
Abstract
Homelessness poses a significant threat to overall physical well-being because of the associated challenges in accessing adequate health care services and maintaining good health, which is oftentimes related to lack of health insurance coverage and a usual source of care.1,2 Consequently, many homeless individuals are susceptible to unnecessary hospital admissions for ambulatory care sensitive (ACS) conditions, which are conditions for which appropriate primary care would likely prevent hospitalization.1,3-5 Unfortunately, most homeless individuals do not have a usual source of quality primary care or insurance coverage and are at a higher risk for hospitalizations for such conditions.
The Institute of Medicine defines primary care as the “provision of integrated, accessible health care services by clinicians who are accountable for addressing a large majority of personal health care needs, developing a sustained partnership with patients, and practicing in the context of family and community.” 6 Primary care access is positively associated with lower mortality and having a usual source of care increases the use of primary care services.7,8 Limited access to primary care services presents significant challenges in managing acute and chronic conditions. Evidence suggests hospital admissions for preventable or ACS conditions may be higher among homeless persons because of inequities in access to primary care services. 9
Several conceptual frameworks illustrate how individuals or populations obtain health services.10-13 The Equity of Access to Medical Care Framework (hereinafter referred to as the framework; Figure 1), developed by Aday and Andersen, is a comprehensive framework that assesses factors contributing to equity in access to health services.11,12 The framework defines access as “those dimensions which describe the potential and actual entry of a given population group to the health care delivery system.”11,12,14 The framework uses an ecological approach to demonstrate the interdependence of health service dimensions and how they act synergistically to promote or impede health care access. In the framework, equity is achieved “when services are distributed on the basis of people’s need for them” rather than sociodemographic characteristics.11,14 Three key beliefs are the core of the framework: (1) health care is a human right, (2) health care resources are limited, and (3) health care policy must allocate these resources equitably. The framework is useful to identify barriers and facilitators to health services experienced by underserved populations, including the homeless.
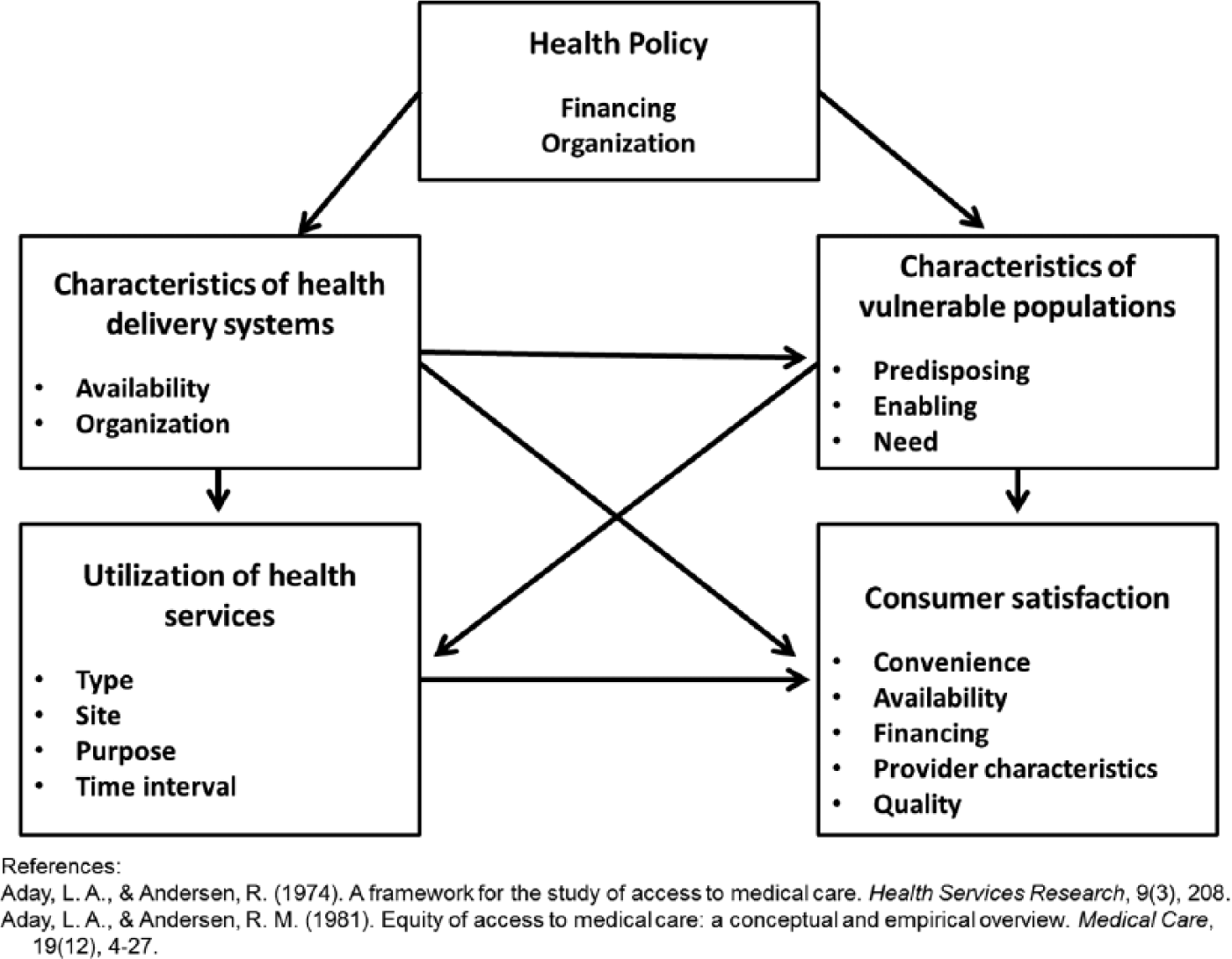
Equity of Access to Medical Care Framework.
The framework consists of inputs and outcomes, beginning with health policy initiatives, a mutable component in the framework. Medical care access is the consequence of health policy, its goal is to improve access to health services. 12 Health policy is often focused on the financial structure of medical care systems, such as the publicly funded Centers for Medicare and Medicaid Services and the Children’s Health Insurance Program. Policy affects the organization of health care programs, subsequently altering human resources or medical educational requirements. 12
