
Abstract
Conversations about inclusivity in anatomy education are at a critical juncture. While the need for a more equitable discipline is widely recognised, significant challenges remain. As this project aimed to reimagine what a truly inclusive learning experience could like and how it might be best achieved, an inclusive approach to research methodology was essential to ensure robust and representative results. Due to the paucity in anatomical literature on this topic, the authors applied concepts from sociological research methodology and innovative methods of demographic data collection to their own discipline. The study utilised questionnaires and focus groups to collect diverse data on lived experiences of inclusivity and exclusion in anatomy education. A convenience sample gathered quantitative and qualitative data through questionnaires and semi-structured focus groups. Guided by inclusive research practices including participatory research, this study makes use of inductive reflexive thematic analysis with critical orientation to situate inclusivity in its social, historical and political contexts. This paper discusses how the authors incorporated these inclusive methods, explores the challenges this type of research generates, and acts as a framework for those wishing to conduct more inclusive research in their discipline. Application of these methods yielded richer and more nuanced data, thus increasing the validity of the study. Although anatomy education may not currently represent diverse populations, positive action towards change is underway, with many in the discipline eager to actively confront exclusion. The existing dataset is predominantly Eurocentric. As such, the next phase of this research will translate recruitment literature and questionnaires into other languages to collect more global perspectives. To encourage further anti-exclusion research, the data will be made widely accessible for analysis.
Introduction
Conversations around inclusivity in anatomy education are at a critical juncture. That a more equitable discipline is needed has been widely recognised, but creating meaningful change remains a formidable challenge. The political backdrop of the 2020 Black Lives Matter protests and the more recent queer, trans, feminist and disability activism have renewed interest in how anatomy curricula fail to represent diversity, provoking educators – us included – to question how it might be best improved. Important work on decolonisation has made space for more overarching discussions around more authentic inclusion, laying bare the scale and complexity of the work to be done (Finn et al., 2022). Seeking to move beyond decolonisation, the phrase anti-exclusion conceptualises our ambition to affect change that not only fosters greater inclusion, but also works against forces that discriminate and marginalise. Medical governing bodies have warned that action for change should not be motivated by crises, as reactive approaches are often short-lived and inadvertently perpetuate exclusions by focusing on a single issue (Medical Schools Council’s Equality, Diversity and Inclusion Alliance, 2021). Attentive to global theories of intersectionality as an analytical tool (Crenshaw, 1989, 1991, 2014/2019), the project reported here aims to progress understanding of what inclusivity in anatomy education looks like and make sustainable steps towards achieving it by using innovative and inclusive research methodology as a foundation. Questionnaires and focus groups enabled collection of a diverse set of data reporting on experiences of inclusivity and exclusion in anatomy education worldwide. Initially interpreted by the authors using reflexive thematic analysis, the data are situated in their social and historical contexts, aligned with contemporary scholarship and policy frameworks, and made accessible to as many people as possible. Our hope is to establish a readily available, rich repository of data that researchers beyond our institution and around the world can analyse, that will encourage a more inclusive approach to anatomy research, prompt new insights into anatomy education, spark new conversations, and encourage community-based collaboration amongst researchers, students, and educators. These processes aim to foster long-term shifts in global anatomy education and research that are attentive to the continually evolving personal and political complexities of inclusivity.
Reflexivity statement
This paper was written by three white cis-gendered women with educational backgrounds in gross anatomy and medical history. We have only experienced the university education system (and the wider political and sociological landscape) within the United Kingdom and are critical of the way in which Anglo-Western cultures of higher education have been, and continue to be, heavily influenced by colonialism. Although inclusivity has always been integral to our personal and professional values, some of us have never collected qualitative data about inclusivity before. We are willing to learn and improve as we strive to improve inclusivity and recognise the importance of addressing any gaps in our experience and knowledge. We bring different personal and academic perspectives to the data, and each have our own research interests within the topic of inclusivity. Our collaborators (listed in the Acknowledgements) who supported the creation of the questionnaires and have contributed to the analysis represent a wider range of demographics. However, we are mindful that our and our collaborators’ demographics are not representative of all people involved in anatomy education, and that our positionality will have affected all stages of this research project. The ability to conduct this study highlights our privilege, and that we are very fortunate to have the full support of our faculty. This is why we are creating a robust process for interested stakeholders to analyse our anonymised data through different lenses and to encourage them to publish their own perspectives. We are also supporting community members to translate the questionnaire and focus group materials, plus the participant information sheet, into other languages and are encouraging them to adjust the content to suit the needs of their home countries, in order to avoid imposing a Western narrative on future dimensions of the project.
Defining the problem
Anatomists themselves have acknowledged the challenges the discipline faces in representing and including the populations it serves (Finn et al., 2022; Meyer and Cui, 2019). Reflecting on discussions with fellow academics, Musarrat Maisha Reza has warned of dismissive attitudes towards inclusivity within medicine, noting that decolonisation is sometimes perceived as ‘more relevant to the arts and social sciences’. Reza (2022) explains that the field typically prioritises a ‘black and white’ perspective that allows little room for diverse viewpoints. Yet despite these barriers, opinions are shifting, and positive change is underway. Institutions are steadily embracing inclusive approaches to curricula too, diversifying student and staff populations and better supporting those more likely to be structurally and systemically discriminated against, oppressed, marginalised or excluded. For example, an expanding body of literature is recommending new approaches to teaching biological variation, accounting for difference and furthering thinking from the Global South (Morley and Leyton, 2022). From teaching sex as a spectrum rather than as a binary (Strkalj and Pather, 2021), to recognising how colonial histories have impacted the diversity of curricula (Finn et al., 2022), to eschewing eponyms for more inclusive terminology (Easterling and Byram, 2022; McNulty et al., 2021), many educators are being empowered to better meet the diverse needs of their learners.
The diversity of enrolees onto medical courses in the United Kingdom is also rising, as is the proportion of teaching staff. Frameworks such as the Athena Swan charter for gender equality, the race equality charter and British Medical Association (BMA) charters including those which outline practical support for mental wellbeing and conditions such as fatigue, have helped to formalise employer commitments to more equitable places of teaching and learning, encouraging good practice across the United Kingdom universities. Questions persist about the lasting impact of such progressive policies on factors such as representation; but the high uptake of charters such as Athena Swan, for example, is acknowledged for raising career aspirations, mediating wage differentials and providing women with a ‘generation of recognisable role models’ (Gregory-Smith, 2015; Munir et al., 2013). Researchers are working to support minoritised faculty, developing strategies for mitigating exclusion; for example, Rodríguez et al. (2022) equip those working towards equity in medicine with a common lexicon, introducing a glossary of terms around the minority tax felt by underrepresented faculty. Efforts to enhance learning experiences for underrepresented student groups, including those with neurodiversity (Robinson, 2022) and disabilities, emphasise the importance of challenging exclusion for safe and effective learning environments (Nieminen and Pesonen, 2022). Whilst these emerging efforts to confront the structural inequalities in medical education are encouraging, they bring into view the need for wider radical overhaul. A more intentional, constant and multifaceted approach to equity, diversity and inclusion (EDI) is required, starting with better understanding of lived experience of how underrepresentation is perceived and manifested.
