
Abstract
Background:
Suicide is a leading cause of death worldwide. However, data on adolescent suicidal ideation remains limited in rural Bangladesh.
Objective:
This study identifies the prevalence and associated factors of suicidal ideation among adolescents in rural southern Bangladesh.
Method:
A cross-sectional study was conducted among 500 school-going adolescents in a southern rural subdistrict in Bangladesh. Data were collected using the Suicidal Behaviors Questionnaire-Revised.
Result:
The lifetime prevalence of suicidal ideation was 20.2% (n = 101; 95% CI: 16.9%–24.0%), and the prevalence in the past 12 months was 19.6% (n = 98; 95% CI: 16.3%–23.3%). The prevalence of suicidal attempts was 8.8% (n = 44, 95% CI: 6.6%–11.6%). Associated factors included being ever-married (Adjusted Odds Ratio (AOR): 6.9; 95% CI: 1.4–33.2; p = 0.016), excessive internet use (AOR: 4.3; 95% CI: 1.1–16.3; p = 0.033), lack of close friendships (AOR: 3.3; 95% CI: 1.2–8.8; p = 0.017), poor family relationships (AOR: 3.1; 95% CI: 1.3–7.2; p = 0.011), and moderate (AOR: 5.9; 95% CI: 2.2–15.9; p ⩽ 0.001), severe (AOR: 8.4; 95% CI: 2.2–34.4; p = 0.003), and extremely severe (AOR: 11.6; 95% CI: 2.6–52.4; p = 0.001) depressive symptoms.
Conclusion:
These study findings can help design effective strategies to prevent suicide and enhance adolescent mental well-being.
Introduction
Approximately 746,000 global individuals died by suicide in 2021. 1 Suicide is one of the four leading causes of death among individuals aged 15–29 years. 2 The prevalence of suicide is 3.8 per 100,000 population worldwide. 3
Around 77% of suicides occur in low- and middle-income countries (LMICs). 2 The prevalence of suicidal ideation (SI) is 14% among 12–17-year-old adolescents in these countries, with higher rates observed in Africa (21%) compared to Asia (8%). 4 The average rate of suicide in South Asian regions is higher than the global average. 5
Bangladesh is a lower-middle-income country in South Asia. 6 The suicidal mortality rate in Bangladesh is 3.08/100,000 population, which has been increasing since 2018. 7 The prevalence of suicide is comparatively higher in rural areas than in urban areas. A study conducted before the COVID-19 pandemic identified a 20.1% (95% CI: 12.6–31.7) prevalence of SI among rural adolescents in Bangladesh. 8 Adolescents aged 10–19 years are vulnerable to multiple risk behaviors, including substance use (tobacco, alcohol, drugs), self-harm, depressive symptoms, aggressive behavior, and involvement in risky sexual activities. 9 With the increasing age in adolescence, communication with peers often becomes easier than with parents, which may contribute to emotional distress and increased substance use 10 and eventually, increases the risk of SI.
A study conducted in 2013 reported a 5% lifetime prevalence of SI among rural Bangladeshi adolescents aged 14–19 years. Associated factors included age, occupation, education level, living with parents, and housing conditions. 11 Another study using Global School-based Health Survey data identified an 11.7% prevalence of suicidal behavior among school-going adolescents, with risk factors including loneliness, bullying, lack of close friends, anxiety, substance use, sexual activity, parental neglect in homework checking, and poor peer support. 12 However, these studies were conducted before COVID-19. The pandemic has brought significant changes among Bangladeshi adolescents, such as increased school dropout rates and early marriages 13 —which may impact adolescent mental health.
Mental health issues are often neglected in Bangladesh. 14 Lack of education, awareness, and social support restricts people from seeking psychological care. Adolescent mental health data are limited in the government database. Although several studies explored suicidality, they either focused on university students or were conducted before the pandemic, leaving a gap in understanding the current burden among adolescents. This study aims to assess the prevalence and associated factors of SI among adolescents aged 11–17 in rural southern Bangladesh. Updated knowledge on the prevalence and risk factors may inform targeted policies and interventions to prevent suicide and promote adolescent mental well-being.
