
Abstract
Introduction
Burn injuries impose a substantial burden globally, particularly in low- and middle-income countries like Ethiopia, where the impact is pronounced. Despite existing studies on individual patient data, there 's a lack of synthesized evidence on burn injury mortality in Ethiopia. This study aimed to evaluate the combined prevalence of burn-related mortality and its determinants in Ethiopian hospitals.
Methods
A systematic search of various databases yielded 11 relevant studies, which were included in the analysis. Data extraction and quality assessment were conducted using Microsoft Excel 2021 and the Newcastle-Ottawa Scale, respectively. Statistical analyses were performed using STATA version 17 software.
Result
The pooled mortality rate among burn patients in Ethiopian hospitals was determined to be 6.99% (95% CI: 4.8, 9.41). Factors significantly associated with mortality included inadequate resuscitation (Adjusted Odds Ratio (AOR) 3.73, 95% CI: 1.31, 10.58), pre-existing illness (AOR: 5.26, 95% CI: 2.12, 13.07), age <5 or >60 (AOR: 2.22, 95% CI: 1.45, 3.40), and burn injury >20% total body surface area (AOR: 5.17, 95% CI: 2.47, 10.80).
Conclusion
The findings underscore a notably high prevalence of burn-related mortality in Ethiopia, with inadequate fluid resuscitation, pre-existing illness, extreme age, and the extent of injury identified as key determinants. Collaboration among healthcare stakeholders and policymakers is imperative to improve burn care services and mitigate the impact of these injuries. This study was registered with PROSPERO (CRD42023494159), providing a comprehensive overview of burn injury mortality in Ethiopia.
Lay Summary
Burn injuries are a significant health concern globally, particularly in low- and middle-income countries like Ethiopia. Despite the existing studies on burn injuries, there's a lack of synthesized evidence on burn injury mortality in Ethiopia. This study aimed to evaluate the combined prevalence of burn-related mortality and its determinants in Ethiopian hospitals.
The study systematically reviewed 11 relevant studies and conducted a meta-analysis to determine the prevalence of burn injury mortality and associated factors. The pooled mortality rate among burn patients in Ethiopian hospitals was found to be 6.99%. Factors significantly associated with mortality included inadequate resuscitation, pre-existing illness, age <5 or >60, and burn injury >20% total body surface area.
The findings underscore a notably high prevalence of burn-related mortality in Ethiopia, highlighting the need for comprehensive and effective treatment approaches. Inadequate fluid resuscitation, pre-existing illness, extreme age, and the extent of injury were identified as key determinants of mortality. Addressing these factors is crucial for improving burn care outcomes and reducing the burden of burn injuries in Ethiopian hospitals.
This study provides valuable insights for healthcare professionals, policymakers, and researchers working towards improving burn injury outcomes in Ethiopia. By understanding the factors influencing treatment outcomes, healthcare stakeholders can refine treatment protocols, enhance resource allocation, and implement preventive measures to reduce the burden of burn injuries in Ethiopian hospitals.