What’s in a name?
At the time of writing in 2023, the language of equality, diversity and inclusion has become a familiar – and at times superficial – phenomenon in education (Charles, 2019; Finn et al., 2021). Attempts to diversify ‘decolonise’ curricula, itself a contested terminology, must be embedded in intersecting issues of social justice, making clear how medicine has been inflected by – and has also helped to sustain – sexist, ableist, heteronormative, classist and colonist cultures and practices. As Finn et al. (2022) have identified, processes such as decolonisation in education – which the authors frame as a ‘form of making curricula inclusive’ – are long-term, ‘messy’ endeavours only effective when characterised by meaningful change and sustained by individual, cultural and institutional commitment. The Medical Schools Council Equality, Diversity and Inclusion Alliance (2021) framework for inclusion, which suggests best practice for those working in medical school environments, similarly endorses decisive action and implementation of changes which not only accelerate inclusion but also challenge exclusion. Offering recommendations on improving inclusivity across key areas of practice such as curricula content, delivery and assessment, clinical placements and recruitment and selection processes, the council emphasise that transparency, accountability and clear reporting are core components of significant and lasting change.
This aspiration towards consistent, meaningful and active change that is transparent and therefore adoptable by others, guides our own commitment to equity in anatomy education. Our international research examines perceptions of inclusivity in anatomy education among anatomist and students. It adds to existing knowledge by identifying challenges, promoting good practice, informing recommendations for change, and steering future research.
Description
Both our anatomy student and anatomist questionnaires remain open to allow for maximum participation. We are conscious that the landscape of inclusivity is constantly changing, and by maintaining this study as dynamic, we can collect up to date data that speaks to the most prescient issues and developments in anatomy education. Phase 1 of this project, which included the initial distribution of our questionnaires, and the first round of student and anatomist focus groups, was completed on the 19th June 2023 (Figure 1). The data collected from questionnaires and focus groups was exported for analysis at this point, with the findings informing this publication and subsequent research reports and peer reviewed publications
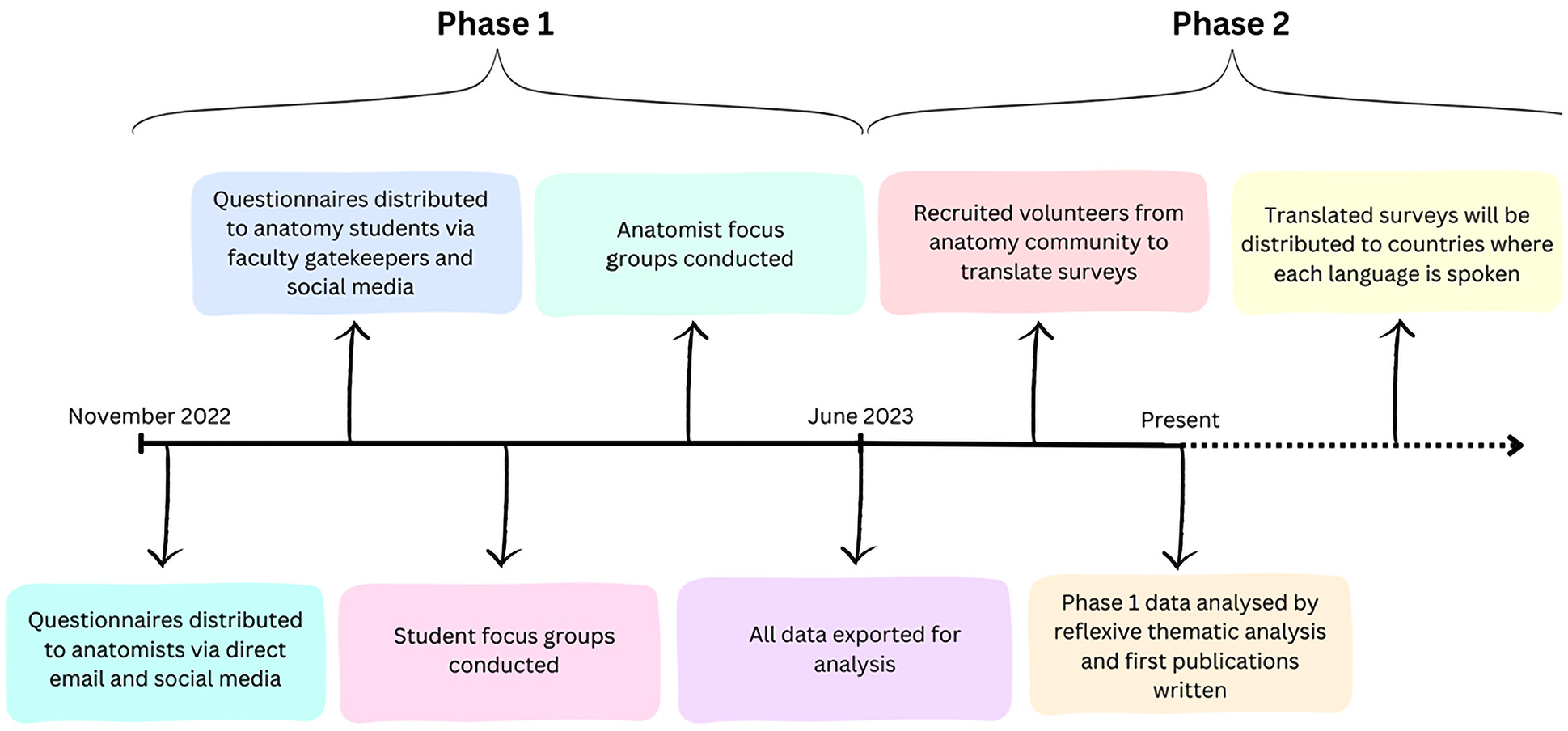
Provides a timeline of the project from the launch of the anatomist questionnaire in November 2022 to our present and ongoing work expanding the international reach of the project through translations of research materials into additional languages.
Participant recruitment: Questionnaires and focus groups
Recruitment for the anatomist survey in Phase 1 was completed through convenience sampling via emails to known anatomy colleagues, who were asked to distribute the survey amongst their own professional networks. We define ‘anatomist’ as any person that works in the field of anatomy, this includes, for example, educators, researchers and technicians. These colleagues were later asked to distribute the student questionnaires, and in this role acted as gatekeepers determining which student cohorts had access to the questionnaire. By ‘student’, we are referring to anyone studying anatomy, for a minimum of one semester, within their university programme. Posters with QR code links to the questionnaires were also physically displayed in our anatomy department and emailed to the team’s contacts. Due to the extensive engagement and positive feedback generated by Phase 1, we decided to expand the reach of our questionnaires by sharing them more widely. To do this, we distributed posters with QR links to the questionnaires across the social media platforms Twitter, Facebook and Instagram, using accounts specifically set up for the Inclusivity in Anatomy Education project. We contacted student led anatomical societies and EDI groups across the allied health professions to request distribution of the questionnaire link to their memberships and networks. We also contacted anatomical societies including International Federation of Anatomical Associations (IFAA) who shared the study and its questionnaires with their member associations, thus increasing the international reach of the project. Additionally, we promoted the questionnaires to educators at anatomy conferences, including the Anatomical Society’s winter meeting and the American Association for Anatomists’ Anatomy Connected meeting in 2023. Our website, which was shared alongside these communications, offered additional participation details and humanised the research by introducing our team members and their inclusivity-driven research interests.
