
Abstract
Introduction:
Given the increase in youth mental health concerns, the American Academy of Pediatrics (AAP) recommends universal suicide screening for ages 12 and older, with positive screens followed by a brief suicide risk assessment. However, it is unclear how pediatric clinicians incorporate this recommendation into practice. Therefore, the objective of this qualitative study was to identify pediatric clinicians’ current practice, attitudes, and barriers to implement the updated universal suicide screening recommendation in primary care.
Methods:
Community-based pediatric primary care providers (PCPs) in the St. Louis Metropolitan area who by self-report provide mental health care for patients participated. Participants completed a 30-minute semi-structured interview with invitations extended through an electronic listserv in a local Pediatric PCP Learning Collaborative. Interviews were transcribed and analyzed using consensual deductive and inductive approaches until data saturation.
Results:
Eighteen PCPs participated in the interviews. Interviews described themes related to acceptability of the recommendations, PCPs’ current screening practices, and perceived barriers for implementing the recommendations. Overall, PCPs agreed with, but expressed hesitancy about, the recommendation. Frequently mentioned barriers to suicide screening included time, training, and inadequate access to resources for follow-up care for at-risk patients. Yet, PCPs were optimistic they could learn with support and were interested in working in this subject area through quality improvement interventions.
Conclusions:
PCPs agree with the AAP recommendation about suicide screening but need support to implement into practice. Specifically, PCPs need time sensitive strategies, resources, training, and practice change support to assist these efforts.
Introduction
Suicide is the second leading cause of death in adolescence. 1 While mental health has long been a concern for adolescents, mental health needs during and after the COVID-19 pandemic continue to increase.2 -4 Given this distress for children and families, the American Academy of Pediatrics (AAP), the American Academy of Child and Adolescent Psychiatry, and the Children’s Hospital Association declared a national emergency in children’s mental health. 5 This state of emergency was reflected in mounting Emergency Department (ED) visits for behavioral health concerns and was also described locally by community pediatricians.2,6 With national shortages of child and adolescent psychiatrists, pediatric clinicians need to be prepared to assist children, youth, and families with care for depression and anxiety, suicide risk screening, and suicide risk assessment. 7 This is especially pertinent as nearly 80% of people who died by suicide, including all age demographics, had contact with a health care provider within a year of their death. 8 An AAP survey also indicated that suicide risk is frequently encountered in pediatric practice. 9 As such, healthcare settings are important locations for screening to occur.
Recognizing the crisis of growing youth suicides and limited access to mental health providers, the AAP with the American Foundation for Suicide Prevention released the Blueprint for Youth Suicide Prevention as a resource to help pediatric clinicians identify, assess, and prevent youth suicide. 10 In concert with that release, the 2022 AAP Bright Futures Recommendation called for universal suicide risk screening for those 12 and above with a validated suicide risk screening tool, no more than once a month and no less than once a year. 11 The Blueprint goes on to recommend that positive screens are followed by a brief suicide risk assessment and then safety planning. While the Blueprint is filled with helpful information and tools, it is unclear if pediatricians can easily implement these recommendations into primary care practice. A study with 1 primary care practice bridged this gap between recommendation and implementation using a quality improvement (QI) process to implement a suicide risk screening pathway and found it feasible and acceptable. 12 Another study using screening data from over 90 000 patient encounters also demonstrated the feasibility of implementing universal suicide screening in a large hospital system. 13 Further implementation science efforts to expand this care, train more pediatric clinicians, and build systems in primary care practice are urgently needed. 14
A first step in developing a system for pediatric clinicians to implement the suicide prevention guideline is to assess the current state of practice, attitudes about the recommendation, and concerns around implementing this recommendation. 15 Therefore, the objective of this qualitative study was 2-fold: (1) better understand clinicians’ attitudes and approaches to suicide screening in pediatric primary care and (2) identify barriers to pediatric clinicians implementing suicide screening in primary care. By identifying current practices and perceived barriers, this work may inform future interventions to improve suicide screening, assessment, and management processes in practice.