Health delivery system characteristics are an input of the framework that examines medical care arrangements 12 and evaluates potential health services access. 11 Component structural indicators include the availability and organization of delivery systems.11,12 Availability describes the workforce and financial resources dedicated to providing medical services. 12 Availability empirical indicators, are the number of health personnel and/or the number of available health care facilities in an area. The organization of delivery systems describes how the resources are used to provide care. More important, it examines how consumers gain entry into the system and the continuity of care. Organization empirical indicators include the structure of the delivery system and convenience for consumers. 11 The unit of analysis for this input is the organization. This input is mutable and likely to change depending on health policy.
Characteristics of the population-of-interest are another input of the framework. 12 This input evaluates the potential access of those at-risk for having poor access to medical services, by focusing on predisposing, enabling, and health-related needs. Predisposing factors are existing characteristics that describe an individual’s likelihood of using health services. Predisposing factors include demographic characteristics (eg, age, race/ethnicity, gender), occupation, health seeking behavior, and individual beliefs. 11 Enabling factors are mutable resources individuals have at their disposal to obtain medical care 12 and include income, insurance coverage, and the convenience of having a regular source of care. 11 Need-related factors, including individual symptoms and days with a disability, are based on an individual’s existing conditions and health care needs (perceived by the individual or evaluated by the delivery system).11,12
The utilization of health services measures realized access and is the outcome of the framework’s inputs This component acts as an “external validation of the effect of the characteristics of the population at risk and of the delivery system on people’s entry (or nonentry) into the system.” 12 Utilization is described by the (1) type, (2) site, (3) purpose, and (4) time interval of the service. 12 The service type received (eg, primary care) and by whom (eg, primary care physician or nurse practitioner) are important characteristics of utilization. The time interval refers to the number of provider contacts or revisits and the continuity of care. Continuity of care is an indicator of the coordination and integration of health services 12 ).
Consumer satisfaction is a measure of realized access that consists of subjective indicators in the framework. 11 This component examines the level of consumer satisfaction with the quantity and quality of health services received. 12 Satisfaction is often focused on a specific visit or medical care episode.
The framework provides opportunities to identify barriers and facilitators to primary care access experienced by the homeless. Using this framework, this article synthesizes the literature to (1) identify these barriers and facilitators and (2) provide recommendations for medical and public health practitioners to improve health among this population. Identifying barriers and facilitators to primary care services among the homeless will offer guidance to develop targeted interventions to improve health care access and overall health.