Alongside questionnaires, Phase 1 of the study also made use of small focus groups to collect student and anatomist perspectives on inclusivity in anatomy education. To recruit participants for focus groups, we invited questionnaire respondents to opt into group interviews by providing their email address. Respondents then selected their preferred focus group through a Google form. As part of our inclusive research process, we aimed to make the interviews an accessible and safe experience where people felt comfortable sharing their ideas. As such, we conducted focus groups via Zoom to reduce the impact of geographic location on the ability to attend. We also ask interviewees to let us know if there was anything we could do to better accommodate their involvement. Post-focus group completion, students received a £10 Amazon voucher as a token of our appreciation.
Participation interactions
Our questionnaires, which we began distributing in November 2022 to anatomists and in February 2023 to students, have attracted an encouraging number of responses to date (see Table 1).
Shows the number and demographics of anatomist and student participants who responded to the questionnaire and focus groups.
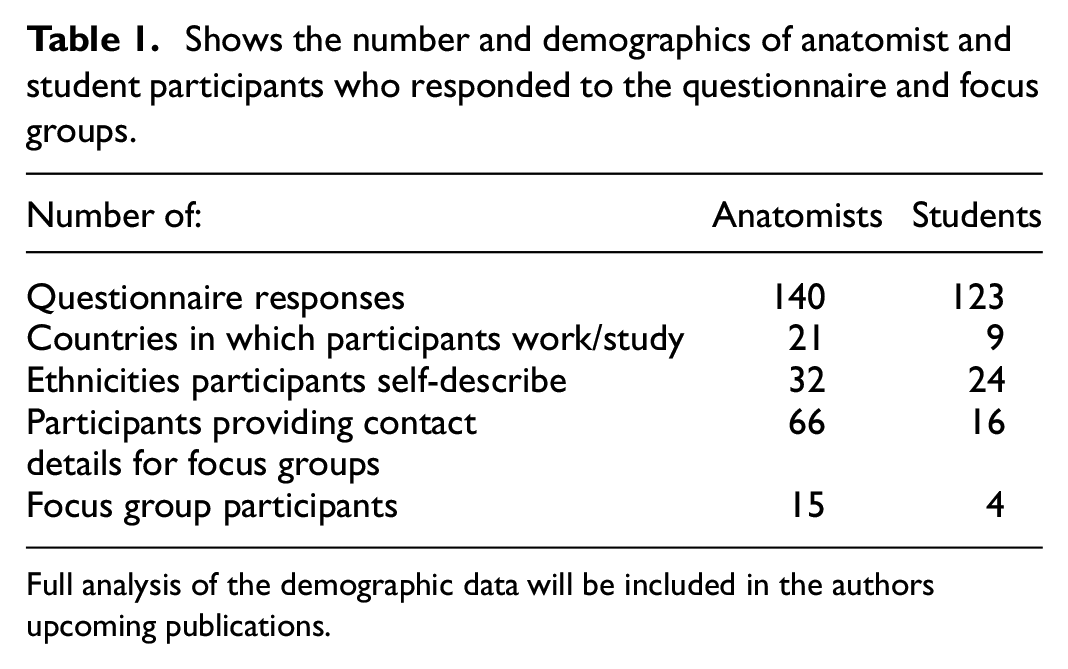
Full analysis of the demographic data will be included in the authors upcoming publications.
The full analysis of the demographic data from this questionnaire will be explored in more depth in the authors’ upcoming paper about incorporating open-text demography.
Questionnaire design
Two questionnaires (Supplemental Tables 1 and 2) were designed to gain insight from anatomy anatomist and students. There were 20 questions in total within the student survey, and 21 questions within the anatomist survey (Supplemental Tables 1 and 2). To understand whether demography impacted experience of inclusion or representation several questions asked respondents to self-describe or select from a scale their age, gender, sexuality, ethnicity, skin-tone, country of employment or study, religion, any health conditions or differences which they felt impacted their day-to-day activities, and activities at their institution.
The remaining questions collected largely qualitative data around lived experiences of representation, inclusivity and diversity, in a combination of closed and open-ended formats. Some invited an agree/disagree response or a yes/no answer, for example, ‘Do you feel that the anatomy curricula at your institution are inclusive of X characteristic? (agree/disagree)’ and ‘Has your anatomy department put in any initiatives to improve inclusivity? (yes/no)’. These questions were proceeded by open-ended follow up questions providing respondents the opportunity to elaborate on their answers, as well as to express their opinions on effectiveness and related aspects. There were no length limitations on responses to open-ended questions, which centred around demography, representation, inclusivity initiatives and barriers to advancing anti-exclusion. As noted by Braun and Clarke (2021), this type of survey design – which relies on participants to use their ‘own words’ rather than choose from answers, produces ‘rich and complex accounts’ which can reveal much about ‘subjective experiences, narratives, practices, positionings, and discourses’.
Prior to release, the questions and format of the questionnaires were reviewed by two colleagues within our institution outside of anatomy that were involved in various EDI committees, as well as external colleagues who served as members of the steering group ‘The Anatomy Collective for Equality’ (ACE). ACE are an action group comprised of international anatomists united in their commitment to advance equality, diversity and inclusion, and work to support and empower individuals to take action towards improving inclusivity across their own practice and institution. Changes were made based on feedback from these colleagues to ensure the questions were as inclusive as possible.
Both questionnaires prioritised accessibility and inclusion. They are both hosted on the online Joint Information Systems Commitee (JISC) system, an infrastructure which is accessible, offers anonymity, and has reduced environmental impact compared to distributing written materials. JISC allows for real-time analysis, meaning data can be simultaneously collected and processed. Anonymity was ensured to avoid analytical bias and to encourage respondents to provide honest answers without concerns about identification by their employers, colleagues or peers.
Approach to demography
One of our research goals is to determine whether demography impacts how represented people feel in their anatomy curriculum, in terms of both physical and non-physical identity. As such, in our questionnaires we asked questions which invited demographic information about ethnicity, skin colour, health conditions, disabilities, physical, sensory or cognitive differences, gender, sexuality, religion and spiritual beliefs and country of study. We identified many different approaches to gathering demographic data from the 2021 UK census but were disappointed that the available tick boxes offered users limited options. For example, the category of ‘White and Asian’ was too broad to be representative. We were also uncomfortable with the use of the word ‘other’, as it suggests a deviation from a perceived ‘norm’, running counter to inclusive methodology. To address this issue, we turned to the Wellcome Trust supported Diversity and Inclusion Survey (DAISY) guide, a tool provided by Equality, Diversity, and Inclusion in Science and Health. This guide provides advice on asking demographic questions which collect qualitative responses and were incorporated into the original demographic questions. Many of the suggestions were a great improvement on already existing demographic surveys, however, when shared with our colleagues, some still did not feel their identities were represented by the available choices. This finding caused the research team to reflect thoroughly on why we were collecting the data, and whether there was a more inclusive way to approach these questions.