Introduction
Burns are injuries to the skin or other organic tissues and are generally caused by heat, electricity, or chemical contact. Burn injuries can occur to anyone, anywhere, at any time, with serious risk of morbidity and death. 1 Despite being preventable, burn injuries pose a significant public health concern worldwide, especially in low- and middle-income countries (LMICs), with varying degrees of severity and consequences affecting not only physical but also psychological health. 1 According to a 2019 World Health Organization (WHO) report, 11 million burn injuries occur annually worldwide, and this is associated with 180,000 deaths, the majority occurring in LMICs and almost two-thirds occurring in African and Southeast Asian regions.1,2 In 2019, there were 9.0 million burn cases worldwide and 111,000 deaths, amounting to 7.5 million DALYs (disability-adjusted life years). 3 The WHO estimated that, in Africa specifically, 43,000 people die of burns every year, with a rate of 6.1 per 100,000 people.4,5
According to WHO, burns significantly continue to disability-adjusted life years (DALYs), with a disproportionate impact on LMICs. For instance, among the children who suffer burns in Bangladesh, Colombia, Egypt, and Pakistan, 17% have a temporary handicaps, and 18% have a permanent disabilities. 1 The cumulative impact of burn injuries on the overall disease burden over a lifetime was 1,617,220 Disability-Adjusted Life Years (DALYs) in sub-Saharan Africa and 1,876,506 DALYs in South Asia. 3 The burden of disease and the resulting economic losses for burn injuries are significant worldwide and are disproportionately higher in LMICs. For instance, in 2019, burn-related losses amounted to 11.7 billion USD in South Asia and 6.1 billion USD in sub-Saharan Africa. 3
Despite the launch of the Global Burn Registry (GBR) in 2017 to improve the understanding of burn injuries worldwide, identify prevention targets, and benchmark acute care, burn injuries remain a global concern. 6 Burn injury is very common in LMICs countries, especially in Africa, where over 1 million burns occur each year in sub-Saharan Africa (SSA), leading to significant morbidity and mortality.7–9
Understanding the epidemiology of burns in Ethiopia and the treatment infrastructure available is crucial for gaining insight into the challenges and opportunities for improving patient outcomes in this context. In Ethiopia, burns constitute 1.5% to 9% of injuries across all age groups and 4% to 15% of injuries among children.10,11 According to Ethiopian Demographic and Health Survey (EDHS) 2016 report burn injuries represent 8.7% of all trauma in Ethiopia.12,13 This implies that burns are a significant public health concern, with various factors such as socio-economic conditions, cultural practices, and access to healthcare influencing the epidemiology of burn injuries. Burn management is challenged by various problems in developing countries, especially in SSA, including high incidence of burns, inadequate burn care facilities, and lack of trained staff and resources.14,15 The availability and quality of burn care services in Ethiopia vary significantly between urban and rural areas. Even in urban centers, only one trauma and burn unit is available in Ethiopia which is Addis Ababa Burn Emergency and Trauma (AaBET) Hospital. However, in rural areas, access to specialized burn care is limited, and patients receive initial treatment at local health centers before being referred to regional or national hospitals for further management.13,16,17 The main reported causes of burn in Ethiopia are heat and flame (36%), electric current (31.6%), hot liquid (28.6%), and chemicals (2.7%). 10
Despite the multifaceted outcomes of burn injuries, we aimed to investigate the mortality of burn injuries in Ethiopia. Burn injury mortality is defined as the proportion of deaths among burn injury patients within a specific population over a defined period. Single center studies have reported mortality rates from burn injuries between 1.36% 18 to 21.7%. 19 Such disparities warrant synthesis of evidence from across multiple studies. Burn injury mortality has been reported to be influenced by a complex interplay of factors such as age, comorbidities, injury type and severity, access to specialized care, treatment protocols, and resource availability.18–25 Whether such factors hold the same level of importance in Ethiopian hospitalized cohorts remains to be determined.
Despite the global recognition of burn injuries as a significant public health issue in Ethiopia, there is no comprehensive synthesis of the existing evidence that is imperative to inform targeted interventions. 10 The absence of a systematic review and meta-analysis focusing on burn-related mortality in Ethiopian hospitals limits the development of evidence-based strategies and hinders progress in optimizing patient outcomes and resource utilization. In this review, mortality was used as a measure or outcome variable to assess the overall mortality status of hospitalized population in Ethiopia. The primary outcome, aggregated mortality of burn injury, was explained as the combined mortality rate from multiple studies and was calculated by dividing the total number of deceased patients by the total number of burn injury patients in all reviewed literature, multiplied by 100. This calculation provides insight into the proportion of burn injury patients who succumbed to their injuries, helping to assess the severity and impact of burn injuries on patient outcomes at any period of hospital admission. Moreover, this review is a hospital-based study, investigating burn injury mortality among adult and pediatric inpatients.