Methods
Search Strategy
The PubMed, CINAHL, and PsycINFO databases were searched using variations of the following terms: primary care, access to care, barriers to care, equity of care, assessment of need, and homeless persons. Studies were restricted to those conducted in the United States. One reviewer (BMW) assessed titles and abstracts to determine if full-text review was warranted; full-text articles were reviewed to determine final eligibility. Reference sections of articles obtained from the initial search were reviewed, and all studies (ie, randomized controlled trials, observational studies, prospective and retrospective cohort studies, case–control studies, and cross-sectional studies, etc) that included a health utilization measure of primary care while investigating the homeless were considered. Studies that examined having a regular or usual source of care were also included.
Initially, 124 studies were identified through a preliminary search and 111 studies remained after duplicates were removed. Nine articles were chosen based on the initial search and application of inclusion criteria. After reviewing reference sections, 3 additional articles were chosen. The final synthesis was of 12 articles (Table 1), which identified barriers and facilitators to primary care among the homeless. The findings from these articles were organized by dimensions of the framework.
Summary of Articles Used in Synthesis.

Abbreviations: BMVP, Behavioral Model for Vulnerable Populations; CC, case-control matching; CCM, chronic care model; CS, cross-sectional data; DHCQ, Donabedian’s Model of Health Care Quality; ED, emergency department; HSU, health services utilization; NA, not applicable; PC, primary care; Qual, qualitative; QE, quasi-experimental; USC, usual source of care; VA, Veteran Affairs; SMI/SAD, serious mental illness and substance abuse disorders.
Data Extraction
The primary author extracted data from articles included in the final analysis. Extractions included author (publication year), study aim, conceptual model used, research design, population, primary outcome, and the major finding. We then identified which dimension of access the study addressed, based on the framework.
Results
Health Policy
To date, there were no articles specifically identifying facilitators or barriers to primary care access at the health policy level that met the inclusion criteria of this review.
Characteristics of Health Care Delivery Systems
Key characteristics of health care organizations to improve primary care access among the homeless were identified. This included the use of homeless-specific primary care delivery systems that provided access to various services in one central location. Primary care facilities that did not offer homeless services in central geographic area were obstacles to health care utilization.
One study compared homeless patients’ experiences in a primary care delivery system tailored to meet homeless-specific needs and a nontailored delivery system. 18 The sites included 3 nontailored Veterans Affairs (VA), a tailored VA, and a tailored non-VA clinic (n = 601). The 2 tailored clinics had higher patient satisfaction scores for almost all measures of patient experience, including patient–provider relationship, cooperation among providers, accessibility/coordination of care, and homeless-specific needs. Patients who received primary care services at the nontailored VA clinics were 1.5 to 2 times more likely to report an unfavorable experience (P < .01).
O’Toole et al 24 examined the impact of a tailored VA primary care medical home on health care needs and utilization patterns among newly enrolled homeless veterans. Case–control matching with a nested cohort analysis was used to examine 6-month health care use with nonhomeless veterans (n = 233). At 6 months, both homeless and nonhomeless veterans had used primary care services. During this period, homeless veterans averaged 8.4 visits per person compared with 2.5 per person for nonhomeless veterans. Homeless veterans also averaged 4.1 new clinical diagnoses. Many homeless veterans received a new diagnosis for an acute condition (74.8%) and/or a chronic condition (67.7%). At the end of 6 months, there was a decrease in the number of participants reporting unstable housing conditions; 44% reported living in a shelter or the streets at the start of the intervention, which declined to 19% at 6 months.
In a similar study, O’Toole et al 23 evaluated the effectiveness of a highly tailored VA primary care clinic on reducing emergency department (ED) use among homeless veterans. Homeless veterans who received care at the tailored clinic were compared with homeless veterans who attended a general practice clinic (n = 177). During the first 6 months, veterans at the tailored clinic had significantly more primary care visits compared with those who attended the control clinic (5.96 per person vs 1.63 per person; P < .01). This difference remained during the second 6 months; however, the average number of primary care visits for both groups decreased (1.63 per person vs 1.31 per person; P = .1). Hypertension, diabetes, and hyperlipidemia chronic disease management improved for veterans who attended the tailored clinic. These veterans also had lower ED visits for ACS conditions than the control group throughout the 12-month period.