Due to a limitation in the JISC platform, if respondents wanted to self-describe rather than select from a list of options, they were forced to select ‘other’. To avoid this, we opted to let respondents freely describe themselves using open-text boxes, removing checkboxes altogether. This approach to eliciting qualitative data has several significant advantages to a study interested in lived experience, as observed by Frith (2000), and Braun et al. (Braun and Clarke, 2021); designing the questions allowed us to maintain focus on topics important to the research, whilst simultaneously ‘captur[ing] what is important to the participants’ and gaining insight into the ‘language and terminology’ that they used. This access to language and terminology was particularly important when it came to coding the data, allowing us to make clear connections between responses. While this qualitative approach to collecting demographic information allowed participants to express themselves more freely, it made the data analysis process more challenging, producing responses of different length and focus. Please note that this method may not be feasible for very large data sets, in which case, the DAISY guide may be a more appropriate framework. This process and its associated challenges are not new; eliminating checkboxes has been suggested by other researchers interested in inclusivity, including Fernandez et al. (2016). However, this work did not provide guidance on how to analyse this data. As such, the authors are collaborating with sociologists, psychologists and psychometricians to offer a meaningful approach to the analysis of open text demography data that avoids reductionist pitfalls. These findings will be released in their upcoming research paper and book chapter.
Colourism is a health and social justice issue globally (Dixon and Telles, 2017), and has been shown to have implications in anatomy resources (Louie and Wilkes, 2018). As ethnicity does not necessarily relate to skin colour, to compliment the open-text demographic questions, we included a chart for respondents to self-indicate their skin colour.
Focus group format
Our aim for focus groups was to explore some themes in more detail than for which the questionnaires had allowed, introduce some new discussion questions, make connections between ideas and lived experiences, and discover possible new directions for the research, including the formation of an inclusivity toolkit for anatomy educators. As such, the questions for the focus groups were informed by the questionnaire data. Prominent themes and areas which required further discussion were identified. For example, in their questionnaire responses, educators expressed concerns around using the appropriate inclusive terminology in their teaching. Subsequently, the anatomist focus groups asked, ‘What are your thoughts on the changing landscape of terminology?’ and ‘What do you think is the best approach to keep up to date with these changes?’. The students in the two focus groups were asked a series of related questions: ‘Do you feel that the terminology used in your anatomy curriculum is inclusive? Inclusive enough?’, ‘How do you define inclusive language?’, ‘Do you feel inclusive language is important? Why?’ and ‘Inclusive terminology is currently changing rapidly, what do you think is the best approach to keep up to date with these changes?’ Seven main questions were prewritten and asked in the anatomist focus group, with each main question leading into between one to three sub questions (Supplemental Tables 3 and 4). For example, the first main question was ‘What is your experience of representation in the curricula you work across?’. This was followed by two follow-up questions: ‘are you and your students represented in the curriculum?’ and ‘are there some facets of the curriculum that you feel represent diversity more effectively than others?’ Whilst these sub questions were planned in advance, they were also led to a certain extent by the discussion as it unfolded, and were adapted, expanded on or eliminated accordingly. The student focus groups were structured similarly, with three main questions, each of which led to one to four sub questions.
Each session ran for approximately 90 minutes on Zoom. The sessions were recorded for use by the research team only; for the purpose of analysis, an anonymised transcript was produced using Descript. Each session followed a flexible format which elicited qualitative responses to a set of questions. The interviewer adopted a facilitative role, avoiding the imposition of hierarchies to encourage participants to freely express themselves without feeling constrained by right or wrong answers or uncertainty. Although there were set questions, the format of the session was flexible to accommodate discussion. This allowed participants – who by nature of their involvement tended to have strong opinions about inclusivity or memorable, emotive personal experiences of it – the space to share personal testimonies and thoughts in a supportive environment.
Questions in both focus groups were geared towards furthering ideas for action towards improving inclusivity, and provided an informal forum for knowledge exchange, particularly concerning teaching practice. For example, anatomists were asked: ‘How do you/would you like to take inclusivity into consideration when developing anatomy curricula or delivering teaching?’ with participants generously sharing measures that centred around implementing accessibility measures and ensuring representation within their curriculum content and their everyday social interactions with students (e.g. ensuring they identified and used their student’s correct pronouns). Students were asked ‘How do you think anatomists can take inclusivity into consideration when developing their anatomy curricula?’ and in response reflected on the ways in which their educators were – or were not – active advocates for anti-exclusion in medical education.
Data analysis
When carrying out our research, we were conscious of how potential biases and positionality might affect setting research agendas, collecting and interpreting data. Some of these have been limited by the inclusive research strategy, however, we must acknowledge that bias is involved in all research projects as the researchers determined the research aims and questions, methodology, analysis, and decided what data and outcomes are shared. As mentioned previously, the research team is small and does not pretend to represent the diverse groups involved in anatomy education. With this in mind, the authors used the method of reflexive thematic analysis, coined by Braun and Clarke (2021), to analyse the data. We took a constructionist approach to the data, as although frequency of data can indicate importance, the meaningfulness of the data was prioritised. By collecting demographic data, we were able to orientate the open text responses critically within the socio-cultural context of the participants’ backgrounds.
The aim of reflexive thematic analysis is to develop themes from data sets through processes of interrogation and interpretation. These themes can then be investigated for significance and patterns of meaning, with careful critical attention paid to the role of the researcher(s) who produced them. Although Braun and Clarke acknowledge that there is no one definitive method of reflexive thematic analysis due to researcher subjectivity and varying project needs, they offer the following six steps as a framework for its practice:
Phase 1: Familiarising yourself with the dataset
Phase 2: Coding
Phase 3: Generating initial themes
Phase 4: Developing and reviewing themes.
Phase 5: Refining, defining and naming themes
Phase 6: Writing up
This process allows researchers to rigorously acknowledge their background at the start of their study, so they can assess the potential impact of their identity on influencing ongoing research processes, from deciding the research questions to collecting and analysing the data. As part of this process, we formed reflexivity statements, which were shared with each other and can be read above. This method of data analysis states that themes are not extracted from the data, but rather that the researcher applies the themes to the data which are influenced by their social, educational and political background. No two researchers will interpret the data in the same way, which is why the analysis for this study is being conducted by multiple researchers. Once processes are in place to release the data more widely, stakeholders can analyse certain aspects of the data (e.g. a specific demographic) to apply their background and experience to the dataset.
The analysis was carried out by multiple members of the research team using the framework from Braun and Clarke as a unified reference to maintain consistency and reliability. The coders changed depending on which section of the data was being explored as our collaborators were mostly interested in one specific aspect. For example, ACE members analysed data concerning barriers to improving inclusivity, a colleague with EDI experience analysed the data about representation, and a psychometrician analysed the demographic data.