Method
Study design
A cross-sectional study was conducted from April 15 to May 14, 2024, in 3 secondary schools in Lohagara, a rural subdistrict of Narail in southern Bangladesh. Approximately 829,000 people reside in Narail, while one-third of them live in Lohagara. 7 The population density is 871.98 sq/m2, and the literacy rate is 74.5%. 15 There are 49 government healthcare facilities, as in most southern subdistricts in Bangladesh. 16 It is predominantly a rural subdistrict, where adolescent mental health coverage is limited.
Study participants
The target population was adolescents aged 11–17 years residing in Lohagara. The study sample included students enrolled in one government and two non-government secondary schools within the subdistrict.
Sample size
Based on a reported 11.7% prevalence of suicidal behavior among adolescents in Bangladesh, 12 a 95% confidence level, and a 4% margin of error,

A total of 500 data points were collected using a two-stage cluster sampling technique to minimize selection bias and to account for potential design effect and intra-cluster correlation. We used a larger sample size to compensate for any loss of precision due to clustering and maintain statistical power. First, we selected 3 of the 34 schools in Lohagara by simple random sampling. In Bangladesh, secondary schools typically consist of six academic levels—classes Ⅵ–Ⅹ, along with a class for Secondary School Certificate examination candidates. Each class is divided into 3 sections, and each section comprises approximately 50–60 students. For this study, 4 sections from the government school and 3 from each non-government school were selected using simple random sampling. All students of the selected classes were invited to participate. Non-residents, students with cognitive impairments, and those unwilling to participate were excluded. Participants taking medications for mental health disorders were also excluded to minimize confounding, as psychotropic medications might influence mood and behavior and could initiate SI, Figure 1.

Participant recruitment process. Exclusion criteria: 1. Non-resident, 2. Cognitive impairment, 3. Taking psychotic medications, 4. Unwilling to participate, 5. Failed to provide consent.
Data collection tools
We assessed SI using the Suicidal Behavior Questionnaire-Revised, a validated and reliable tool with 4 items and a total score ranging from 3 to 18. 17 The Bengali translated version of this questionnaire was used to assess suicidal behavior in some studies, and the validity and reliability were established in previous studies.18–21 A score of 2 or higher on the first item indicated lifetime SI, while the second item assessed SI within the past 12 months. 17 No pilot studies were conducted.
The Depression, Anxiety, and Stress Scale-21 Items (DASS-21) was used to evaluate the presence and severity of depression, anxiety, and stress.22,23 The validity and reliability of the translated version were tested in previous studies.24,25 This questionnaire comprises 21 items divided into 3 subscales (seven items each). Responses were recorded on a 4-point scale ranging from 0 (“Did not apply to me at all”) to 3 (“Applied to me very much or most of the time”). Subscale scores were summed and multiplied by 2 to obtain the final scores for each domain.26,27 Data collectors received prior training on suicidal risk identification, basic mental health counselling and first aid, and appropriate response procedures on maintaining participants’ safety and confidentiality. Participants identified with symptoms of mental health disorders or SI had the school authorities and their parents or legal guardians promptly informed. We advised the guardians to consult a psychiatrist for their children, provided them with relevant contact information, and referred them to the nearest primary care facility.
We used another structured questionnaire to collect individual, interpersonal, institutional, community-level, and psychological information. We adopted the Socio-Ecological Model to guide our conceptual framework. This model suggests that suicidal behavior is influenced by a broader range of factors in individual, interpersonal, institutional, community, and societal domains. 28 All questionnaires were translated into Bengali to ensure clarity and effective communication with participants.
