to deliver primary healthcare (PHC) in remote areas, because inhabitants in such areas are few and dispersed across vast spaces1,2 and those providing care often have limited access to collegial and/or medical support. For nurses, working in a remote area includes an expanded role, a wide range of responsibilities and the need for high levels of competence.3,4 To date, there is little knowledge on nurses’ scope of practice when delivering PHC in remote areas.4–7
PHC services are the foundation of healthcare systems worldwide. 1 Compared to other health services, the focus of PHC services lies on the broader determinants of health; the aim is to address the comprehensive and interrelated aspects of physical, mental and social health and well-being. Encompassing prevention, treatment, rehabilitation and palliative care, most health needs can be met through PHC services. PHC services can furthermore be used to empower individuals, families and communities to optimize their health.2,4 In the Western world today, there is great pressure on PHC services due to increasing demand,6,8,9 in part created by a growing number of older people and patients with chronic conditions.8,10,11 Accessibility and the realization of continuous patient-centered care that includes a high level of patient involvement are challenges.1,6
In remote areas, PHC services are primarily provided by registered nurses (RNs) and primary health nurses (PHNs; also called community, district or public healthcare nurses), who are often independently responsible for most patient encounters. The services that nurses in remote areas provide are varied and can include, e.g. immunizations or management of chronic diseases, common illnesses, emergency roadside trauma or injuries across the lifespan. Researchers have previously seen that even experienced nurses can feel discomfort with the broad scope of practice required when working in remote areas. 2
Factors that can impact the provision of quality care in remote areas include the healthcare provider’s degree of clinical knowledge and skill, resources (or lack thereof), and that health services are often located far away from an area’s population and not readily accessible. There is often limited access to collegial and/or medical support for nurses engaging in remote and independent work.1,6,7 Researchers find that nurses in remote areas can experience a sense of working in isolation or a lack of support. 6 In a study set in Australia, 2 researchers saw that nurses working in remote areas engaged in the process of ‘doing the best you can with what you have’ and that the outcome of this process was linked to making compromises. 2 Other researchers find that nurses in rural acute care face unique ethical challenges and that they sometimes ‘bend’ rules and take risks in an attempt to provide quality patient care. 12 Nurses practicing in remote areas often cover large geographic distances, which can result in long journeys and a lot of working hours spent traveling from patient to patient. Also, living in small communities can entail ethically challenging dilemmas and/or conflicts linked to separating private and professional information: what one knows about a patient from living in the community versus what one knows about the patient from professional practice. 12 All of these factors can make daily work, nurse recruitment and even retention difficult.4,7
There are few studies on PHC delivery in the Nordic countries, where the population density is low (17 inhabitants per square kilometer). 13 Researchers investigated the nature of nursing practice in rural and remote areas of Greenland. They concluded that nursing practice in that setting was characterized by a high degree of variability and complexity and that nurses needed a wide range of knowledge and skills. 14 In a study set in Norway, in which PHNs’ experiences with population-based work were examined, researchers concluded that there were contradictions between nurses’ actual practice, in which individual, acute patient care was focused on, and governmental directives, in which an overall, broader population wellness was focused on. In that study, the researchers found that greater knowledge and emphasis on population-based work in public health nursing was needed. 15 In a study set in Finland, in which how PHNs practice in their daily work was investigated, researchers found that PHNs held a key position in delivering healthcare. They also concluded that to manage the complexity of future societal expectations and demands, nursing education (basic and advanced levels) should be urgently developed. 16
Contextually dependent, the scope of the nursing role in PHC is continuously evolving to meet patients’ and communities’ needs. 6 To meet both current and future competence needs, improved and updated understanding of nurses’ scope of practice when working in remote communities is needed. Increased knowledge of nurses’ daily practice in remote areas can help management teams better support nurses who are working in such a context, can facilitate the recruitment of nurses with appropriate competence, and can even influence the further development of nursing education programs. The aim of this study was to describe and analyze the characteristics of nursing encounters in PHC in remote areas.