Discussion
Addressing our own privilege
The groundwork for this research has been laid through a series of initiatives which have taken place at Peninsula Medical School since 2020. Staff in the school were encouraged to make an equality pledge 1 (Watson et al, 2023) demonstrating their commitment to embedding equity and inclusion into their working life, with one of the team pledging to improve representation of diversity in the anatomy department. Conscious that the department’s Eurocentric anatomy models were inadequately representing the diverse student population or the communities they would go on to treat, the anatomy lead set about acquiring new teaching resources. Having failed to find high-quality models with different skin tones and morphological features available commercially, they partnered with model makers Adam,Rouilly to offer users the option of applying various skin tones and features to their models. Whilst this action should have been implemented sooner, its positive impact includes an ongoing commitment from Adam,Rouilly to develop resources that represent a broader spectrum of body shapes, sizes and anatomy beyond the able-bodied, white, young male norm. While these steps towards greater inclusivity benefitted the department, they also inspired reflection on the bigger picture, beyond our research team and the individual university.
Through questionnaire responses and focus group discussions, it became evident that many individuals involved in anatomy education face constraints in actively engaging with inclusivity. Anatomy researchers and educators cited cultural barriers, time constraints, financial pressures, lack of knowledge and doubts about institutional support as reasons why they were not currently undertaking or planning anti-exclusion initiatives or planning any for the future. In contrast, we are conscious of the privilege we have experienced in setting up and launching this project. Fortunately, our medical school values align with the motivations for this project. ‘Inclusive’, ‘Kind’ and ‘Socially-Minded’ are directly mentioned within these values, which have allowed us to feel supported by colleagues and apply for small amounts of internal funding to hire a short-term research assistant on the project. Without this individual’s help, the project would have stalled due to the heavy teaching load of the anatomy team. This support may not be available in other institutions, as shown in our data. To pass on this privilege and to maximise the potential of this project, we aim (as noted above) to make our anonymised data and research methods available to others. This includes making the questionnaires available for translation into other languages, so that researchers from around the world can collaborate with us to gather more global perspectives on what inclusivity in anatomy education looks like around the world, and how best to achieve it.
Inclusive research practice and agenda
Our research focuses on inclusivity and representation, so we wanted to maintain those values within all aspects of it, including our research agenda. As researchers, we recognise the limitations of their own perspectives and experiences in capturing the diverse spectrum of human experiences within the study’s domain. It became evident that the research would inevitably confront the task of representing the ‘Other’, a concept first noted by Fine (1994), who examines the importance of involving the represented individuals in the research dialogue, transforming them from ‘subjects’ into active co-creators. Although Fine talks about the ‘other’ when she refers to those who have different backgrounds and experiences, we chose not to utilise this term in our questionnaire as othering homogenises groups of people and creates an ‘us versus them’ social narrative (Akbulut and Razum, 2022).
To address this, we embarked on a deliberate effort to diversify our collaborator pool, seeking individuals who shared an interest in Equity, Diversity and Inclusion (EDI) from different institutions. Collaboration was made with the Anatomy Collective for Equality (ACE) and colleagues in our institution who are actively engaged in broader EDI initiatives within and beyond the university. Their input was pivotal in the development of the research questionnaire. Furthermore, the team plans to make anonymised datasets available to key stakeholders, thereby affording individuals from underrepresented groups and early-career or underfunded researchers access to valuable data resources. This approach acknowledges the nuanced insights that individuals from underrepresented groups bring to data analysis.
The research team’s commitment to community-based participatory research (CBPR) is demonstrated in their determination to engage and benefit the wider community. In this case, the community encompasses not only anatomy learners but also healthcare professionals and the broader public. This spirit of mutual benefit, support and socially engaged research was also expressed by our participants, as evident in the following quote from the anatomist questionnaire data: [Inclusivity in anatomy education is] creating an environment where everyone feels valued, liberated, and can develop, explore their individual interests and contribute to the betterment of society.
Everyone involved in the anatomy community, including educators, students, researchers and technicians, are viewed as collaborators, data analysts, stakeholders, authors and beneficiaries. To ensure a comprehensive and multidisciplinary perspective, experts in sociology, psychology and psychometrics were recruited to enrich the research with a multitude of viewpoints and draw upon theories and principles from disciplines outside of anatomy. CBPR has three components (Leung et al., 2004); 1. Participatory research which was carried out using the questionnaire and focus groups. 2. Education, which will involve increasing awareness in the anatomy community and giving practical advice for making curricula more inclusive via a toolkit, and 3. Social action, where the research is taken on by the global community to start their own projects and analyse the data with their own lens. This could also involve lobbying organisations to make their resources more inclusive, as we accomplished with Adam,Rouilly, the model manufacturers.
Representing diverse voices
As Wilkinson and Kitzinger (1996) emphasise in ‘Representing the Other’, it is crucial to listen attentively to the voices of those being represented while avoiding adulterating their perspectives. This is reflected in our predominant reliance on qualitative data collection methods, allowing participants to articulate their thoughts and experiences in their own words. Nevertheless, the research team acknowledges their position of authority over the data, as they determine research questions, participant recruitment strategies and data analysis methodologies (Corlett and Mavin, 2018). It is recognised that if a different group of researchers in a distinct institutional context were to undertake a project with the same research question, the outcomes could vary significantly. This interpretivist paradigm is driven by an understanding that the research process is inherently subjective and influenced by the composition of the research team, their environments, world views and other social factors (Pervin and Mokhtar, 2022). The significance of challenging the dominant positivist paradigm in medical education research and taking a constructionist approach has been observed Bunniss and Kelly (2010).
Research data gathered from the questionnaires and focus group transcripts were analysed using reflective thematic analysis, as described by Braun and Clarke (2021). This approach allowed for the critical evaluation of our identities as researchers and individuals, and acknowledgement of the potential influence of backgrounds, both social and educational, on data interpretation. Each researcher initiated the project with reflective considerations of their social, political, personal and educational backgrounds, maintaining ongoing reflexive accounts throughout the data analysis process (Letherby et al., 2012). To encourage more people to contribute their perspectives to data analysis, we have incorporated elements of the Community-Based Participatory Research approach, aiming to give a wider community mutual ownership of this project (Viswanathan et al., 2004). When referring to the ‘community’, we consider anatomists, students, anatomical resource companies, societies and the wider public to be included. They have been involved in several ways;
- Collaborating with members of the steering group ACE and colleagues with specific expertise in EDI we invited to give feedback on the questionnaire design. This feedback informed our decision to invite open text responses to our demographic questions, since – members of the community did not feel represented by the tick boxes originally offered.
- Anonymising the data sets to share with the community Robust processes need to first be put in place to ensure participant anonymity and safety.
- Translating the materials into other languages.
- Informing changes made to anatomy resource companies such as Primal Pictures who have created an EDI pledge in order to make their products more inclusive and Kenhub who asked us for feedback on their new EDI statement.
- Presenting data at the Anatomical Society Winter Meeting 2023The authors are also hosting a symposium based on the project at the IFAA international congress in summer 2024, to share more broadly with the anatomy community.
- We hope that this research can eventually inform wider publics through outreach projects to celebrate and explore anatomical diversity.
Although others have already drawn attention to the lack of inclusivity in anatomy education, there has not yet been an explorative study that actively seeks to involve the anatomy community on a global scale to make changes to anatomy curricula and lobby anatomical organisations worldwide.