Data management and analysis
We analyzed data using STATA version 17 (StataCorp LLC, College Station, TX, USA). The dependent variable was lifetime SI. Univariate logistic regression was conducted to identify crude odds ratios (CORs). Variables with p < 0.2 were selected for multivariate logistic regression to adjust for potential confounders. Both crude and adjusted odds ratios, along with their 95% confidence intervals (CIs), indicated the strength of associations. A p-value < 0.05 was considered statistically significant. Missing values were minimal (maximum 7.6% for one variable). Therefore, we conducted the analysis using available case data.
Result
Individual level
A total of 500 responses were collected. The majority of participants (64.6%, n = 323) were aged from 14 to 17 years. About half of the respondents (51.3%, n = 255) were females. We determined socioeconomic status by monthly family income, homeownership, and parental occupations. Each indicator reflecting disadvantage was assigned a score (low family income = 1, no homeownership = 1, unskilled or unemployed parents = 1). The total score ranged from 0 to 3. Scores of 0 to 1 indicated high socioeconomic status, while 2 and 3 indicated medium and low socioeconomic status, respectively. Nearly half of the participants (47.6%, n = 238) were classified with medium socioeconomic status. Most participants (85.4%, n = 426) identified as Muslim. A small proportion (4.3%, n = 20) were engaged in part-time employment in addition to their studies. Additionally, 3.2% (n = 16) were married at least once. Among the participants, 2% (n = 10) reported smoking cigarettes, while no one provided information regarding other substance use. Approximately 4.6% (n = 23) were classified as extreme internet users, spending more than 16 h online per day. Nearly half of the respondents (49.3%, n = 242) reported regular participation in extracurricular activities, Table 1.
Baseline characteristics of adolescents aged 11–17 years (n = 500).

Interpersonal level
Among the participants, 44.9% (n = 210) belonged to large families. The majority (78.4%, n = 388) lived with both parents, while 8.0% (n = 40) reported having step-parents. Approximately 22% (n = 110) reported a poor relationship with their parents, while 24.1% (n = 120) reported conflict among family members. Parental negligence in checking academic performance was noted by 1.2% (n = 6). About 3.8% (n = 19) experienced severe domestic violence, and 4.8% (n = 24) indicated a family history of suicide or SA. Approximately 11.9% (n = 59) reported lacking close friends. Peer conflict was reported by 29.6% (n = 147) and 42.5% (n = 212) experienced peer isolation, Table 1.
Institutional level
Around 12.8% (n = 64) reported having severe academic stress, while 37.3% (n = 186) were dissatisfied with their academic performance. Most of the students (92.5%, n = 458) perceived their teachers as supportive, Table 1.
Community level
Around 16.5% (n = 82) of respondents experienced bullying by classmates, teachers, family members, relatives, or neighbors. About 12.6% (n = 62) reported that their parents did not own a house. Half of the students (52.1%, n = 254) reported their monthly family income was more than 20,000 BDT, Table 1.