Methods
Design and setting
A descriptive survey of nurses’ patient record documentation and self-reports on patient encounters was performed. The study was performed in Finland, where PHC services are publicly funded and available to all. PHC services encompass basic medical treatment, nursing, rehabilitation, and health promotion and disease prevention, e.g. school healthcare, maternity care and home care.17–19
In Finland, RNs are required to hold a bachelor’s-level degree equating to 210 European Credit Transfer and Accumulation System (ECTS) credits and 3.5 years of full-time studies. PHNs are also required to hold a bachelor’s-level degree, equating to 240 ECTS credits and four years of full-time studies; this includes three years general nursing education (comparable to RNs) and one year of advanced studies in preventive healthcare. To work in their chosen profession, both RNs and PHNs must have authorization (license to practice a profession).19–21
The study was set in an island community in part of an archipelago that can be considered a remote area of Finland. The archipelago consists of 6,700 islands (approximately 535 square meters), of which 65 are inhabited. 22 Demographic data for the setting regarding inhabitants by age group are, in total (n) and percent (%): 0–19 years, n = 280 (13.6%); 20–64 years, n = 1,078 (52.4%); ≥65 years, n = 699 (34.0%), equating to 2,057 inhabitants in total. 23
The setting is split into five PHC districts, and services in each district are provided by either two PHNs or an RN and a PHN working collaboratively. A physician (general practitioner; GP) is also present in each district one office day per month. Depending on the district, nurses provide care for between 149 and 608 inhabitants. The nurses are on duty during office hours and additionally have on-call duty between 4:00 pm and 12:00 am on weekdays and between 8:00 am and 12:00 am on weekends. The nurses can also sign a written agreement with their employers allowing them to be contacted between 12:00 am and 8:00 am in case of emergency.
The nurses in each district work autonomously but can consult one another or other professionals. Other professionals can include the district physician, nurse colleagues from other districts or, in emergencies, an emergency department physician, Emergency Call Center officers or an RN with competence in prehospital emergency care. One challenge in the setting is the geographical distances between nurses and patients; journeys to visit patients can take up to several hours. Patients requiring more advanced care are transported by helicopter, ambulance or coast guard to a first-level hospital on the main island or directly to a university hospital on the Finnish or Swedish mainland.18,19,24
Data collection
In Finland, all nurses are required by law to document the nursing process.18,19 Patient records were therefore considered a good source whereby the characteristics of nursing encounters in PHC in remote areas could be described. The first author performed a retrospective survey of patient records in spring 2019. Patient records from a total of four weeks (two weeks in January and two weeks in July 2018) were surveyed. In total, 846 patient records were reviewed. In the preliminary analysis, it became clear that there was a relatively large amount of internal missing and/or fragmentary documentation. Therefore, the research group made the decision to engage in further prospective data collection and, consequently, to add a second step to the survey.
In step two, all nine nurses working in the setting in April 2019 were asked to self-report their nursing encounters during a 10-day period, using a study-specific protocol. This added 224 documented nursing encounters to the study data. The protocols were delivered to the nurses and collected by post. When the protocols were returned, it was noted that two nurses had chosen to voluntarily alter information in their protocols; they had not registered phone calls and some laboratory tests (about 60 encounters) during the self-report period. These are therefore missing from the data material. In total, data from 1,070 nursing encounters were collected. Patients’ ages were missing from eight nursing encounters, which led to exclusion. Consequently, a total of 1,062 nursing encounters were included in the study. The same patient could occur several times in the material.
Instrument
A study-specific protocol was developed to facilitate the collection of data from the patient records, also used in the self-reports on nurse interventions. The protocol was piloted on 10 patient records, after which some minor revisions were made, e.g. the reason for the nursing encounter was specified. In the final protocol, the following items that encompassed the characteristics of nursing encounters were included: patient characteristics (age, gender), nursing encounter characteristics (time of encounter, duration, type, setting), reason for the nursing encounter (additional patient consultation, intervention, health examination and/or preventive counselling, medical condition, assistance during physician/GP visit, administrative, no reason specified, multiple reasons), assessments and clinical interventions (laboratory test, vital signs, other assessments, clinical intervention, multiple assessments/interventions), and patient guidance and/or consultation with other professionals.