Coming together: An inclusivity hackathon
A subsection of the data was analysed by the action group Anatomy Collective for Equality (ACE) and used as the basis for a ‘hackathon’. This concept was adapted from the field of computer science, where coders who are not usually collocated come together to create innovative solutions to challenges in a set amount of time (Angarita and Nolte, 2020). Similarly, the themes from questions asking about the barriers to inclusive anatomy education were used to create four case studies surrounding these challenges. The attendees were split into groups with facilitators to discuss these cases more deeply and come up with solutions together. After the hackathon, attendees were asked to make a pledge to improve inclusivity in their own institution which could be anything from adding pronouns to an email signature to wider curricular changes depending on the person’s level of influence. Making equality pledges has been shown to increase dialogue around EDI, and the authors believe it could lead to a positive shift in culture (Watson et al., 2023). This collaborative style of event could be used across a range of platforms, including conferences, workshops, organisations and societies to keep the conversation going and foster collaboration between anatomists worldwide so tackling inclusivity doesn’t feel so isolated.
Global collaborations to pledge for inclusivity
As a result of the ACE hackathon event, a virtual anatomy software company that was in attendance pledged to make their platform more inclusive based on topics they discussed. They produced an extensive action plan which was sent to the research team and ACE for feedback and review. This company has a global consumer base, and has translated their platform into multiple languages, so showing public support of EDI values will send a pungent message to their users about its importance. Since then, a popular online anatomy resource company has also asked the team to review their materials for inclusivity and representation. Working with these international companies will maximise the impact of the data on a global scale, so it reaches more anatomists and students.
Sharing actions towards best practice
In addition to the group discussion which occurred during hackathon, the anatomist focus groups acted as an informal forum for sharing best practice, as well as barriers to achieving greater inclusivity in anatomy. Anatomists were all asked ‘How can anatomists take inclusivity into consideration when developing anatomy curricula?’ As well as ‘Have you or your anatomy department put in place any initiatives to improve inclusivity?’ Participants generously reflected on their own inclusive teaching techniques and shared informal anecdotes about how their efforts were received by students. This is where it became apparent that small changes can make a big difference. For example, one educator shared that their anatomy department had begun including students as ‘co-creators’ in their own curriculum. As part of this, mixed working groups of anatomists and students worked together on improving inclusivity and holding their institution accountable to making change. Other participants similarly described students taking an active part in improving inclusivity, including instigating initiatives around more diverse representation in dermatology resources. In the student focus groups, speakers expressed gratitude for efforts towards greater representation across anatomy curricula, saying that these efforts made them feel that they belonged in medicine more widely. One student who was involved in teaching themselves brought up the value of visible signifiers of inclusivity beyond curricula content, giving the example of pronouns on badges and pride badges as inclusive culture for all involved.
Other participants found the focus groups a safe space to admit they were unsure about where to start, but that listening to others and taking part in the focus group had given them the confidence to begin implementing inclusive approaches to their teaching (e.g. because they had gained new knowledge around terminology) or to actively seek out – or lobby for – training to help with doing so. It is important to mention that a great breadth of discussion took place with participants across the project, and some expressed unease with confusion around or objections to efforts to improve inclusivity within medical education. Whilst these responses will be closely considered in further research outputs, they serve as a reminder that there is no consensus around issues of inclusion. Indeed, unanimity is rarely productive; confronting the complexity of what inclusivity in anatomy education looks and how we might improve it will necessarily involve listening to a great diversity of thought and balancing different, changeable perspectives.
Challenges conducting the study
Throughout the project, collecting a diverse range of data from both educators and learners in an inclusive manner posed challenges. Firstly, all communications were in English, which limited engagement from those in non-English speaking countries. Convenience sampling was used to distribute the questionnaire in Phase 1, of which most of our contacts and social media followers were based in the UK. This limitation biases the data towards Western points of view, which is not representative of all anatomists and students who are involved in anatomy education (see Figures 1 and 2). Also, some countries ban Western social media sites, like China, which further restricts the international reach of the study. In addition, most participants teach in medical courses due to our limited range of contacts. However, medicine is not the only programme where learning anatomy is fundamental to the curriculum. Other healthcare programmes like nursing, paramedicine, radiography, etc., are not represented in phase one of this study, despite inviting contributions from these areas, which make up a large proportion of anatomists who have equally valuable views and experiences (Figure 3).
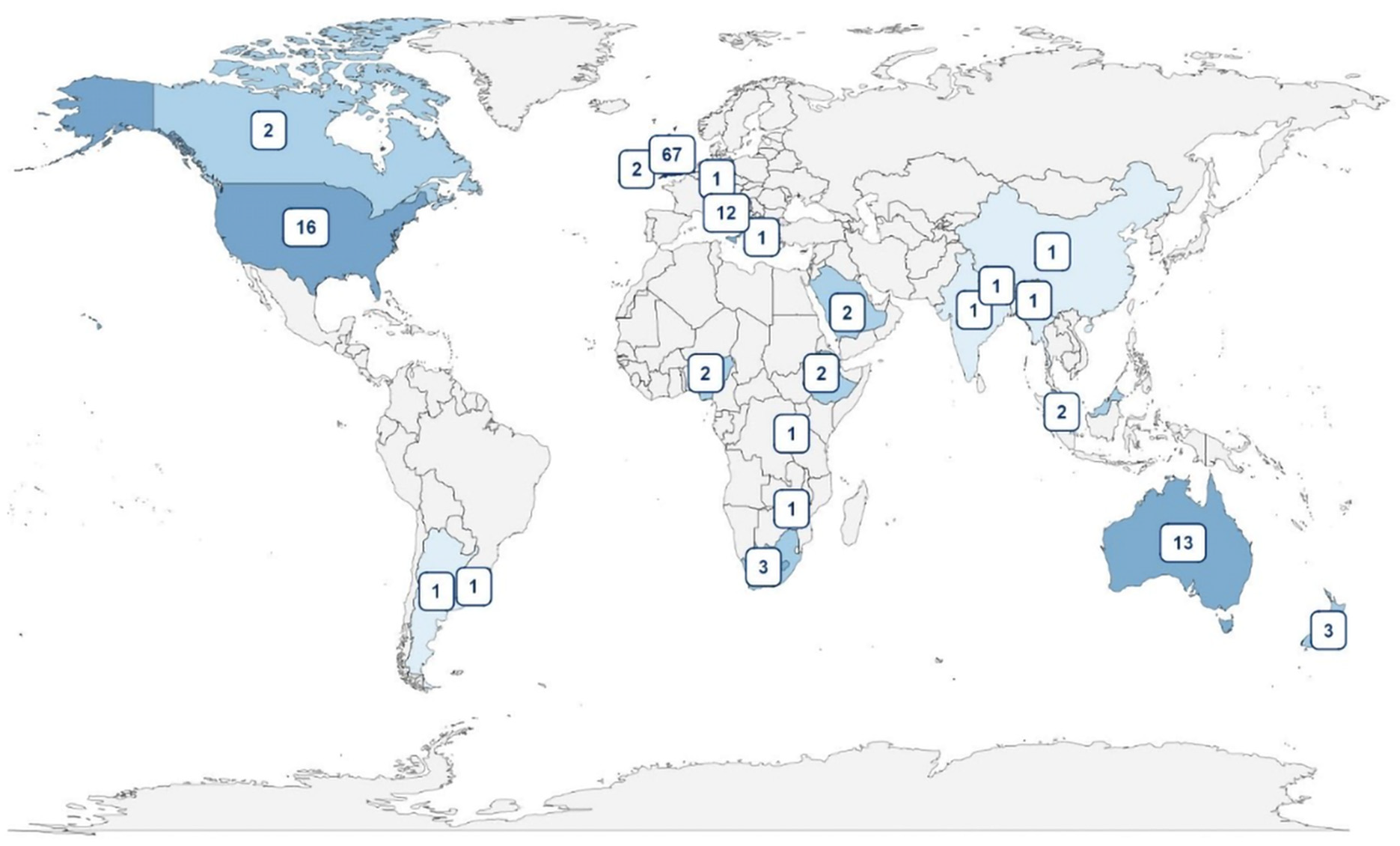
A map showing the distribution of countries of occupation amongst anatomists answering the questionnaire.