McGuire et al 22 assessed the effect of an integrated primary care clinic for homeless veterans with serious mental illness and substance abuse disorders, on primary care access and overall physical health. The integrated clinic provided primary care, mental health, substance abuse, and social services in one location; the standard clinic linked homeless veterans to primary care and social services located in separate facilitates. Patients were followed for 18 months, with interviews occurring at baseline, and months 6, 12, 18 after enrollment. Homeless veterans at the integrated clinic had shorter wait periods for their initial primary care visit compared to patients at the standard clinic (0.3 vs 53.2 days). In addition, during the 18-month period, patients at the integrated clinic had more primary care visits per patient compared with patients at the standard clinic (7.4 vs 4.7 visits).
Characteristics of the Homeless
Several characteristics associated with being homeless were identified as barriers or facilitators to obtaining primary care. Predisposing factors included sociodemographic characteristics, enabling factors ranged from insurance status to competing needs, and health-related needs were based on existing health conditions.
Predisposing: Barriers
Chronic homelessness is a barrier to primary care access.16,25 Gallagher et al 16 predicted establishing a regular source of care among 365 homeless adults and concluded that individuals who were homeless for more than 5 years were less likely to report a usual source of care compared with those who were homeless less than 5 years (P < .05). A similar study predicted health care use among 974 homeless women. 25 Severe homelessness (ie, a long history of homelessness) was found to be a barrier to medical care. Sociodemographic characteristics are also identified as barriers to primary care access among the homeless. In a study by Gallagher et al, 16 they maintain males, Hispanics, adults younger than 41 years, those without a high school education, and nonveterans were the least likely to report an usual source of care.
Kushel et al 2 identified factors associated with health care services use among 2974 homeless and marginally housed persons, determining that individuals with a mental illness were less likely to use ambulatory care (odds ratio [OR] = 0.84; 95% confidence interval [CI] = 0.40-1.77). Psychological distress, as measured by the RAND Health Survey SF-36, was another major barrier to primary care access.25,26 The survey included statements about general mental health status in the past 4 weeks; for example, “Have you been a happy person,” “Have you felt downhearted and blue?” 26
Predisposing: Facilitators
Being recently homeless, or homeless for fewer years, was associated with increased primary care access. 15 A recent study identified factors associated with having a regular primary care provider among 750 homeless persons with a usual source of care. 15 Recently residing in one’s own home (OR = 1.01; 95% CI = 1.01-1.02) or an institution (OR = 1.01; 95% CI = 1.01-1.01), and fewer years being homeless (OR = 0.96; 95% CI = 0.93-0.99) were associated with having a usual primary care provider. For sociodemographic characteristics, Gallagher et al 16 found that females, adults 41 years and older, and veterans were the most likely to report a usual source of care (P < .05). Another study determined that Black homeless women were more likely to have a usual source of care and fewer reported barriers to health services than White homeless women. 25 Homeless Hispanic women were also more likely to have a usual source of care than White homeless women. 25 When examining unmet needs, Kertesz et al 19 concluded that Black homeless persons were less likely to report unmet needs for general medical care compared to White homeless persons (OR = 0.38; 95% CI = 0.17-0.85).
Kushel et al 2 found substance abuse to be associated with increased primary care access. Homeless and marginally housed persons who abused alcohol or drugs were more likely to use primary care in the past year than those who did not (alcohol, OR = 1.20, 95% CI = 0.57-2.52; drugs, OR = 1.33, 95% CI = 0.59-2.98).
Enabling: Barriers
Several studies identified competing priorities related to being homeless as barriers to primary care access, having a primary care provider, or usual source of health care.15-17 Competing priorities included difficulty finding food, shelter, clothing, a place to wash, and/or a place to use the bathroom. Gelberg et al 17 determined the role of competing priorities versus health services access among 365 homeless adults. Homeless adults measuring 20.4% reported having frequent difficulty meeting basic needs, and 47% reported “rarely or never” having difficulty meeting basic needs. The unadjusted logistic regression model showed those who reported having frequent difficulty meeting basic needs were less likely to have a regular source of care (OR = 0.30; 95% CI = 0.16-0.53) and less likely to have had an outpatient physician visit in the past year (OR = 0.69; CI = 0.41-1.15). In the study by Gallagher et al, 16 individuals with competing priorities were less likely to report a regular source of care (OR = 0.60; CI = 0.44-0.82). Chwastiak et al 15 likewise identified competing priorities as medical care barriers per their study participants (n = 750).