Therefore, in this review, we examined the existing literature to quantify the overall mortality rates and factors associated with burn injuries in Ethiopian hospitals to lay the groundwork for context-specific interventions. By synthesizing the findings through a meta-analysis, this study aimed to provide robust evidence for healthcare professionals, policymakers, and researchers working toward improving burn injury outcomes in Ethiopia.
Research questions
What is the aggregated magnitude of mortality resulting from burn injuries in Ethiopia?
Which factors contribute to determining the mortality outcome of burn injuries in Ethiopia?
Methods
Study protocol and registration
This systematic review and meta-analysis aimed to determine the overall prevalence of burn injury mortality and associated factors in Ethiopian hospitals. The results of this review adhered to the recommendations of the guidelines provided in the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) 26 (Online Supplementary Table S1).
Eligibility criteria
Inclusion criteria
All observational studies related to this subject that reported death mortality of burn injuries and their associated factors that were published in English and conducted in Ethiopian Hospitals were included in this review.
Exclusion criteria
Correlational studies, quasi-experimental studies, experimental studies, descriptive studies other than cross-sectional studies, articles without abstract and/or full-text, commentaries, letters, duplicated studies, anonymous reports, editorials, irrelevant topics, research conducted outside Ethiopia, papers with documentation in languages other than English, and qualitative studies were excluded.
Search strategy and selection criteria
Major databases, such as PubMed, Medline, Hinari, Science Direct, African Index Medicus, EMBASE, and Cochrane Library, were searched and accessed from 16 December to 31 December 2023. In addition, gray literature, such as Google Scholar and the repositories of Addis Ababa and Haramaya University, were used as additional sources. Studies with complete reports written in English were retrieved and included in this review. Boolean operators, like “OR” and “AND” were used to combine the following search terms; “Treatment outcome’’ OR “Management outcome’’ OR “Outcome’’ AND “Clinical outcome’’ AND “Burn’’ AND “injury” AND “Epidemiologic factor” OR “associated factor” OR “Factor” OR “Predictor” AND “Public hospital” OR “Government hospital” AND “Ethiopia.” The terms were searched for separately and combined using the Boolean operators. The Co-Co-Pop (Condition, Context, and Population) search strategy was used, in which death outcome/mortality, Ethiopian hospitals, and burn injury individuals represent the condition, context, and population, respectively (Online Supplementary Table S2).
Data extraction and risk of bias (quality) assessment of studies
The data were extracted by two independent reviewers (A.G.B. and O.A.) using Microsoft Excel 2021. Study setting, sample size, population with the outcome of interest, publication year, study period, study design, sampling technique, and all factors affecting mortality from burn injury with lower and upper confidence intervals were extracted. Disagreements at the time of data extraction were resolved through discussion with a third reviewer. The extracted data were imported into the Stata version 17 software for analysis. To assess the quality of each study, we used the Newcastle-Ottawa Scale. 27 This assessment tool consists of three domains: 1) selection (representativeness of the sample, sample size, non-respondents, and ascertainment) with a maximum of five points; 2) comparability (control of the most important factor and control for any additional factors) with a maximum of two points; and 3) outcome (independent blind assessment and statistical testing) with a maximum of three points. The score for each study was calculated on a scale of 0–10, and a score exceeding 7 was deemed ‘good’ and eligible for inclusion in the study (Online Supplementary Table S3).
Outcome measurement
In this review, mortality was used as a measure or outcome variable to assess the overall mortality status of hospitalized population in Ethiopia. The primary outcome, aggregated mortality of burn injury, was explained as the combined mortality rate from multiple studies and was calculated by dividing the total number of deceased patients by the total number of burn injury patients in all reviewed literature, multiplied by 100. The second objective was to establish predictors of mortality from burn injury.