Methods
Eligible participants were community-based pediatric primary care providers (PCPs) in the greater St. Louis Metropolitan area who self-reported that they treat patients for mental health concerns. Invitations to participants were extended through an electronic listserv in a local Pediatric PCP Learning Collaborative. 16 This collaborative began as a practice-based research network (PBRN) and now consists of over 60 community pediatric practices that serve over 175 000 patients in the greater St. Louis metropolitan area. The collaborative disseminates information, resources, and opportunities among members to improve child health and well-being. PCPs participated by completing a single 30-minute semi-structured interview. The local Institutional Review Board deemed the study to be exempt.
After reviewing relevant literature, an interview guide was drafted by the study team to assess current practice for: (1) identification and management of patients at risk of suicide and (2) providers’ attitudes about the AAP universal suicide risk screening recommendation. The interview included 8 open-ended questions about suicide risk screening, how PCPs determine safety, their confidence in managing patients with suicidal thoughts, barriers to implementing universal suicide screening, and potential quality improvement projects of interest. Questions for the semi-structured interview are listed in Table 1.
Questions Used in the Semi-Structured Interviews.

Participants completed the 30-minute virtual video interview between April 26, 2022 and June 14, 2022. Interviews were conducted by the PBRN coordinator, audio-recorded and transcribed verbatim by Landmark Associates. 17 Demographic data was collected, and participants received a $50 gift card for participating.
The research team (LE, SR, EL, AS) analyzed the transcribed interviews using both deductive and inductive qualitative coding techniques. A deductive codebook was developed prior to analysis to define initial codes associated with items from the interview guide. At least 2 research team members analyzed each transcript manually, line-by-line, with deductive coding strategies to identify the text units associated with each question. 18 After this, for each transcript, 2 different analysts then categorized each text unit by assigning a code defined in the preliminary codebook. Text units that were not associated with the primary codebook domains were isolated and inductively analyzed by grouping semantically related text units together and creating new codes. This ensured adequate coverage of all concepts in the interviews, and the codebook was revised to include the new codes. Notably, at each level of this iterative analysis (eg, identifying text units, assigning codes), the research team analyzed each transcript separately then reviewed discrepancies and came to agreement based on group discussions. After all transcripts were assigned codes, 2 analysts re-coded each transcript using the revised hierarchical coding frame. Data saturation was achieved.