Psychological characteristics
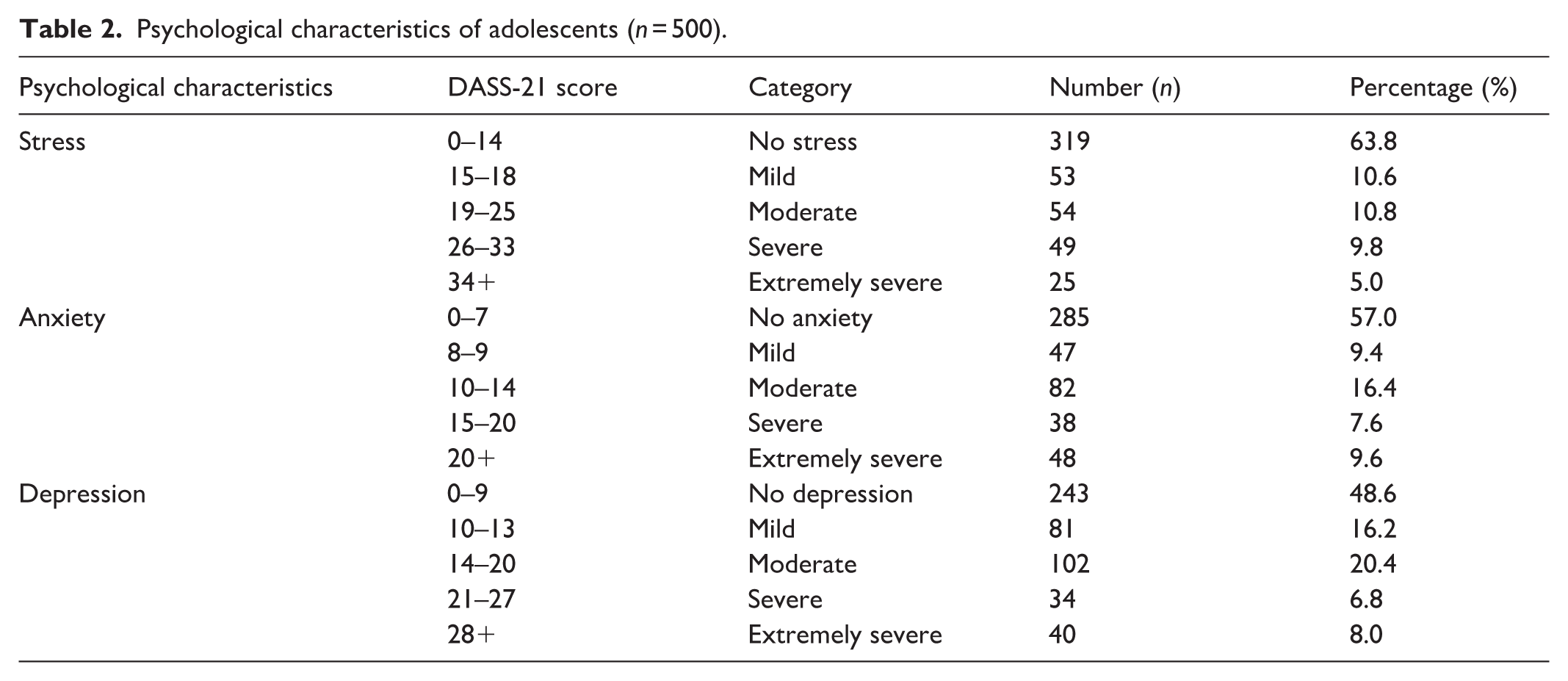
Based on the DASS-21, more than one-third (36.2%, n = 181) of respondents experienced mild to extremely severe symptoms of stress. About 43% (n = 215) experienced different levels of anxiety, while around half of the participants (51.6%, n = 257) experienced mild to extremely severe depressive symptoms, Table 2.
Psychological characteristics of adolescents (n = 500).
Prevalence of SI and attempts among adolescents
Table 3 shows that the point prevalence of lifetime SI was 20.2% (n = 101; 95% CI: 16.9%–24.0%). The past 12 months prevalence was 19.6% (n = 98; 95% CI: 16.3%–23.3%). The prevalence of suicidal attempts was 8.8% (n = 44, 95% CI: 6.6%–11.6%).
Prevalence of suicidal ideation among adolescents.

Associated factors of SI
Variables with p < 0.2 in the univariate analysis were further assessed using multivariate logistic regression to adjust for confounding factors. Although smoking was statistically significant in the univariate analysis, it was excluded from the multivariate analysis because of the small number of smokers in the cohort. In the multivariate logistic regression analysis, including the DASS variables (Anxiety, Depression, and Stress), ever-married adolescents had approximately 7 times higher odds of SI (AOR: 6.9; 95% CI: 1.4–33.2; p = 0.016) than unmarried adolescents. Extreme internet users had over 4 times greater odds (AOR: 4.3; 95% CI: 1.1–16.3; p = 0.033) than normal users.