Data analysis
The results are presented in numbers (n) and frequencies (%). Cross-tabulation was performed to describe nursing encounters in relation to patient age groups. Patients one year of age or younger are registered as one-year-olds. The chi-squared test was used to estimate significant differences in characteristics. A p-value of < 0.05 was considered significant.
The data were registered and analyzed in Statistical Package for Social Sciences (SPSS) version 26.0 (IBM SPSS Statistics for Windows, Version 26.0, IBM Corp., Armonk, NY, USA).
Ethical considerations
The ethical principles delineated in the Declaration of Helsinki were used to guide the research. 25 Ethical approval was obtained from the Regional Ethical Committee part of Åland’s Public Healthcare Service in April 2018 (No. 3/2018) and permission to perform the study was granted by Åland’s Public Healthcare Service organization. Informed consent was sought from all informants prior to the start of data collection. For the data material collected from the patients’ records, anonymity was guaranteed.
When analyzing and compiling the results, threats to patient safety were identified. Therefore, the preliminary results were reported back to the management team before publication.
Results
A total of 1,062 documented nursing encounters were analyzed. The encounters were separated into patient age groups: 1–17 years, n = 60 (5.7%); 18–64 years, n = 197 (18.5%); ≥65 years, n = 805 (75.8%). Those aged ≥65 years accounted for most encounters (p ≤ 0.001). In total, women accounted for 55.5% of encounters; 39.0%, 50.0% and 58.4% respectively in each age group.
The nursing encounter characteristics are presented in Table 1. The typical encounter occurred during the day shift, lasted 0–15 minutes, was a face-to-face encounter, and took place at a primary healthcare center (PHCC). From the results, compared to other age groups and comparing the shortest visit (0–15 minutes) to longer visits (>15 minutes), those aged 1–17 years significantly accounted for the longest encounters (p ≤ 0.001). Those aged ≥65 years significantly accounted for the no patient contact (p < 0.05) and home visit/nursing home (p ≤ 0.001) encounters. In total, 71.5% of the face-to-face encounters were planned. Those aged ≥65 years accounted for the largest number of planned visits (p < 0.001): 1–17 years (63.8%), 18–64 years (48.1%), ≥65 years (78.4%).
Nursing encounter characteristics, by patient age group and in total, n (%).
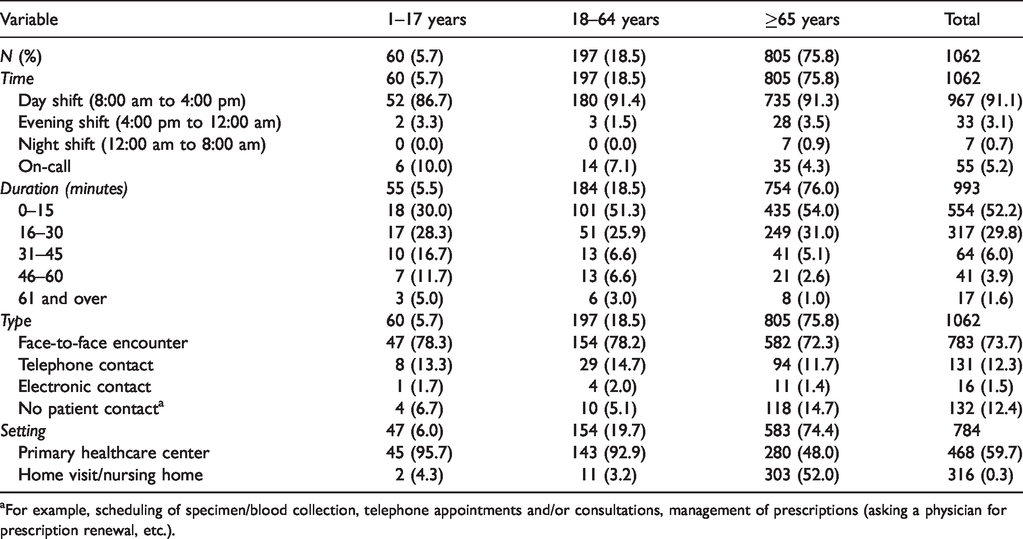
aFor example, scheduling of specimen/blood collection, telephone appointments and/or consultations, management of prescriptions (asking a physician for prescription renewal, etc.).