Results
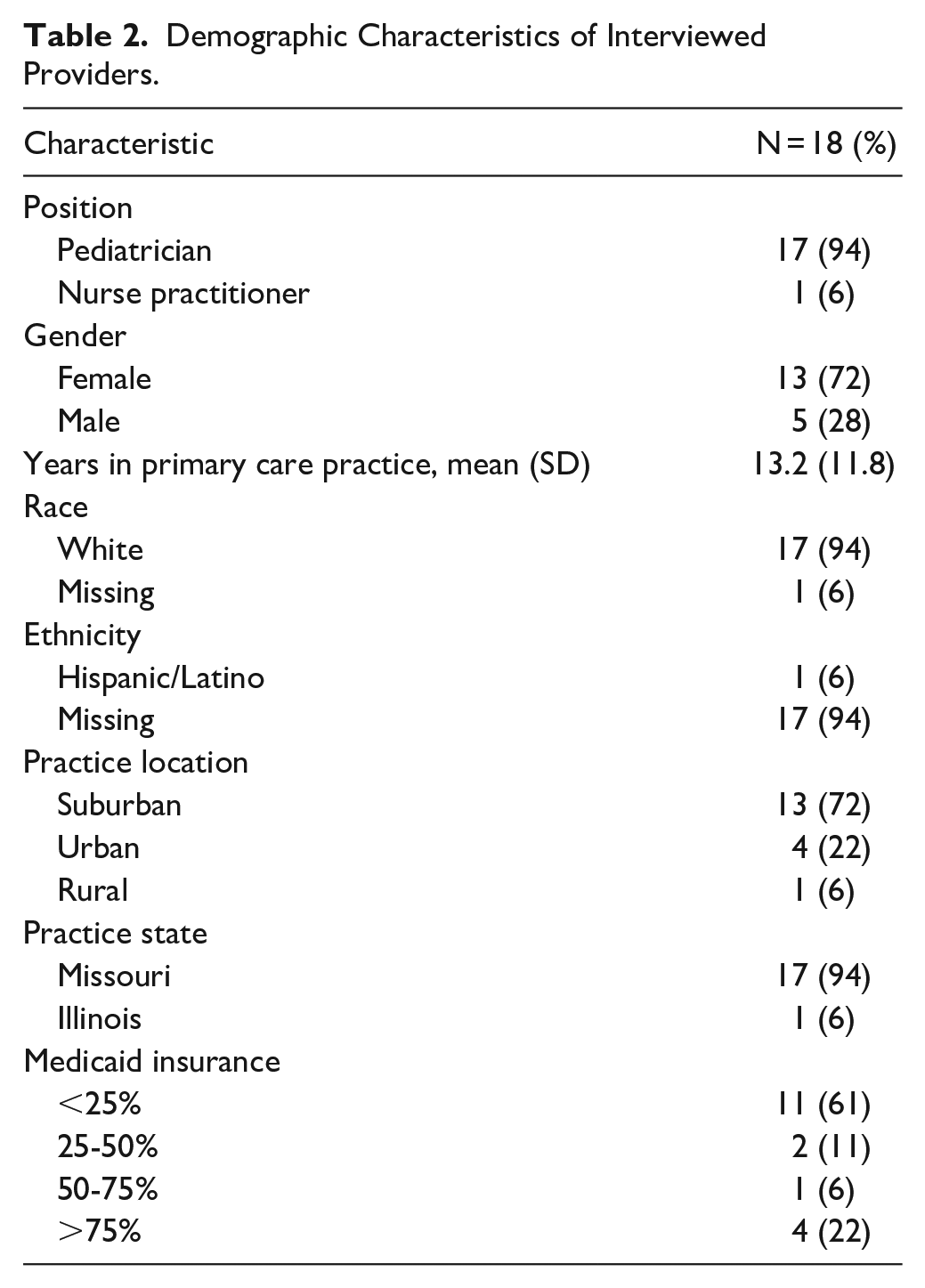
A convenience sample of 18 PCPs volunteered to participate in the semi-structured interview. Interviewed participants had a mean experience in primary care of 13.2 years. They covered the St. Louis Metropolitan area and represented mostly suburban practices (n = 13). These PCPs serve a mix of privately and publicly funded patients: 11 (61%) worked in practices that served a patient population with less than 25% Medicaid, and 7 (39%) worked in practices that served a patient population with greater than 25% Medicaid. Four providers (22%) served mostly Medicaid populations of children. See Table 2 for provider demographics. Missouri ranks 28th among state youth suicide rates with 12.5 per 100 000 deaths by suicide in 15- to 19-year-olds and above the national average of 10.6 per 100 000. 19
Demographic Characteristics of Interviewed Providers.
Six analytical themes were developed from the interviews: acceptability of suicide risk screening (Theme 1), varied screening tool use (Theme 2), provider safety assessment and decision-making (Theme 3), uncertainty in managing suicide risk (Theme 4), systemic barriers to suicide risk screening implementation (Theme 5), and willingness to engage in implementation work (Theme 6). See Table 3 for illustrative quotes.
Pediatric Clinician Interview Themes and Illustrative Quotes.

First, PCPs agree with the new AAP recommendation for universal suicide risk screening for those age 12 and up (Theme 1). This is demonstrated by a quotation from a PCP:
Oh, I think it’s probably a good recommendation. I would agree ’cause I’m sure, of all the ones I know about, I’m probably only seeing the tip of the iceberg.
While PCPs expressed agreement, there was also considerable ambivalence about implementing the recommendation in practice:
I agree with the recommendation, and I also would like the AAP to come spend a week with me and tell me where I’m supposed to get that done It’s hard being the pediatrician ‘cause you’re the frontline for everything.
Additionally, our interviews reflected a variety of screening practices (Theme 2) including clinical judgment and 1 validated screener, the Ask Suicide Screening Questions (ASQ). One example of clinical judgment being used in practice is expressed below:
I have a relationship with all these people. I’ve been takin’ care of most of them since they were born. I know them. Hopefully, I have a relationship with ’em enough to be able to glean some of the aspects that would contribute to their situation.
Several PCPs also spoke about the value of using validated screeners such as the ASQ when assessing their patients20
-22:
By adding that ASQ onto the bottom of the PHQ-9, you might catch those anxiety kids that would be at risk for suicide and still be doing your depression screen.
23
The Blueprint recommends using validated tools such as the ASQ, C-SSRS, and the Suicide Behavior Questionnaire-Revised.