Among the interpersonal variables, adolescents experiencing family conflicts had more than 3-fold higher odds (AOR: 3.1; 95% CI: 1.3–7.2; p = 0.011). Those who lack close friends had more than 3-fold increased odds (AOR: 3.3; 95% CI: 1.2–8.8; p = 0.017) of SI.
Adolescents with moderate symptoms of depression had 6 times higher odds (AOR: 5.9; 95% CI: 2.2–15.9; p ⩽ 0.001), those with severe symptoms had more than 8 times higher odds (AOR: 8.4; 95% CI: 2.2–34.4; p = 0.003), and those with extremely severe symptoms had over 11 times greater odds (AOR: 11.6; 95% CI: 2.6–52.4; p = 0.001) than those without depressive symptoms, Table 4.
Associated factors of suicidal ideation among adolescents (univariate and multivariate analysis).

Bold values represent statistical significance (p < 0.05).
Multivariate logistic regression, excluding the DASS variables, found that ever-married adolescents are 9.6 times more likely to develop SI (AOR: 9.6; 95% CI: 2.2–42.4; p = 0.003). Those in a relationship are around 4 times more likely to develop that (AOR: 3.7; 95% CI: 1.2–11.4; p = 0.024). Severe internet use (AOR: 4.1; 95% CI: 1.3–13.1; p = 0.015), lack of close friends (AOR: 2.4; 95% CI: 1.1–5.5; p = 0.039), poor relationship with family members (AOR: 2.7; 95% CI: 1.3–5.6.1; p = 0.008), family history of suicide (AOR: 4.5; 95% CI: 1.5–14.0; p = 0.009), and bullying (AOR: 2.8; 95% CI: 1.3–5.7; p = 0.006) had significant associations with SI, Table 5.
Associated factors after multivariate logistic regression, excluding the DASS variables.
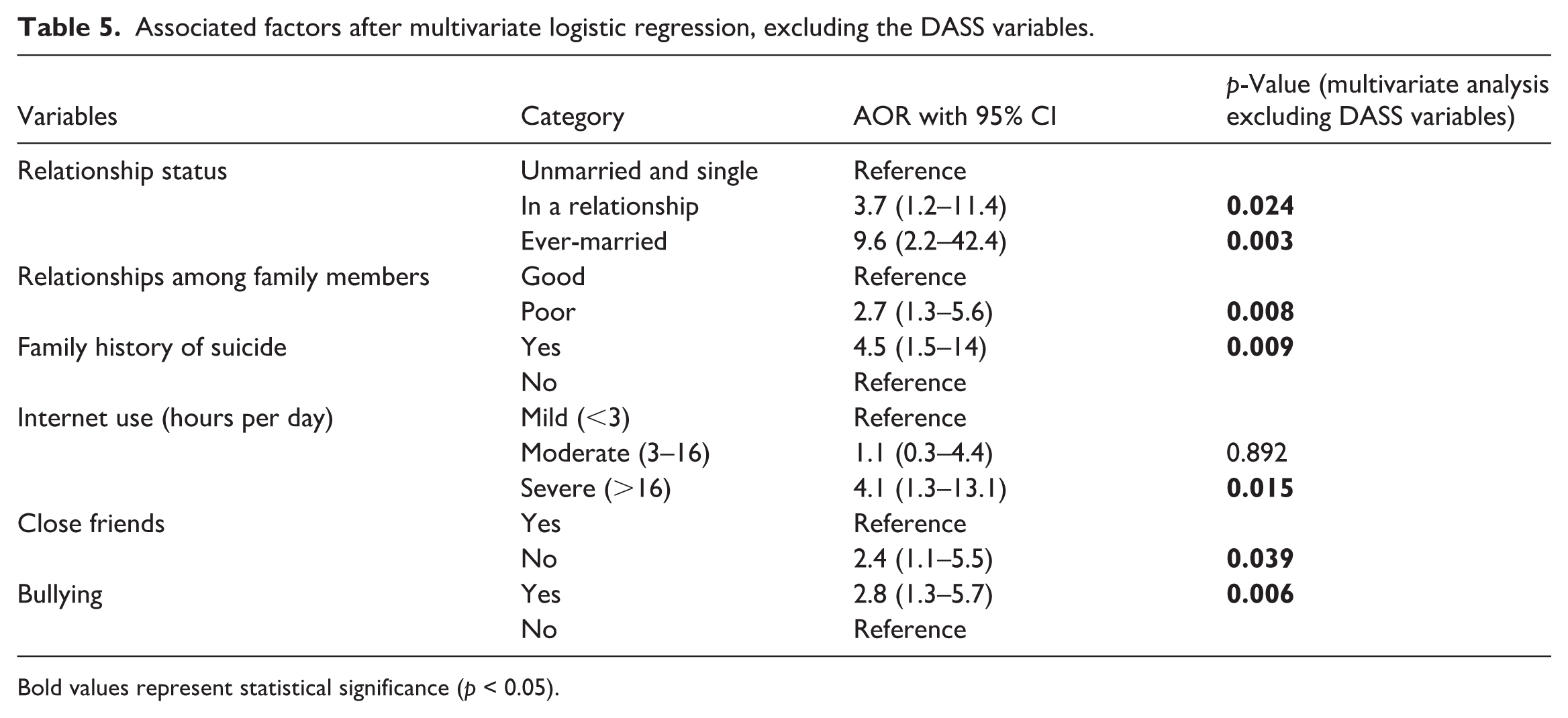
Bold values represent statistical significance (p < 0.05).
Sensitivity analysis