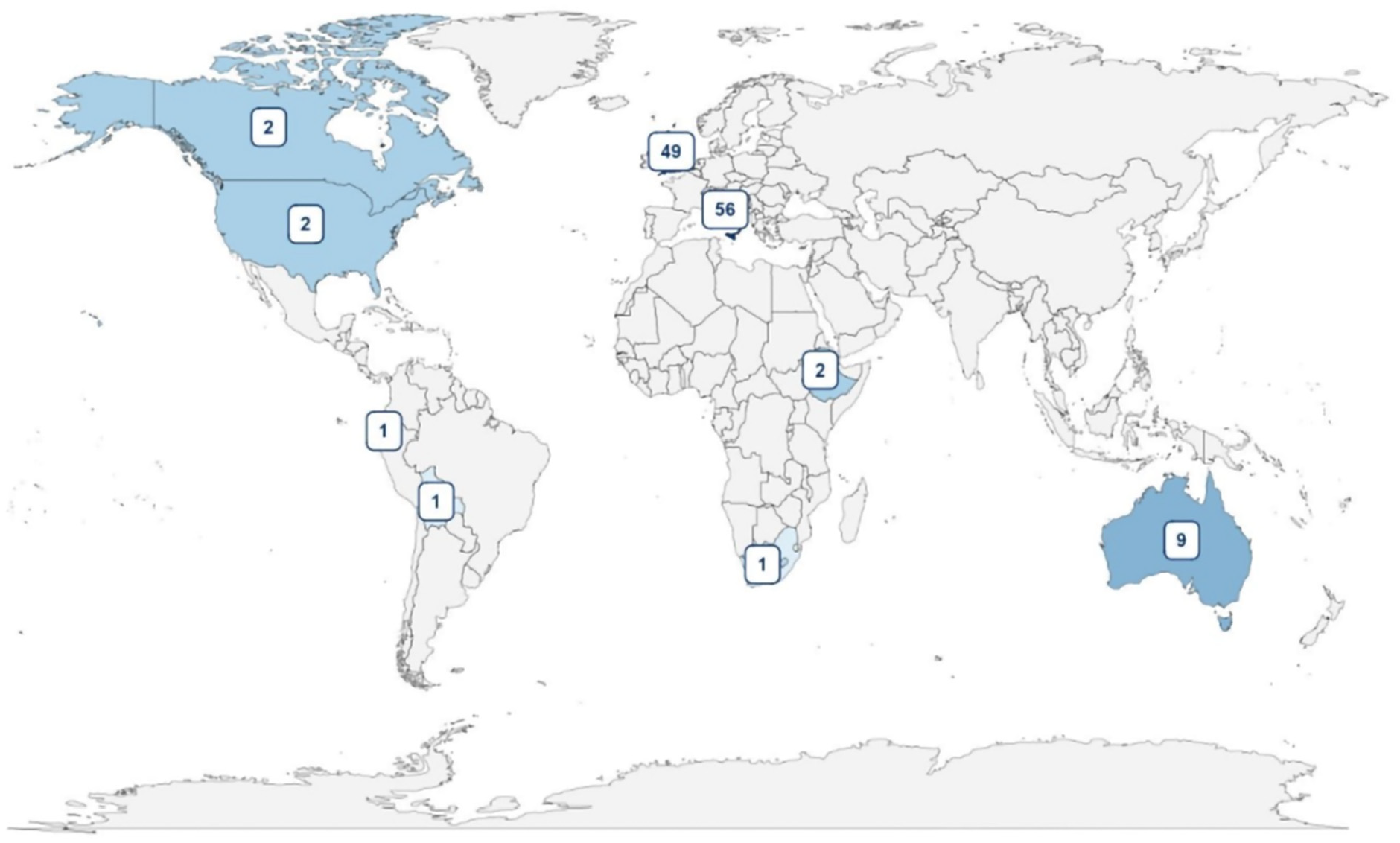
A map showing the distribution of countries of study amongst students answering the questionnaire.
Regarding participant engagement, we had an overwhelming response from anatomists for the focus groups as they were oversubscribed. However, we struggled to recruit for the student focus groups, so £10 Amazon gift card were offered to students that had expressed an interest in participating. Introducing incentives can increase the participation bias of a study and can homogenise the participation pool, thus decreasing diversity in the data (Hsieh and Kocielnik, 2016). Removing the incentive is optimal for obtaining a diverse group of participants, but we have not discovered how best to recruit students to participate in the study yet. Perhaps involving student groups in the recruitment and allowing them to conduct the focus groups for their peers would increase participation. Hsieh and Kocielnik (2016) also suggest offering a variable incentive, which the participant can choose, can increase diversity.
A further challenge is that the research team mostly consists of academics who have busy teaching schedules, meaning there is less time for scholarship, and it can be difficult to keep the momentum of the project. In those instances, it is useful to have a research assistant to share in the data analysis and writing of papers, and to offer administration support where needed. However, a lot of healthcare education research is not supported by funding councils (Jones et al., 2007) and many awards are not sufficient to hire a research assistant for a prolonged period. This also means that although the research assistant role can be flexible, there is not much job stability for individuals in these positions as their work constantly depends on acquiring small pots of funding. This is not inclusive for those researchers who want more stability.
Although using qualitative methods to collect data gave us as rich and unrestricted account of the participants’ experiences, collecting and analysing data in this way presents some consideration points. Firstly, language can be ambiguous, so there is room for misinterpretation from both the participants and researchers, which can ultimately impact the themes created from the data. Our life experiences and personal biases will have also impacted our interpretation of this language; maintaining reflexive accounts of the analytical process helped us to understand exactly how our positionality has affected the research processes and interpretation of the data. In addition, one person’s account is not necessarily representative of a whole population, so without statistical testing to determine the significance, an experience could be an outlier. We must be wary not to assume that because one person in the community has had that experience, everyone else has experienced the same (Ochieng, 2009). Having said that, the nature of this research into lived experiences of inclusivity and representation means that we are interested in and attentive to individual experience, and do not need that experience to be representative whole – rather, inclusivity must work on a case-by-case basis, for all involved. This is why we took a constructionist approach to data analysis in this project – meaningfulness was not overshadowed by frequency.