The reason for the nursing encounter is presented in Table 2. A total of 1,258 reasons were seen; multiple reasons for the encounter were given for 12.0% of encounters and no reason for the encounter was given for 11.8% of encounters. For those aged 1–17 years, the most common reason for the encounter was health examination and/or preventative counselling. The most common intervention was immunization/vaccination (38.1%), followed by specimen collection/blood sample (23.8%). The most common medical condition was injuries/trauma (37.5%).
Reason for the nursing encounter, by patient age group and in total, n (%).
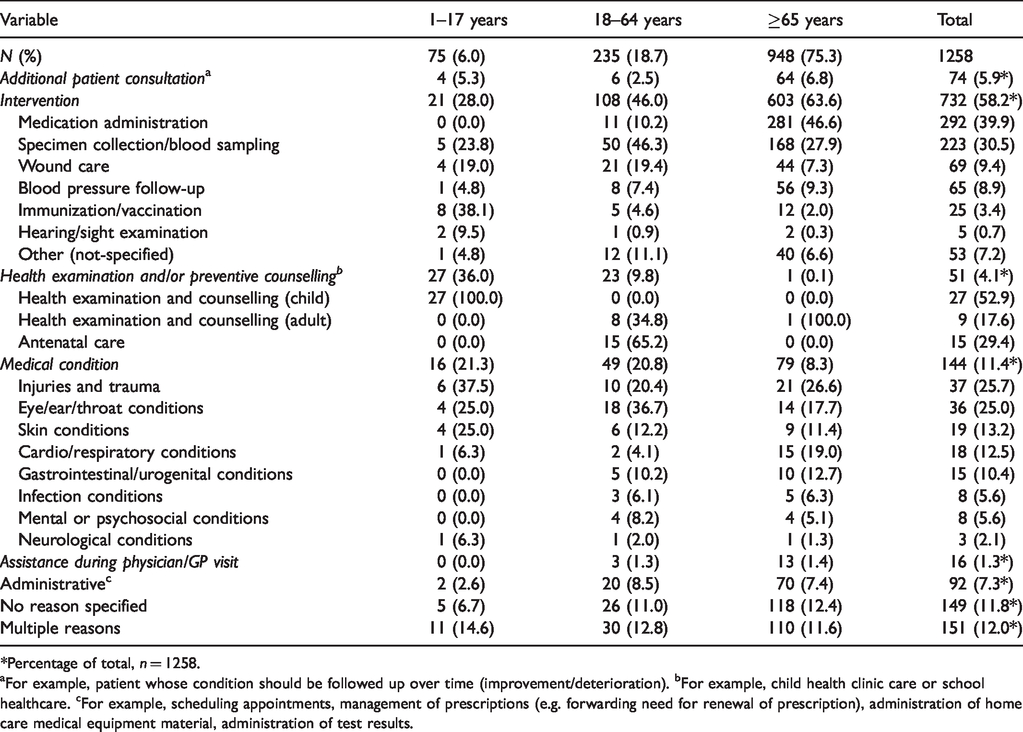
*Percentage of total, n = 1258.
aFor example, patient whose condition should be followed up over time (improvement/deterioration). bFor example, child health clinic care or school healthcare. cFor example, scheduling appointments, management of prescriptions (e.g. forwarding need for renewal of prescription), administration of home care medical equipment material, administration of test results.
For those aged 18–64 years, the most common reason for the encounter was an intervention. For this group, the most common intervention was specimen collection/blood sampling (46.3%), followed by wound care (19.4%). The most common health examination and/or preventive counselling was antenatal care (65.2%), and the most common medical condition was eye/ear/throat conditions (36.7%) followed by injuries and trauma (20.4%).
For those aged ≥65 years, the most common reason for the encounter was an intervention. For this group, the most common intervention was medication administration (46.6%), followed by specimen collection/blood sampling (27.9%). The most common medical condition was injuries and trauma (26.6%), followed by cardio/respiratory conditions (19.0%).