11
Although the providers specifically mentioned using the ASQ, no other suicide risk screeners were mentioned. When assessing the safety of patients with suicide risk (Theme 3) most PCPs ask about suicide-related safety factors. One quote from a PCP demonstrates this process:
. . . for the parents, I talk to them about keeping them safe, about making sure anything in the house that could be a danger to the child or teen is locked up and out of their reach. . . truthfully, if I feel like they’re not gonna be safe ever alone, I’m typically sending them in at that point because it’s not practical for them to be alone.
Referral to other health care settings specialized for behavioral health concerns is frequently mentioned as a strategy for managing patients who screen positive for suicide risk. Pediatric providers also articulate limitations in their ability to provide quality care for these mental health concerns:
I’m able to give them resources and like, “This is where you can go. . .” besides doing a safety plan of talkin’ to parents about getting weapons out of the home. . . Then, pointing them to the resources we have, but other than that, I don’t really—I don’t have anything else really to offer.
Furthermore, although most PCPs agreed with the recommendation, many were uncertain about implementing suicide screening protocols and managing patients with suicidal thoughts in practice (Theme 4). This ambivalence is highlighted in the following quotations where PCPs ranked their confidence on a 1 to 10 scale (ie, 1—low confidence, 10—high confidence; see Table 1):
Five. . .I mean, the reality is, how does anybody feel confident? Low, less than five because I just feel like they need more help than what I can give them seeing them monthly or every three months
Even some PCPs who expressed high confidence in managing these patients expressed concerns about long-term follow-up and a lack of resources:
I would probably say an eight or a nine just because of the lack of inpatient resources and the delays in therapy. . .
PCPs also discussed systemic barriers to suicide risk screening implementation, which included time and worries about resources (Theme 5). Time-related constraints were consistent barriers discussed in the interviews including completing screening and time to manage those at increased risk, as illustrated by the following quotation:
I have to tell you, a lot of this is it’s not due to lack of interest or lack of compassion, it’s purely lack of time. Anything that takes an additional 45 seconds out of my day is something that I can’t repeat throughout the day, otherwise, I’m gonna be working till 9:00 p.m. and just can’t survive it.
Moreover, PCPs also frequently mentioned the lack of training to deal with mental health and suicide-related concerns as a potential barrier to implementing universal suicide screening, which is suggested in the following quotation:
I think with suicidality—even with these tools, I just don’t feel that comfortable about it, because I wasn’t trained to handle it right?’
PCPs further discussed how their concerns for managing complex mental health cases are exacerbated by resources, like urgent mental health assessments and faster therapy appointments, not being available. One frequent barrier acknowledged was having nowhere to send the patient when the screening was positive. Participants expressed this concern and frustration when considering what to do next:
What do you want me to do with that? Oh, let’s open this jar of worms and then—I can’t take ‘em home with me. They can’t stay here in the clinic.
Lastly, although PCPs described many barriers to implementing the screening recommendation, they were optimistic they could learn to operationalize suicide screening with support (Theme 6). The following quotation indicates a PCP’s enthusiasm about possible QI projects:
I personally could use some improvement. . . just because I don’t know that we get as much direct training in that. That sounds like potentially a way to sort of streamline identification of kids who are acutely in crisis and need an intervention today versus kids that I can at least try to get parents to come back sometime in the near future. . . . Like I said, more accessibility, more opportunities for us to learn in a easier way. . .
Another PCP concisely described their interest in implementation participation as something beneficial for their practice as a whole, stating:
I think if we can find a way to make that easy for us to offer in the practice, for me, that’s wonderful.
When asked specifically about where PCPs would want to start with QI projects, a variety of responses were obtained ranging from the nonspecific desire to improve as stated above to more specific thoughts around the 3 Blueprint elements of universal screening, brief risk assessment, and safety planning.
I would do the brief. I just would wanna make sure everybody—do we screen everybody universally, and then the at-risk gets the brief? I would be interested in that. . . [T]he order of preference would be a universal suicide risk assessment or screening for all youth over 12, then the safety assessment. ’Cause I think that screening kids for suicide who are depressed leaves out the chunk of kids who may be suicidal and not depressed.
Discussion
This study describes a qualitative approach with interview responses from local pediatric primary care providers on universal suicide risk screening given the new AAP universal suicide screening recommendation. This assessment of attitudes, current state, and challenges, may assist the implementation of interventions so broader suicide risk screening dissemination occurs.