Data analysis
Quantitative meta-analyses were conducted using STATA version 17 statistical software to measure the mortality of burn injury and its determinates. The prevalence of and factors affecting mortality from burn injuries were inconsistent across the included studies. Thus, the individual studies were combined with a random-effects meta-analysis model using the Dersimonian–Laird method. Statistical heterogeneity was assessed using I-squared test statistics and p-values. To identify the source of heterogeneity, subgroup analysis was performed according to region, sample size, publication year, sampling technique, and age. Sensitivity analysis was conducted to assess the impact of each individual study on the combined estimate. To check for publication bias, the Egger's test with a funnel plot 28 was performed. The results of this meta-analysis are presented in tables, funnel plots, forest plots, and narrations.
Results
Search results and article selection
A total of 1251 articles were identified from major databases such as PubMed, Medline, Hinari, Science Direct, EMBASE, Cochrane library, and Google Scholar. Two articles were identified from the local academic databases and repositories of Addis Ababa and Haramaya University, respectively. Of the total identified articles, 247 were excluded because of duplication. After examining the titles and abstracts, 971 articles were excluded. Then, 33 articles were sought for retrieval and 19 articles were retrieved. After assessing for eligibility, eight articles were excluded; three lacked relevant outcomes for this meta-analysis29–31 and five had no full text to access.32–36 Ultimately, 11 full-text articles were included in this review and meta-analysis18–24,37–40 (Figure 1).

PRISMA flow diagram showing screening and selection of studies for the systematic review and meta-analysis of mortality of burn injury and associated factors in Ethiopia, 2023.
Characteristics of the reviewed studies
In this systematic review and meta-analysis, 11 articles with 3010 participants were included. The individual sample sizes for each study ranged from 92 to 423. Almost half of the studies were conducted in Addis Ababa Ethiopia,21–23,37,40 whereas the others were conducted in Northern Ethiopia, 18 Southern Ethiopia, 39 Eastern Ethiopia, 38 Northwest Ethiopia,20,24 and Southwest Ethiopia. 19 All studies employed a cross-sectional design18–24,37–40 (Table 1).
General characteristics of the reviewed studies included in the systematic review and meta-analysis of burn injury mortality in Ethiopia, 2023.

Meta-analysis results
The prevalence of burn mortality in Ethiopia
In this review, the pooled prevalence of aggregated mortality among burn patients in Ethiopian hospitals was found to be 6.99% (95% CI: 4.8, 9.41) using the random-effects model DerSimonian Laird method. This meta-analysis shows that there is a significant level of heterogeneity among studies included in the review (I2 = 90.16%), which was statistically significant (P < 0.001) with a 95% CI, hence a random effect model was used 41 (Figure 2).

A forest plot showing the pooled prevalence of burn injury mortality in Ethiopia, 2023.
Sensitivity analysis
A sensitivity analysis was performed to test for small-study effects in the meta-analysis to estimate the pooled prevalence of mortality due to burn injuries in Ethiopia. The results showed that no individual study influenced the overall pooled prevalence of mortality (Figure 3).

A sensitivity analysis of burn injury mortality in Ethiopia, 2023.
Subgroup analysis
To identify the source of heterogeneity, further analysis was performed using the publication year, region/study setting, sampling technique, age group, and sample size. Accordingly, studies conducted in Addis Ababa were one source of heterogeneity, with pooled prevalence of 6.90% (95% CI :4.22–9.57) and (I2 = 71.35%, P < 0.001). In addition, publication year was another source of heterogeneity, in which studies conducted since 2020 showed pooled prevalence of 6.26% (95% CI: 3.57–8.94) with I2 = 90.82%, P < 0.001). Pediatric age group was also another source of heterogeneity 5.81% (95% CI: 3.10–8.52) with (I2 = 90.41%, P < 0.001) (Table 2).
Subgroup analysis of burn injury mortality by age group, study setting, sample size, sampling technique and publication year in Ethiopia, 2023.