A further challenge conducting the study arose when we asked participants who contributed to the anatomist questionnaire and focus groups if they would be interested in a toolkit of practical advice to support the creation and continuation of more inclusive curricula. This received an overwhelmingly positive response, as participants identified gaps in personal knowledge as a potential barrier to enhancing inclusivity and particularly to actively introducing inclusive initiatives. However, the dynamic nature of inclusion – or rather, combatting exclusion, makes this a challenging undertaking. Inclusivity is not a fixed concept; it evolves in response to the ever-changing dynamics of society, politics and individual’s beliefs and values. For example, the terminology related to Equity, Diversity and Inclusion (EDI) constantly transforms, posing challenges when trying to stay up to date. A static document would also not allow for the community to be involved in keeping this toolkit relevant, sharing their views, asking questions about its content and seeking support. Conscious of this, the researchers have shifted their focus towards not only developing a toolkit but also establishing an online platform. This platform aims to foster a sense of community among educators who can collectively contribute their ideas and address challenges related to inclusivity in real-time. The ideal platform for the toolkit would be an online community so educators from around the world could participate in its creation and upkeep. However, host platforms cost money so further continuous funding would be needed to set this up and pay for the website fees.
Conclusion: Charting a course for the future of inclusive anatomy education
As this initial phase of our research concludes, we are at the outset of our journey towards understanding and improving inclusivity in anatomy education. As we prepare to publish more data from the project, we look forward to starting important conversations around prescient issues concerning equity in anatomy education, for example, around the fissures between medical education and clinical practice, overcoming the fear of saying or doing the wrong thing in conversations about inclusivity and diversity, and reducing the emotional and time burden of ‘diversity tax’ often unintentionally but unfairly placed on marginalised individuals. For now, our data overwhelmingly indicate that existing medical curricula are failing both anatomists and students, particularly in terms of representation. Although these findings are uncomfortable, with participants expressing justified anger and frustration, we have been encouraged by the medical community’s desire and drive to create an anti-exclusionary culture. These findings, combined with our dedication to action, have yielded productive, positive and tangible outputs ranging from starting challenging conversations around barriers to securing commitments from Adam,Rouilly for greater diversity in skin tones on their models. Not only has a rich body of data been collected which will advance knowledge, but also the research process itself has served as a point of action for anti-exclusion. Collaborations with ACE, Adam,Rouilly and online platforms for learning anatomy are underway, and the data have informed positive changes to the way that anatomy is taught at the Peninsula Medical School. The anatomist focus groups also acted as a forum for action for change in anatomy education. Serving as a supportive space where colleagues across institutions relayed knowledge about and experiences of best and worst practices, shared useful resources, suggested ways to overcome opposition and exchanged thoughts about improving inclusivity in the future. For some, participation in focus groups was itself a powerful act of resistance, as they faced institutional barriers to anti-exclusion and/or had suffered exclusion themselves. For others, participation in the project represented an important early step in their own journey towards more inclusive teaching and learning. Participants confronted gaps in their knowledge, discussed anxieties about getting inclusivity ‘wrong’ or appearing tokenistic, or developed their confidence in recognising, advocating for, and contributing to greater inclusivity in anatomy education. Participation in the project, whether through the questionnaire alone or focus group, helped people to feel seen. Of course, it is not enough to be seen – people must also be heard. The perspectives gathered so far will be transformative in helping us to improve inclusivity in anatomy education, and particularly in developing a toolkit to support educators and learners. But we want to hear more. Specifically, we want to determine what inclusivity in anatomy looks like on a more global scale, and to understand how it might be achieved in local communities. Our present data are predominantly Eurocentric, and as such, have limited application to other countries and cultures. We are currently working with volunteers to translate our questionnaires into other languages, so that we can gather more international data. A more global data set will reinforce the widespread demand for more inclusive teaching resources, both physical and virtual, and add to our understanding of how this varies in different contexts. It will also be critical to the development of our virtual toolkit, helping us to identify and suggest strategies to approach inclusivity in a culturally appropriate, sensitive and impactful way, that prepares learners for clinical practice in global communities. Moving forwards, the project’s growth and sustainability will depend on greater collaboration with our growing international community of researchers, students and educators. Research on inclusivity is not just about findings, but the research process itself, the people who undertake it, and their reasons for doing so. We look forward to the continued impact of this work and the positive transformations it may inspire in the ongoing pursuit of inclusivity.
Supplemental Material
sj-tif-1-mio-10.1177_20597991251313878 – Supplemental material for From attention to action: Advancing inclusivity in the landscape of anatomy education
Supplemental material, sj-tif-1-mio-10.1177_20597991251313878 for From attention to action: Advancing inclusivity in the landscape of anatomy education by Lily Evans, Katie Snow, Aiden Jayanth and Siobhan M. Moyes in Methodological Innovations
Supplemental Material
sj-tif-2-mio-10.1177_20597991251313878 – Supplemental material for From attention to action: Advancing inclusivity in the landscape of anatomy education
Supplemental material, sj-tif-2-mio-10.1177_20597991251313878 for From attention to action: Advancing inclusivity in the landscape of anatomy education by Lily Evans, Katie Snow, Aiden Jayanth and Siobhan M. Moyes in Methodological Innovations
Supplemental Material
sj-tif-3-mio-10.1177_20597991251313878 – Supplemental material for From attention to action: Advancing inclusivity in the landscape of anatomy education
Supplemental material, sj-tif-3-mio-10.1177_20597991251313878 for From attention to action: Advancing inclusivity in the landscape of anatomy education by Lily Evans, Katie Snow, Aiden Jayanth and Siobhan M. Moyes in Methodological Innovations
Supplemental Material
sj-tif-4-mio-10.1177_20597991251313878 – Supplemental material for From attention to action: Advancing inclusivity in the landscape of anatomy education
Supplemental material, sj-tif-4-mio-10.1177_20597991251313878 for From attention to action: Advancing inclusivity in the landscape of anatomy education by Lily Evans, Katie Snow, Aiden Jayanth and Siobhan M. Moyes in Methodological Innovations
Footnotes
Acknowledgements
The authors wish to extend their gratitude to all the participants who generously contributed their time and perspectives to the project. Thanks are also due to the Peninsula Medical School for their financial support of this project, and for creating a research culture that makes space for and celebrates research on inclusivity. The authors additionally wish to thank Professor Gayle Letherby and Dr. Chloe Milsom for their insights on this study. Colleagues at the Anatomy Collective for Equality and Dr. Michael Dillon provided important input at the early stages of this project, shaping our thinking around inclusive questionnaire design. Adam,Rouilly and Primal Pictures are thanked for their enthusiastic ongoing partnership and commitment to improve the diversity of anatomy resources used across medical education. Finally, thank you to the International Federation of Associations of Anatomists for distributing the questionnaire to their member associations and expanding the international reach of the project.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The lead and corresponding authors received financial support from Peninsula Medical School’s Department of Education and Scholarship (DES) to support this research.
Ethics approval
This research has been approved by the University of Plymouth Faculty of Health, Research Ethics and Integrity Committee. The ethical review project ID for this study is 3419.
Supplemental material
Supplemental material for this article is available online.
Notes
Author biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.