Assessments and clinical interventions are presented in Table 3. A total of 589 assessments and clinical interventions were registered (i.e. performed in 45.6% of all encounters). The most common laboratory test, in total and across all age groups, was blood sampling. The vital signs assessed during nursing encounters were, in total, blood pressure (51.3%), heart rate (33.2%), oxygen saturation (13.4%) and respiratory rate (2.1%). The most common other assessments were otoscopy and electrocardiogram. The most common clinical intervention was injections. Multiple assessments/interventions were performed in 151 encounters (12.0%).
Assessments and clinical interventions, by patient age group and in total, n (%).
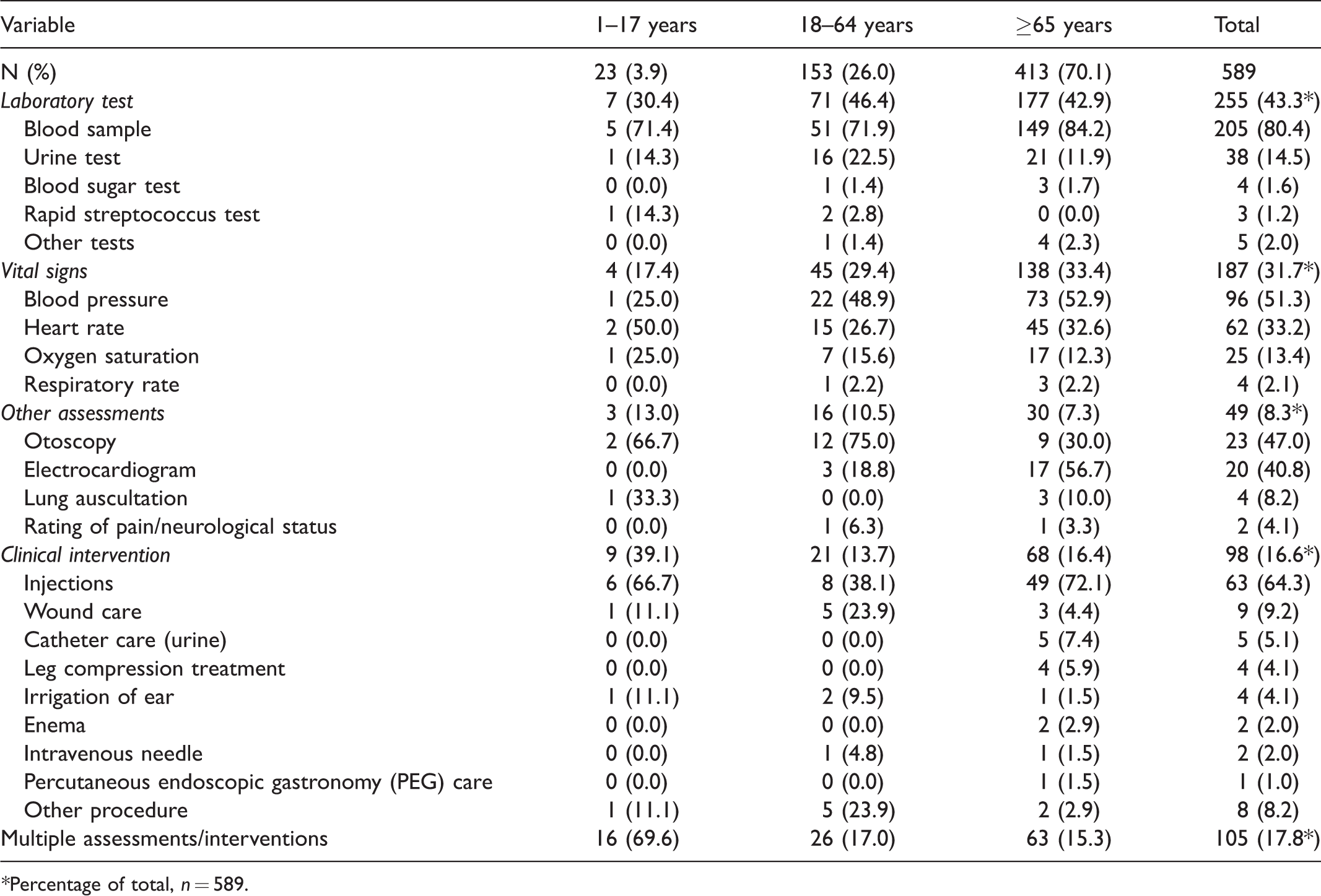
*Percentage of total, n = 589.