Several studies found the inability to pay for medical care as a primary care barrier. Chwastiak et al 15 surmised participants who had trouble paying for medical care in the past 3 months were less likely to have a primary care provider (47.5% vs 26.3%; P = .001). Barriers to general health care services included the following: inability to pay for services (69%), no access card necessary to receive subsidized health care from safety net facilities (56%), and lack of transportation (n = 200). 19
Enabling: Facilitators
Facilitating factors for primary care access included health insurance coverage, having a regular source of care, assistance meeting basic needs, transportation, serious mental illness, and having a greater need for medical care. Health insurance coverage was associated with having a usual primary care provider (OR = 1.57; 95% CI = 1.42-1.74). 15 Similar studies also found an association between health insurance coverage and primary care access, and reductions in barriers to medical care.2,25 Homeless adults with non-Medicaid health insurance were more likely to report a usual source of care (OR = 2.61; CI = 1.11-6.15), 16 while having a regular source of care predicted use of preventive services and outpatient medical care. 25 Other facilitating factors included assistance meeting basic needs (ie, housing, employment, food, and childcare). 20
Need: Barriers
Kushel et al 2 identified factors associated with health care services uses among 2974 homeless and marginally housed persons. Individuals with 1 or more comorbid conditions were more likely to report barriers to medical care than those with no medical comorbidities. 2
Need: Facilitators
Having more than 1 comorbid condition was associated with primary care use, as primary care use increased with every additional comorbid illness (1 comorbid condition, OR = 1.28; 95% CI = 0.53-3.12; 2 comorbid conditions, OR = 2.73; 95% CI = 0.89-8.43; 3 comorbid conditions, OR = 5.26; 95% CI = 0.53-19.83). 2 It is important to note that those with comorbid illnesses were also more likely to report barriers to care. 2 In a study to predict health services use, a greater need for medical care was identified as a facilitator for perceived need, and associated with having a regular source of care. 25
Utilization of Health Services
Free clinics were reported as the easiest location to receive medical care in a cross-sectional study to examine unmet health care needs among the homeless in Birmingham, Alabama. 19 In the survey, 86% of participants reported the inability to pay for care as a common barrier to obtaining health services. While having long wait times, free clinics provided gratis care and had less restrictive requirements when compared with county hospital clinics and EDs.
Consumer Satisfaction
Important factors in the experience of satisfaction of primary health care among the homeless was investigated in 1 study (n = 17). 21 Participants wanted health care providers that were committed to their care and engaged them respectfully. Also vital to satisfaction with care were interpersonal interactions that demonstrated empathy, sensitivity, and acceptance. Additional satisfaction care delivery factors that were critical included homeless persons having confidence and trust in their providers, as well as the knowledge that they would not be stereotyped or prejudged because of their housing situation.
Discussion
This review offers an overview of barriers and facilitators to primary care access for the homeless using the Equity of Access to Medical Care Framework (Table 2). At the organizational level, health care delivery systems tailored to meet the needs of the homeless, were the most successful in improving primary care access. Health insurance coverage, assistance meeting basic human needs, and having a regular source of care, facilitated primary care access, and reduced hospitalizations and ED use. Provider characteristics, such as demonstrating cultural sensitivity, were critical to patient satisfaction and the overall health care experience. However, the number of barriers to primary care access is particularly alarming, especially considering the vulnerability of the population. This review offers a glimpse into these barriers and facilitators experienced by this population.
Application of Equity of Access to Medical Care Framework to Barriers and Facilitators to Primary Care Access Among the Homeless.