Publication bias assessment
Publication bias was assessed using the Egger's test, revealing a significant result with a p-value of 0.000, indicating the presence of publication bias. However, the Begg's test shows there is no publication bias with P-value of 0.12. Furthermore, a funnel plot was utilized, and asymmetry was observed indicating publication bias. In the funnel plot, the vertical line represents the effect size, while the diagonal lines represent the precision of individual studies, with 95% confidence intervals (Figure 4).
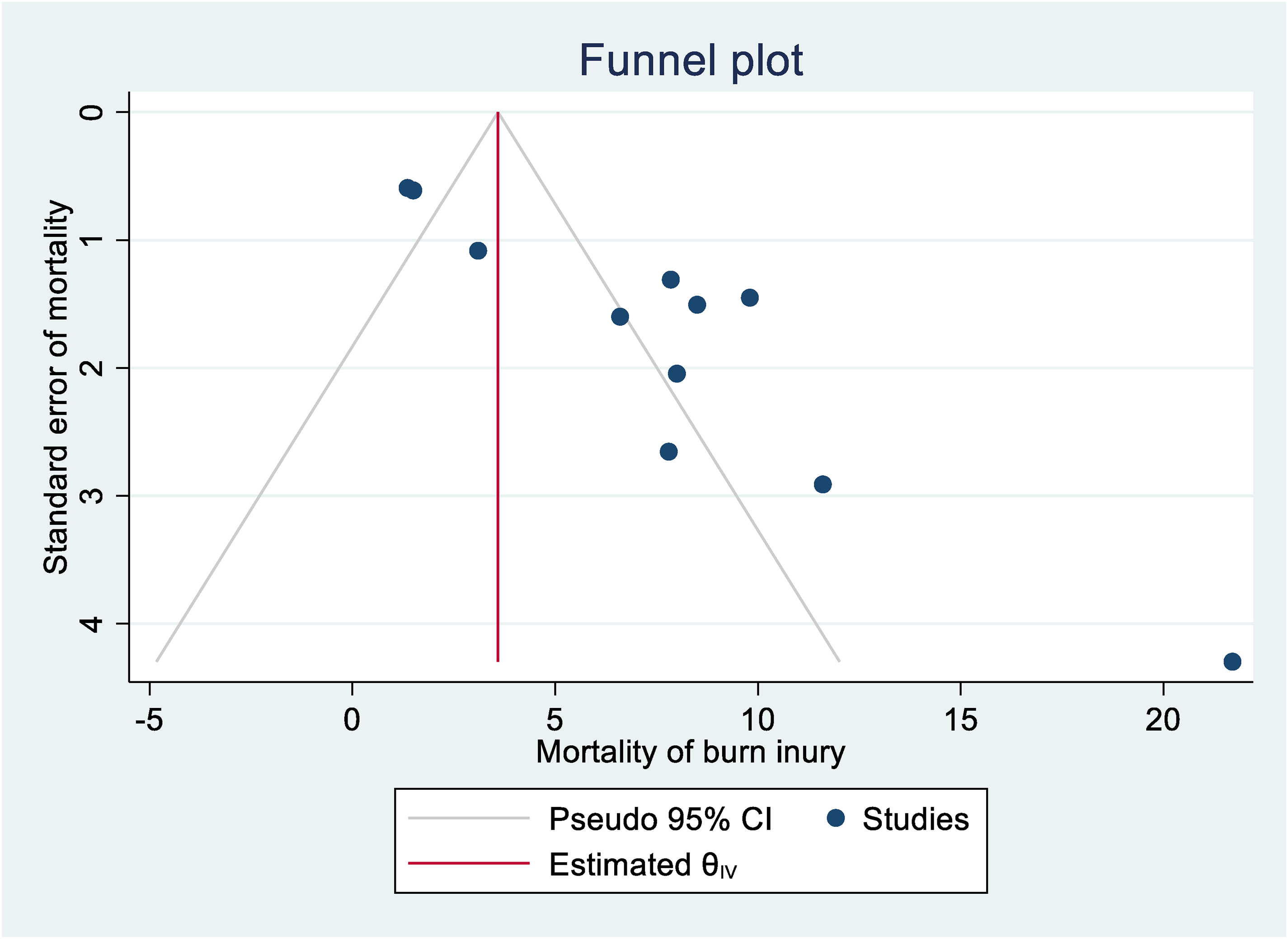
Funnel plot showing publication bias with pseudo 95% CI on mortality of burn injury in Ethiopia, 2023.