We conducted a sensitivity analysis using the 12-month prevalence of SI as the response variable. Although the associations were in the same direction, we observed some differences. Relationship status, excessive internet use, family history of suicide, and depressive symptoms were found to be statistically significant. Additionally, older age (14–17 years), peer isolation, domestic violence, and poor academic grades were also found to be significantly associated with SI. However, cigarette smoking and poor relationships with family members were no longer significant.
Discussion
This study aims to assess the prevalence and associated factors of SI among adolescents in rural southern Bangladesh. The lifetime prevalence of SI is 20.2% (n = 101; 95% CI: 16.9%–24.0%), and the past 12-month prevalence is 19.6% (n = 98; 95% CI: 16.3%–23.3%). The rate of SA is 8.8% (n = 44, 95% CI: 6.6%–11.6%). Factors significantly associated with SI include being ever-married, excessive internet use, lack of close friends, family conflicts, and moderate to extremely severe depressive symptoms.
The lifetime prevalence of SI observed in this study is higher than the global prevalence (14%) among 12–17-year-old adolescents. 4 A study conducted with 59 low and middle-income countries identifies a 16.9% prevalence of SI and a 17.0% prevalence of SA among adolescents. 29 In South Asia, the prevalence of SI and SA are 16.7% (95% CI: 11.5%–23.5%), and 5.6% (95% CI: 3.5%–9.0%), respectively. 30 Our finding aligns with the prevalence in rural India (20%, 95% CI: 17.4%–22.9%), 31 but is higher than the rates in Nepal (13.59%) 32 and Pakistan (7.2%). 4 The cultural similarity between Bangladesh and India can be attributed to this resemblance.
