
Abstract
Suicide is the third leading cause of death in Americans aged 15 to 24 years, with just under 4200 deaths in 2007 1 and an estimated 100 to 200 suicide attempts for every death. 2 In addition, about 1 million adolescents attempt suicide, and nearly 500 000 are admitted to psychiatric hospitals from emergency departments for suicide attempts or serious suicidal ideation each year. 2 Suicide leads to emotional and financial costs for patients, parents, and the treatment system. 3
Numerous organizations2,4-6 have identified primary care as an opportune setting to identify, triage, and provide brief intervention for suicidal youth. Primary care providers (PCPs) are uniquely positioned as gatekeepers because 70% of adolescents see a physician at least annually and are more willing to talk with medical staff about mental distress than with a “counselor.”7,8 In addition, empirical studies now support the value of screening for depression (commonly associated with suicide) in adolescents in primary care settings, and this practice is strongly encouraged by major medical and psychiatric associations.9-12 In fact, the Joint Commission on Accreditation of Healthcare Organizations now recommends that all patients receiving care in an accredited ambulatory setting should be assessed for suicide risk. 13 Despite the growing call for PCPs to incorporate suicide prevention in their practices, little is known about providers’ thoughts and practices regarding suicide.
To address this gap in the literature, PCPs across Pennsylvania were invited to complete a survey about current attitudes, practices, and barriers to assessing adolescent suicide risk and psychosocial problems more generally.14,15 This article provides a descriptive analysis of the data collected from the survey.
Methods
The survey consisted of 53-items focused on (1) demographics; (2) attitudes, knowledge, and comfort with general psychosocial and suicide screening; (3) current screening practices and barriers; and (4) satisfaction and barriers regarding making referrals to behavioral health services. In May 2009, a link to a Web-based questionnaire was sent to all members of the Pennsylvania Chapter of the American Academy of Pediatrics, the Pennsylvania Coalition of Nurse Practitioners, the Pennsylvania Academy of Family Physicians, and the Pennsylvania Association of Community Health Centers (N = 7577) via email requesting their participation in completing a questionnaire on mental health. No financial or other incentives were offered for participation. Each professional association was sent at least 3 reminder emails between May and July 2009. Responses were anonymous. The Institutional Review Board of The Children’s Hospital of Philadelphia approved the study.
Statistical Approach
Descriptive statistics (eg, frequency, percentage) were calculated for all items. Differences between groups were compared using analyses of variance and χ2 analyses. Logistic regression models were performed to determine factors associated with screening while controlling for relevant covariates.
Results
Characteristics of Sample
A total of 671 PCPs completed the survey (response rate = 8.9% of all receiving the email invitation to participate). Respondents were 74% female, with a mean age of 48.0 years. Just under half (49.3%) of respondents were medical doctors, 41.0% were nurse practitioners, and 6.1% were doctors of osteopathic medicine. Respondents had a mean of 17.6 years of professional experience and practiced in a variety of urban, suburban, and rural settings (see Table 1).
Characteristics of Sample a

Data are number (%) unless otherwise indicated.
Prevalence of Suicide Attempts, Ideation, and Behavior Encountered
Just over 40% (40.6%) of respondents reported having at least 1 adolescent patient attempt suicide in the past year, and 7.7% of those reported more than 6 adolescent patient suicide attempts in the past year. Nearly 69% (68.6%) reported seeing an adolescent patient with suicidal ideation in the past year, and 15.9% reported 6 or more adolescents in the past year with suicide ideation. There were no statistical differences in the number reporting suicide attempts between urban, suburban, and rural areas (n = 650):
Primary Care Provider Attitudes About Mental Health
Eighty-five percent (85.0%) of respondents agreed with the statement that addressing adolescent behavioral health problems is consistent with their philosophical approach to their professional practices. However, PCPs in urban settings were more likely to agree with this statement than were PCPs in rural settings: F2,629 = 3.429, P = .033.
Frequency of Screening for Mental Health Problems and Suicide Risk
Sixty-seven percent (67.1%) of PCPs reported screening their adolescent patients for general mental health problems at most well visits, whereas 27.1% reported screening for mental health problems rarely or only when suspected. The PCPs in urban settings (30.5%) screened at both well and sick visits for mental health problems more often than did those in suburban (19.7%; Tukey HSD = .192, P = .019) and rural settings (19.8%; Tukey HSD = .351, P < .001) (see Table 2). In contrast, only 25.4% of PCPs reported screening for suicide risk at most well visits, whereas 61.2% reported screening for suicide rarely or only when indicated. The PCPs in urban settings (47.6%) also reported screening specifically for suicide at well and/or well and sick visits more often than did PCPs practicing in both suburban (30.0%; Tukey HSD = .223, P = .003) and rural settings (31.4%; Tukey HSD = .232, P = .022). Only 14.2% of PCPs reported “often” or “always” using a standardized screening tool to assess suicide risk in adolescent patients.