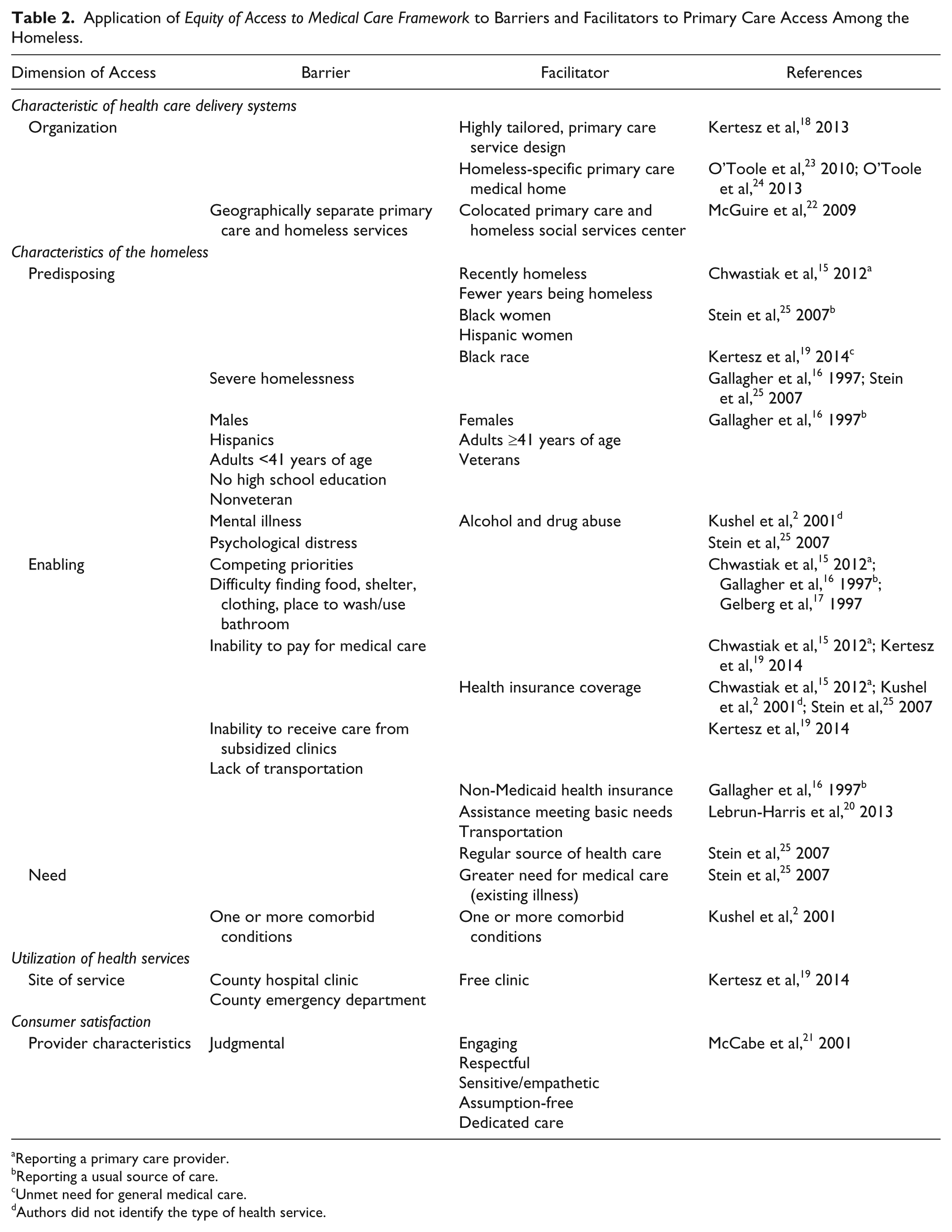
Reporting a primary care provider.
Reporting a usual source of care.
Unmet need for general medical care.
Authors did not identify the type of health service.
The homeless are the poorest of the poor and inherently a vulnerable population. They are at an increased risk for poor health outcomes because of a myriad of factors that increase their susceptibility to adverse events. Chronic psychological stress is unavoidable for homeless individuals. The feeling of powerlessness, uncertainty, and the lack of control of life events are major sources of psychological strain.27,28 Discrimination and social rejection are additional stressors experienced by the homeless, further isolating them from society and excluding them from the general public. 29 Chronic stress presents challenges in the management of chronic conditions, as well as, the promotion of overall well-being.30,31 Moreover, stress is a barrier to primary care access. 25 In conjunction with discrimination and isolation experiences, additional stress may negatively affect health seeking behavior in the health care setting. 32
Simultaneously, the homeless also encounter obstacles in obtaining adequate clothing, food, shelter, and transportation because of limited financial resources. The inability to acquire these basic needs has deleterious consequences on the health of this population. As several studies in the synthesis indicated, competing priorities are barriers to primary care access. Homeless individuals are more focused on meeting their physiological and safety needs, and may delay medical treatment, which exacerbates disease symptoms. To improve this population’s health, policy makers, health care providers, and public health practitioners must identify strategies to meet these needs. The articles presented in this review offer approaches to improve primary care access for the homeless. Strategies include health policy initiatives that increase access, the provision of culturally sensitive care, and the identification of subpopulations experiencing increased barriers to accessing primary care services.