A previous study reported a 5% prevalence among rural Bangladeshi adolescents, 11 but the prevalence we obtained is higher than that. The potential reason for this difference can be variations in study timelines and respondents’ ages. The past-year prevalence of SI is comparable to that in LMICs (16.2%, 95% CI: 15.6%–16.7%) 33 but exceeds that in India (12.5%, 95% CI: 10.4%–15.0%), 31 and Thailand (8.8%). 34
The higher prevalence of SI in Bangladesh is associated with multiple factors. Relationship status is one of the significant individual factors. Previous studies show that adolescents who are married, engaged, or have received marriage proposals are more likely to experience suicidal thoughts. 35 A systematic review conducted with South Asian countries identifies that being unmarried plays a protective role in female adolescents’ mental well-being. 36 In Bangladesh, 78.2% of adolescents get married before age 18, and 5.5% before age 13. 37 Most adolescents live with their in-laws’ families because of economic dependency and joint family structures. Family conflicts, unemployment, and financial instability at a younger age may have an impact on their mental health. A study suggests that the prevalence of depression among married adolescents is 53.1%, 38 and it is 39% during the antepartum, 39 which may contribute to increased SI. 40 Those who are divorced, separated, or involved with multiple partners may also feel psychological pressure, which can transform into depression and SI. Problematic internet use has been identified as a risk factor for SI in Chinese 41 and Korean adolescents. 42 During the COVID-19 pandemic, the prevalence of internet addiction among Bangladeshi school-going adolescents was 88.25%. 43 Our study finds a significant association between excessive internet use and SI.
Among the interpersonal factors, lack of peer support has been widely recognized as a contributor to adolescent SI.12,44 Previous studies show that a lack of perceived support from friends is associated with poor mental health. 45 Several studies identify a poor family environment as a risk factor for adolescent suicidality.46,47 Depression is another significant psychological predictor of SI.48–50 A study conducted with 5 South Asian countries finds that the prevalence of depression among those who committed suicide was 37.3%. 51 Our study identifies that moderate to extremely severe depressive symptoms are strongly associated with SI in adolescents.
We used lifetime SI as our response variable. As our study population is 11–17-year-olds, asking whether they ever had any suicidal thoughts helped capture early-onset vulnerabilities in their developmental period. Additionally, the possibilities of recall bias could be minimized.
In sensitivity analysis, we observe some common associations, including relationship status, excessive internet use, family history of suicide, and depressive symptoms, indicating their strong associations with both lifetime and 12-month prevalence of SI. However, several newer associations are also identified, indicating their importance in adolescent mental health interventions. This variation can be caused by the lower prevalence of recent ideation and the temporal variability of some risk factors. We are unable to detect any significant association between smoking or poor family relationships and the 12-month prevalence of SI. The probable reason could be the smaller number of smokers. Additionally, the effect of poor family relationships could be less detectable in short-term SI based on the intensity and frequency.
While some studies have reported factors such as bullying, 52 anxiety,12,53 stress, 53 overprotective parents,54,55 a family history of suicidal behavior 56 and gender 48 are associated with SI, our study has not found such associations. These discrepancies may be due to differences in sample sizes, age groups, geographic locations, or study methodologies. Several studies identify associations between cigarette smoking and SI in adolescents.57,58 In our univariate analysis, smoking has appeared as significant. However, we have to exclude that from the multivariate analysis due to the small cohort in the smokers’ subgroup. Further studies are recommended to evaluate this association.
Our findings align with Bronfenbrenner’s ecological systems theory, which indicates that a child’s development is influenced by multiple environmental levels. Individual factors, including relationship status, stress, anxiety, and depression, as well as interpersonal factors like peer conflict, poor family relationships, and a family history of suicide, fall under the microsystem and mesosystem. It indicates that both personal and socio-environmental factors influence adolescent SI. 59
Limitations
This study is conducted using data from three government and non-government schools within a specific geographic area due to time and resource constraints. Although these schools’ admission policies are inclusive, students from remote areas are often unable to enroll due to transportation, financial, and infrastructural barriers. Consequently, the study may not be generalizable to all secondary school students in Bangladesh. Because of the cross-sectional nature of the study, we are unable to establish causal relationships. The possibilities of reverse causation cannot be ignored. Depressive symptoms or SI can lead to behavioral changes like smoking, excessive internet use, or social isolation. Additionally, the participation was voluntary, and we used self-reported data. The lack of pilot testing could affect comprehension and response validity. Knowing that the legal guardians would be informed if mental health disorders or SI were detected, students might be reluctant to provide accurate information. Therefore, the possibility of response bias cannot be ignored. However, given the scarcity of psychiatric care at the sub-district level in Bangladesh, we had to inform their guardians to ensure appropriate counselling and care. We used standard logistic regression, without adjusting for clustering at the school or class level, which might underestimate the standard error. However, the relatively large number of clusters and modest cluster sizes likely minimize the impact of intra-cluster correlation. The multivariate analysis was conducted with basic demographic variables. Therefore, the complexity of self-medication behavior was not fully captured. We exclude adolescents taking medications for diagnosed psychiatric disorders, a high-risk group, to minimize potential confounding, as psychotic medications may influence mood and increase suicidality. The questionnaires were partially validated, and a full psychometric evaluation was not conducted, which may affect the precision of the study outcomes. Therefore, our findings can be used for initial screening, but further studies are recommended to validate the results.