Prevalence of Screening by Practice Setting a
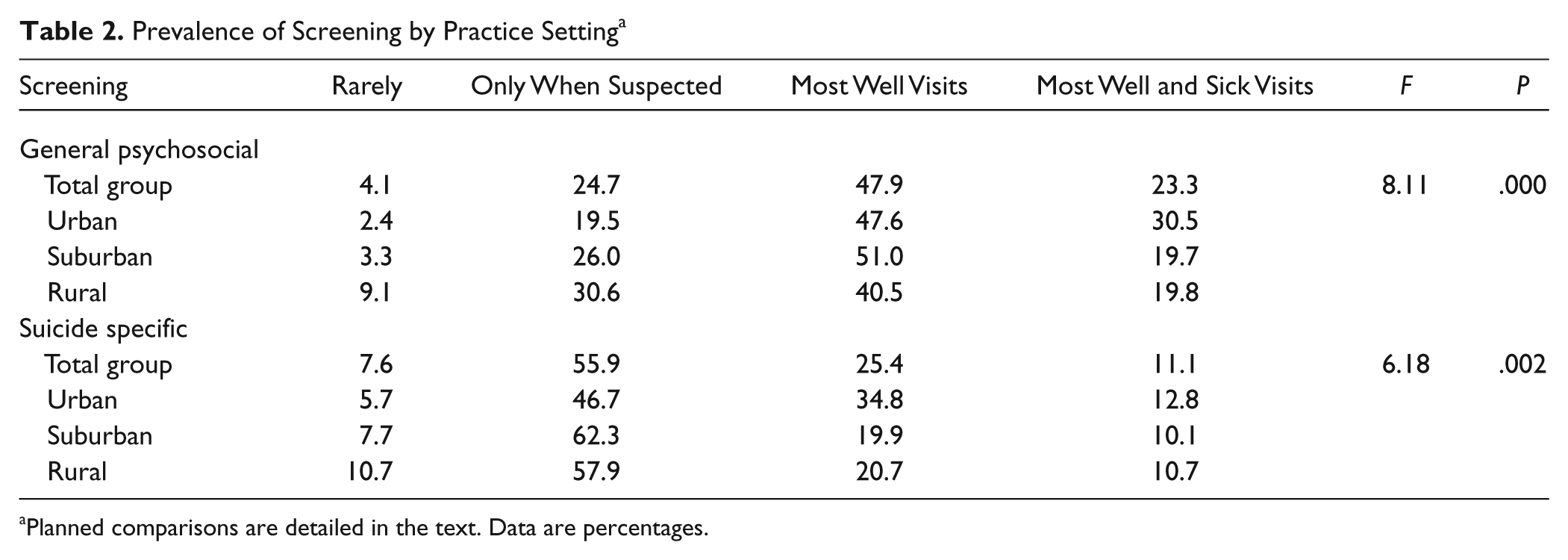
Planned comparisons are detailed in the text. Data are percentages.
Factors Associated With Screening for General Mental Health Problems
Table 3 lists the factors that significantly corresponded with whether a provider screens for general mental health problems. The PCPs who reported adequate knowledge in adolescent suicide risk assessment were nearly 5 times as likely to screen for mental health problems at both well and sick visits compared to those who reported a lack of knowledge in this area (odds ratio [OR],= 4.8; 95% confidence interval [CI], 2.9-8.0). Even when controlling for availability of behavioral health referrals, this finding remains significant (Wald = 32.67, P < .001). Female providers (OR, 3.7; 95% CI, 2.1-6.6) and providers in urban settings (OR, 3.2; 95% CI, 1.6-6.4) were significantly more likely to screen for mental health at well and sick visits. Finally, providers who reported having a suicidal adolescent patient in the past year were more likely to screen for mental health at well and sick visits (OR, 2.8; 95% CI, 1.6-4.8). This effect remained significant when controlling for availability of services and adequate knowledge (Wald = 4.37, P = .037), although adequate knowledge accounted for significantly more variance (Wald = 25.54, P < .001). Furthermore, availability of services was unrelated to frequency of mental health screening (F1 = 1.19, P = .28). In general, factors predicting screening for suicide were similar to those predicting screening for general mental health.
Factors Predicting Screening for General Mental Health and Suicide a

Reference category is rarely screening. CI, confidence interval; OR, odds ratio.
Perceived Barriers to Screening
Only 25.5% of respondents reported adequate training in adolescent suicide risk assessment, and 32.9% reported adequate knowledge in this area (see Figure 1). Despite low rates of training and knowledge, 64.2% of PCPs reported feeling comfortable talking with adolescents about suicide, and 58.4% reported feeling comfortable deciding which circumstances require breaking an adolescent’s confidentiality. Most PCPs (86.9%) believed there were no iatrogenic effects from talking with youth about suicide. More than half (54.6%) of the providers reported feeling undercompensated by insurance companies for treating behavioral health problems related to suicide. In fact, only 3.0% reported adequate compensation. Less than half (44.5%) agreed that PCPs frequently use physical health billing codes to reflect behavioral health services rendered. Time was cited as a barrier to suicide risk assessment by 32.8% of respondents.