Nurses’ consultations are presented in Table 4. In total, 100 consultations were registered in the data material. The vast majority of consultations occurred with a physician (76.0%). Other nurse colleagues (21.0%) or others (3.0%) were also consulted during nursing encounters.
Nursing consultations, by patient age group and in total, n (%).
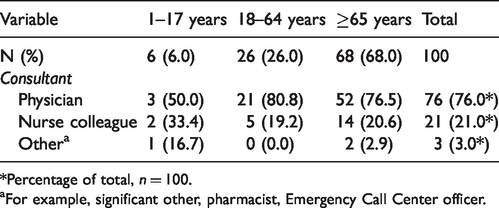
*Percentage of total, n = 100.
aFor example, significant other, pharmacist, Emergency Call Center officer.
Discussion
As seen in the results, a typical nurse encounter in PHC in the studied remote area occurred during the day shift, lasted 0–15 minutes, was a face-to-face encounter and took place in a PHCC. Those aged ≥65 years accounted for most of the nursing encounters, with those encounters taking place in a home visit/nursing home context. This was not unexpected, because the proportion of older inhabitants is higher in this region. 23 Such a trend is even seen in other remote areas, when compared to urban regions. 26 Researchers have shown that older adults use PHC services to a greater extent than other age groups.6,8 In the present study there were also multiple reasons for nearly one out of 10 nursing encounters for those aged ≥65 years. Emanating from the results, nurses providing PHC in remote areas need advanced competence in gerontology and geriatrics, including the competence to use structured assessments to detect patient deterioration. Such competence is needed to meet the needs of older adults suffering from multi-morbidity and complex health threats and to ensure patient safety and quality of care.26–29
To detect patient deterioration, competence in clinical decision-making, including structured assessment, is vital. Here, the relatively low number of documented assessments, especially vital signs, was striking. One reason for such results may be that the nurse informants used intuition instead of objective measures; given the nature of and remote setting for their work, the nurse informants know their patients well. This perhaps led the nurse informants to ‘less-than-fully’ document certain elements of the nursing encounter in the patient records. Researchers in another study have demonstrated that the lack of clear guidelines for observing patients’ vital signs and inadequate facilities for recording vital signs in electronic health records can lead to inconsistencies in the way vital signs are recorded. 5 Still, nurses are obligated to document performed assessments19,30,31 and should also document the reason(s) for the nursing encounter and any clinical intervention(s) performed. Omissions in documentation were seen in these last two areas in this study. Lack of information in patient records can compromise patient safety. Consequently, standardized routines for monitoring patients and documenting findings and performed clinical interventions are needed.
As seen in our study, the nurse informants needed competence in the administration of injections, medication administration, specimen collection/blood sampling and wound care. The nurse informants more commonly encountered patients with injuries and trauma, eye/ear/throat conditions, skin conditions, cardio/respiratory conditions and gastrointestinal/urogenital conditions; such competence is traditionally acquired during RN education. The nurse informants also needed competence in health examinations and counselling (primarily child health clinic care or school healthcare) and antenatal care; such competence is traditionally acquired during PHN education. Therefore, to meet the needs specific to the realization of PHC in remote areas, competence equivalent to the competence that RNs and PHNs possess is needed. Norbye and Skaalvik emphasize that decentralized nursing education is important for recruiting and retaining nurses in rural and remote areas. 32 Other researchers maintain that competence equivalent to the competence that nurse practitioners possess is needed in such a setting. 6 A nurse practitioner (NP) is ‘a generalist or specialized nurse who has acquired, through additional graduate education (minimum of a Master’s degree), the expert knowledge base, complex decision-making skills and clinical competencies for Advanced Nursing Practice, the characteristics of which are shaped by the context in which they are credentialed to practice’. 33
In this study, some reasons for the nursing encounter such as assessments and clinical interventions were seldom or not at all represented, e.g. diabetes and allergies were conspicuous in their absence. One can question whether competence in seldom represented areas can be maintained. Consequently, for patient safety reasons, criteria for when nurses in such settings should consult a physician and/or specialist should be drawn up.