Agreement about the need for pediatric clinicians to screen in this way was reinforced, however clinicians in these practices named barriers and concerns to implementing suicide screening. Notable barriers identified were the lack of time to perform suicide risk screening, subsequent risk assessment, and management of those at increased risk within the time constraints of primary care practice.
When evaluating the current state of suicide risk assessment strategies and techniques, there was a wide variety of practice from clinical judgment to using validated tools. The AAP recommendation supports the use of validated suicide risk screeners, so training and supporting pediatric clinicians to use these screeners may be a potential area for QI work. 10
Barriers to implement this universal screening recommendation include structural factors, such as time, resources, and training. Providers are concerned about the next steps for patients screened as high risk, both in terms of time to further assess, but also whether there are mental health professionals available to quickly see those with increased risk. Moreover, there seems to be training and support needed around the safety risk assessment. This discernment of risk level takes time, training, and practice. All these concerns are highlighted in our interviews and may contribute to uncertainty and lower confidence in managing these patients. However, participants recognized they need training, and the majority were optimistic they could learn and wanted to work on QI projects in this area.
A plausible way to address these barriers and improve efficiency when implementing the AAP guideline is practice facilitation, an intervention strategy that supports practice change and builds capacity to improve outcomes.24,25 One PBRN has successfully utilized practice facilitation to improve depression care and treatment. 26 The trained facilitators work with the practices to establish QI goals, share data, offer support, and coach practices on how to make the strategies work in a particular practice to achieve desired patient outcomes.
Another concept from implementation science called human-centered design may also provide solutions to address the lack of time. Elements of human-centered design include: a needs assessment, intervention development with user feedback, and intervention testing in practice with iterations. 15 Additional potential time-saving methods (such as implementing tablet-based screening or using electronic health record platforms) may be components of these interventions. 27 More implementation work in this area still needs to be done and the complexity of implementation in clinical settings beyond education and training clinicians must be further studied as the transition from evidence to practice is often long and incomplete, taking nearly 17 years for only 14% of the research to be implemented in practice.28,29
In addition, reimbursement policy changes for time spent in screening, risk assessment, and safety planning, as well as recent International Classification of Diseases (ICD-10) time-based codes, may also help. Ultimately, successful interventions may change current workflow, time, and reimbursement models for suicide screening to occur in keeping with the AAP recommendations.
Several limitations of our study should be considered. Participants were a small, relatively non-diverse convenience sample of local volunteers from 1 Midwestern metropolitan area and interview questions were limited. The questions were not pilot tested, and questions related to facilitators of screening were not asked in the interviews. The research team is also well known to many participants, which might influence responses. Additionally, the self-reported criteria that they treat patients for mental health concerns was not more specifically defined, namely no measure recorded frequency or types of mental healthcare provided by each participant. As such, our findings may not be generalizable to all PCPs in our community or to PCPs in other locations.
Conclusion
Using a qualitative approach, this study identified agreement on the need for suicide screening consistent with the AAP guidelines among pediatric clinician participants. However, given these interviews, training pediatricians is not enough; they will need help designing systems within their practice to make this kind of screening work in ways that are practical. What the screening, risk assessment, and safety planning process should look like in pediatric practice, and how to help those adolescents with positive results, needs greater attention to make it feasible, acceptable, and actionable. Next steps for this work includes: (1) gaining more perspectives on suicide screening from parents, community members, and adolescents; (2) designing an intervention to promote adherence to the guideline while attending to time, workflow, and patients’ and families’ needs; and (3) using practice facilitation to implement the designed intervention. This sequence offers clinicians support and resources in ways compatible with their practice and acknowledges the learnings from these interviews. Galvanizing pediatric clinicians’ desire to learn and help adolescents in this area holds great promise for better health outcomes.
Footnotes
Acknowledgements
The authors wish to thank all the participating clinicians. In addition, we thank our WU PAARC advisory group for their care, attention, and support including: Dr. Randy Sterkel, Dr. Sandeep Rohatgi, and Dr. Stephanie Fritz.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Washington University Institute of Clinical and Translational Sciences grant UL1TR002345 from the National Center for Advancing Translational Sciences (NCATS) of the National Institutes of Health (NIH). Additional funding was provided by the St. Louis Children’s Hospital Foundation grant PR2019747.