Barriers to screening.
Referrals and Relationships With Mental Health Providers
Three quarters of PCPs (75.0%) reported referring at least 1 adolescent patient to behavioral health services in the past year for suicidal ideation or behavior, yet only 24.9% reported that they can always or often quickly get mental health service appointments for their suicidal patients. Furthermore, availability of services was unrelated to frequency of mental health screening (F1 = 1.19, P = .28). Although 68.3% of the sample prefer a psychiatrist (over other behavioral health providers) to perform the initial assessment and medication prescription for suicidal adolescents, most PCPs (61.4%) did not report preference for a psychiatrist to provide ongoing treatment for suicidal adolescent patients. Most PCPs reported that patients attended behavioral health services after a referral (43.2% often or always; 44.1% sometimes). Only 10.9% of PCPs reported that their adolescent patients attended behavioral health services without the help of their parents. Few (21.9%) always or often heard back from behavioral health providers after a referral was made.
Discussion
The most significant finding in this study is that 40% of PCP respondents reported treating an adolescent who attempted suicide in the past year, and nearly 70% reported seeing patients with suicidal ideation. These prevalence rates are consistent with previous findings. 16 Although the recent emphasis has been on depression screening in primary care,9-11 these data suggest expanding best practice guidelines to include suicide screening as a required or, at least, encouraged domain for assessment in primary care. In addition, suicide risk spans numerous health conditions and can present without depression. 17 Thus, only screening for depression may not be adequate to identify this high-risk population.
In this sample, having contact with a suicidal patient was associated with increased screening for suicide. This experience may motivate PCPs to screen, or PCPs who screen more may identify more suicidal youth. Similarly, knowledge about suicide risk assessment was associated with increased screening for suicide general mental health risk. Although the direction of causality cannot be determined from the data, other studies have suggested that PCP training in suicide risk assessment increases screening and detection.18,19
One way to promote suicide screening would be to incorporate it into depression screening. Coupling suicide assessment with depression assessment makes sense clinically and improves efficiency. Unfortunately, the recommended depression screening tools offered by the US Preventive Services Task Force, 10 the Beck Depression Inventory–Fast Screen and the Patient Health Questionnaire (PHQ-9), do not have adequate suicide items. More broad-based screening tools, like the Web-based Behavioral Health Screen, 20 include both depression and suicide items, thus make screening more thorough and effective.
We found that providers in urban settings were more likely to screen for both general mental health and suicide risk than were providers in other practice locations. Although greater service availability may account for this, availability of behavioral health services did not predict screening nor did it account for the relationship between provider knowledge and screening. Thus, PCPs’ decisions to screen patients seem more related to their knowledge of mental health issues and their experience with these patients.
Finally, barriers must be considered from a policy level. Clearly, the most endorsed barrier to screening was lack of reimbursement. Depression screening in primary care often results in significant increases in provider’s financially uncompensated time with patients. 21 We found that many PCPs billed for mental heath under physical health codes. Advocacy for reimbursement for the suicide screening must continue at the national and state level for Medicaid and with private insurance companies. Besides saving lives, early identification of suicidal youth can prevent costly emergency department and hospital admissions. For Medicaid patients procedure codes for mental health screening have been approved, but reimbursement remains uncommon.
It should be noted that although the sample size is large (671), the low response rate (8.9%) is a limitation of this study. Unfortunately, this comprehensive survey consisted of 53 questions that took about 12 minutes to complete—a significant time investment for this busy community of providers. Thus, PCPs who completed this survey may be those most concerned about mental health needs. However, if in a highly motivated group of PCPs only 23.3% universally screen for mental health problems, 11.1% universally screen for suicide risk, and 14.2% routinely use standardized screening tools, then it is likely that these rates are much lower in the general population of providers.
Conclusion
Despite recent recommendations for increased screening for depression and suicidal symptoms in primary care,9,10 few providers follow these recommendations. Barriers are many, including limited knowledge about suicide risk, lack of reimbursement for screening, and poor availability of behavioral health services. Even when funding is available to provide free training, there is access to a Web-based screening tool, and facilitated linkages with behavioral health providers are available, behavioral change in PCPs is slow. Such has been the case with Pennsylvania’s youth suicide prevention project in primary care. 22 Many providers welcome such change but acknowledge that policy change supporting reimbursement may be the primary factor prohibiting a rapid and much needed integration of services.
Footnotes
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors received no financial support for the research, authorship, and/or publication of this article.