Conclusion
Approximately one in five adolescents in rural Bangladesh experiences SI, and 1 in 11 attempts suicide, highlighting a significant public health concern. Further research across diverse regions of the country is essential to identify area-specific contributing factors. Community leaders and policymakers should develop targeted strategies to address issues such as early marriage. Parents and guardians should be encouraged to engage in open conversations with their children about relationships and avoid involving them in family conflicts. Schools and communities can play a critical role by implementing student engagement initiatives that promote collaboration and social connection. Early screening and behavioral intervention programs are necessary in academic and community settings. Enhancing adolescent participation in mental health and wellness programs may further support psychological well-being and help prevent the onset of SI during the school years.
Supplemental Material
sj-docx-1-smo-10.1177_20503121261428200 – Supplemental material for Prevalence and associated factors of suicidal ideation among rural school-adolescents: A cross-sectional study in Southern Bangladesh
Supplemental material, sj-docx-1-smo-10.1177_20503121261428200 for Prevalence and associated factors of suicidal ideation among rural school-adolescents: A cross-sectional study in Southern Bangladesh by Rifa Tamanna Mumu, Md Parvez Shaikh, Dipak Kumar Mitra and Shadman Sakib Ayan in SAGE Open Medicine
Supplemental Material
sj-docx-2-smo-10.1177_20503121261428200 – Supplemental material for Prevalence and associated factors of suicidal ideation among rural school-adolescents: A cross-sectional study in Southern Bangladesh
Supplemental material, sj-docx-2-smo-10.1177_20503121261428200 for Prevalence and associated factors of suicidal ideation among rural school-adolescents: A cross-sectional study in Southern Bangladesh by Rifa Tamanna Mumu, Md Parvez Shaikh, Dipak Kumar Mitra and Shadman Sakib Ayan in SAGE Open Medicine
Footnotes
Acknowledgements
I am profoundly thankful to North South University for allowing me to do the research. I am also grateful to the headmasters for permitting me to collect data from their schools and encouraged student participation. My gratitude extends to my parents for their unwavering support and inspiration. A preprint version of the research is available on ResearchGate.
Ethical considerations
Ethical approval for the study was obtained from the Institutional Ethics Committee of North South University (2024/OR-NSU/IRB/0201) before data collection.
Consent to participate
Permission was obtained from the respective school authorities. Informed written consent was secured from the legally authorized representatives of all participating students, and informed written assent was obtained from each student. Participants were assured of the confidentiality of information provided and were informed that all data would be collected anonymously and used solely for research purposes.
Consent for publication
Not applicable as the data was collected anonymously.
Author contributions
Conceptualization, Investigation, Methodology, Data curation, Formal analysis, Writing (Original draft preparation): Rifa Tamanna Mumu. Writing (Original draft preparation and editing), Resources: Md Parvez Shaikh. Supervision, Review: Dipak Kumar Mitra. Data collection, curation, Review: Shadman Sakib Ayan.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data is available on figshare.com. ![]() .
60
.
60
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.