The nurse informants seldom consulted other professionals. This is in line with other studies, in which researchers have found that nurses in remote areas often experience professional isolation.12,34 While our results here may have been affected by the omission of documentation, routines for consultations should be implemented. The remoteness of the setting should not be considered a barrier. There are many alternative means whereby consultations can be supported, such as e-health or m-health solutions. Researchers have found the use of technology in PHC to be beneficial.35–37
The World Health Organization emphasizes a move from a disease-oriented agenda toward health promotion. 4 Other researchers have seen an increased risk of poor general health and lifestyle behaviors in rural settings compared to urban areas,38–40 so this can be of special interest in the setting investigated here. In our findings we discerned a continued focus on a disease-oriented agenda. Perhaps this was because of missing and/or fragmentary documentation. However, one cannot ignore that there has been a shift in the organization of healthcare services in Finland: hospital stays have been shortened and more patients with complex health conditions are moved to PHC. The preventive and promotive aspects of PHC are vital for public health, and one should accordingly seek to limit the emergence of a focus on a disease-oriented agenda in such care.8,41 Consequently, nurses in remote areas should have good skills and sufficient expertise in driving a health-promotive agenda.2,42,43
Methodological considerations
The relatively large amount of internal missing and/or fragmentary documentation in the patient records may have affected the results. A self-report protocol was developed to compensate for this, but there were also missing data in the protocol. Two nurses voluntarily altered the information they recorded in their protocols; they did not register phone calls and some laboratory tests. It is also likely that other nurses may have left out information, e.g. because of a lack of time. This may have affected the results. Some results were also inconsistent, e.g. wound care is mentioned as the reason for a nursing encounter in 69 records, but only nine wound care interventions were documented. Further studies, including observations and interviews, are needed to gain a more comprehensive understanding of nurses’ scope of practice in PHC in remote areas.
To the best of our knowledge, this is the first survey of nursing encounters in remote areas of Finland. To capture variations over the year, data were collected during two two-week periods, once in winter and once in summer. During the summer, activities related to, e.g. school healthcare, are fewer or non-existent, thus such encounters may be underrepresented. Nevertheless, a large number of nursing encounters were collected.
Conclusion and clinical implications
Working as a nurse in a remote area requires a wide range of competence, and competence equivalent to the specific competence that RNs and PHNs possess is needed. Some nursing tasks and patient conditions were overrepresented. Competence in those areas and in gerontology and geriatrics are essential. Some tasks and conditions were also seldom represented. For patient safety reasons, it can be important to review how nurses can maintain competence in those areas encountered less often. To ensure quality of care in PHC in remote areas, there is a need for standardized routines for monitoring patients and documenting findings and performing interventions. A high degree of autonomy in the nursing role was revealed, which is linked to great accountability and responsibility. When recruiting nurses for work in PHC in rural areas, both employers and prospective employees should be made aware of the complexity and independency of the role, including the need for broad competence.
Further research on this topic is needed, including the use of other study designs, e.g. interviews and/or observations. However, the characteristics of nursing encounters in PHC in remote areas were described, and the results can be considered applicable to communities with similar geographical challenges.
Footnotes
Author contributions
The first author collected the data. The first author together with last author piloted the protocol, performed the first analysis, and created a first draft of the manuscript. All authors participated in the creation of the study design and data analyses. The second, third and last authors supervised and gave critical revisions. All authors have read and approved the final manuscript.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Funding has been received from the Swedish Cultural Foundation in Finland, Ålands kulturstiftelse r.s, Ålands Självstyrelse 75-års Jubileumsfond, and Åland University of Applied Sciences.
Acknowledgements
The authors would like to thank all the nurses diligently working in remote areas who participated in this study.