Improving Health Policy Initiatives
There is limited research on policy-level processes that impede or promote primary care access among the homeless. Increasing the availability of affordable primary care services, when combined with other efforts, is unmistakably a needed policy that would increase primary care access. The policy expansion of Medicaid under the Patient Protection and Affordable Care Act has the potential of increasing primary care access among the homeless. 33 Medicaid expansion could increase health insurance coverage to previously unqualified homeless adults. 33 However, tailored outreach efforts need to occur at the organizational-level to identify and enroll homeless persons.
Health care coverage was a facilitator for primary care access in several studies included in the synthesis.2,15,25 Therefore, identifying uninsured homeless individuals and linking them with resources to obtain affordable care is essential. It is important to note that while several studies found that insurance can improve access to primary care services, a causal relationship does not exist. Gallagher et al 16 concluded homeless individuals with non-Medicaid insurance were the most likely to have a usual source of care; suggesting that those with Medicaid insurance had difficulty obtaining a usual source of care. Similarly, Johnson et al 34 found that the probability for being admitted to the ED for an ACS condition was highest among publicly insured patients in the general population. These findings further support that insurance alone does not increase access to health services, especially to primary care services.
As the framework illustrates, multiple factors may impede or facilitate primary care access. One such facilitator is the site where medical services are received. Homeless individuals indicated free clinics and safety net clinics, as the easiest sites to receive medical services. 19 Health policy determines funding amounts available to support these clinics. The Health Resources and Services Administration’s Health Care for the Homeless Program provides funding for several safety net health centers. 35 Since these clinics deliver tailored care to the homeless population, they have the potential to increase access to affordable primary care services. 36
Providing Culturally Sensitive Health Care
In addition to health policy initiatives, using tailored delivery models that provide culturally sensitive care can increase primary care access and improve patient satisfaction.18,23,24 Equity in access to primary care services is more than just the availability of primary care facilities. Delivery systems must promote equity and improve the quality of care delivered. Improvements are needed among patient–provider communication, a key variable in patient satisfaction. 18 Therefore, to provide quality care, providers must understand the unique needs of the homeless. Their needs are more complex than the general population and health provider characteristics influence whether homeless persons will use health services.21,37 If providers are not familiar with this population’s needs, or are not willing to meet their needs, this may impede health care use.
Improving interpersonal communication can facilitate primary care access and advance the quality of care in this population. Using “I” and “you” statements are one strategy to improve patient–provider communication with the homeless population by creating a welcoming and receptive environment without judgment. 37 Formal training for health care professionals that improve cultural understanding and awareness is another strategy to improve provider communication. 38 There are several existing curricula to improve provider knowledge of diverse groups such as the homeless, as well as attitudes and beliefs.
In addition, several studies have examined the need for culturally appropriate health care delivery models for the homeless.39-41 One such delivery model is medical respite care. This flexible care delivery model accommodates the needs of homeless people by providing shelter and continuous care. It also provides basic needs that act as competing priorities in more traditional delivery models. Medical respite care for the homeless increases access to health care services, and reduces hospital readmissions and hospital lengths of stay.40,41
Identifying At-Risk Subpopulations
Certain subpopulations of the homeless may have increased barriers to primary care services. This consequently results in worse health outcomes. Subpopulations included males, ethnic minorities, and individuals with a mental illness.2,16 Hospitalizations for ACS conditions have been used as a proxy measure for access when evaluations of primary care access were needed.5,36,42,43
Review findings indicate being male as a barrier to primary care access. 16 On the contrary, previous research found women have a higher probability for being admitted for an ACS condition, indicating that housed women have more barriers to primary care services than housed men.34,44 This disparity suggests homeless women may have access to additional resources that are unavailable to nonhomeless women. The majority of homeless families are headed by women, which may indirectly increase the number of available health-related resources. 45 Furthermore, homeless women with children may be gaining health care resources through Children’s Health Insurance Program or programs that are linked to family services.
Several studies have documented racial disparities in ACS hospitalizations in the general population. Trend analyses indicate ACS hospitalizations have been increasing among Black patients, especially for acute and preventable conditions such as urinary tract infections and dehydration.44,46 Johnson et al 34 determined the odds of being admitted through the ED for an ACS condition were the highest for Blacks and Hispanics. Other studies concluded being Black as a predictor for an ACS hospitalization when compared with Whites.47,48 These studies suggest that Black and Hispanic individuals have increased barriers to accessing primary care services than the general population.
Surprisingly, these reviewed studies ascertained Black and Hispanic homeless women 25 and Black homeless individuals 19 had fewer barriers to accessing primary care services compared to White homeless women or White homeless individuals. A study conducted in Los Angeles, California, found that while White homeless women had higher educational attainment than Black and Hispanic women (which is considered a facilitator to primary care access in the general population 49 ), they reported more barriers to medical care services. 25 A similar study maintained Black homeless persons were less likely to report unmet medical care needs when compared to White homeless persons. 19 Stein et al 25 speculated this racial disparity observed between the homeless and nonhomeless population may be related to mental illness. Black and Hispanic individuals may be homeless because of economic reasons (eg, unemployment, lack of affordable housing, extreme poverty) rather than mental illness, which may be the case for White individuals. White homeless persons have higher rates of hospitalizations for mental illness when compared to Blacks and Hispanics. 50 This presents 2 very different subpopulations within the homeless that have unique needs and barriers, primarily because mental illness is also a barrier to primary care access. 2
As previously discussed, a mental illness diagnosis impedes primary care access among the homeless and the general population. 2 In the housed population, patients with a coexisting mental illness have higher hospital admissions for ACS conditions compared with those without a mental illness, indicating reduced access to primary care services.51,52 Having a mental illness diagnosis appears to supersede being a racial/ethnic minority, which is often alone a barrier to primary care access.44,46-48
Future Directions
The positioning of health care as a human right is a central tenet of the framework. Primary care acts as a gateway to medical care by providing preventative and diagnostic services, linking individuals to additional health services, and improving overall physical and mental well-being. Based on this concept and the primary care purpose, the United States health care system is compelled to allocate resources ensuring vulnerable populations, such as the homeless who bear a disproportionate burden of illness, have access to quality primary care services.
The framework used in this review highlights key components and players in our health care system that can enhance access to primary care services among the homeless. Policy makers must allocate resources equitably to ensure the medical care needs of our most vulnerable and at-risk populations are being met. This entails evaluating the effect of health care policies and programs, such as the Affordable Care Act and the Health Care for the Homeless Program, on delivering quality health care to the homeless. Health care providers must ensure their practices are meeting the needs of the homeless. Developing, implementing, and evaluating “homeless-sensitive” care training programs are one step toward this direction. Our review indicates positive, interpersonal experiences in the health care setting are essential to improve the quality of care to the homeless. Furthermore, public health practitioners must develop interventions that address the unique characteristics of a homeless population (ie, providing basic human needs like shelter, food, and safety, to reduce barriers to medical care access). Delivering and evaluating these programs to meet homeless-specific needs is vital to enhance primary care access and improve overall health.
Study Limitations
Despite interesting findings, there are several limitations to this review. First was the potential for redundant sampling as 2 studies included in the review may have analyzed data from the same patient population at different time points.23,24 Second, 2 studies used having a usual source of care 16 and a primary care provider 15 as the primary outcome measure instead of actual health care utilization. Third, 3 studies focused on homeless veterans, a subpopulation that could have potentially different health care use patterns than homeless nonveterans.22-24 Despite the limitations, the findings of the review provide pertinent information with respect to understanding the barriers and facilitators of primary care access among the homeless.
Conclusion
The findings of this review suggest homeless people have significant challenges and barriers to obtaining primary care. Health policy initiatives, tailored health care delivery systems providing culturally-sensitive care, and targeted interventions can assist with overcoming these barriers. Future investigations of homeless barriers and facilitators to primary care access should focus on the impact of health policy changes. Quantitative and qualitative studies should be evaluated to determine the best strategies to enhance access and improve the quality of care. Understanding primary care access barriers and facilitators can assist in the development of evidence-based medical and public health practices, and policy decisions to improve health outcomes among the homeless.
Footnotes
Acknowledgements
The author would like to thank Kit N. Simpson, DrPH, for her feedback on the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.