Factors associated with mortality of burn injury
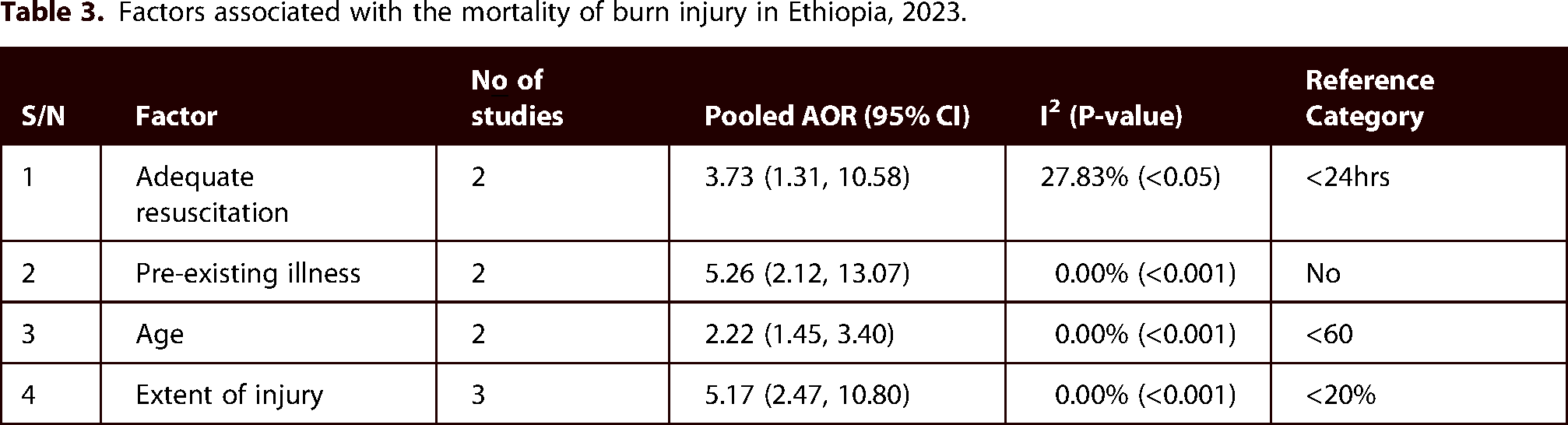
In this meta-analysis, we identified four factors for analysis and found that inadequate fluid resuscitation, pre-existing illness, Age < 5or > 60 years, and extent of injury were positively and significantly associated with the pooled mortality of burn injuries (Table 3). Malnutrition, no insurance, electrical burns, and flame burns were also factors affecting the mortality of burn injuries individually (Online Supplementary Table S4).
Factors associated with the mortality of burn injury in Ethiopia, 2023.
Resuscitation
The pooled effect of two studies in this meta-analysis revealed that patients with inadequate resuscitation within 24 h had 3.73 times higher odds of mortality than their counterparts (Adjusted odds ratio (AOR):3.73, 95% CI: 1.31, 10.58) with mild heterogeneity between studies (I2 = 27.83%).
Pre-existing illness
The pooled effect of two studies showed that those burn patients who had pre-existing illness were 5.26 times more likely to die compared to those who had no pre-existing illness (AOR: 5.26, 95% CI: 2.12, 13.07), with no heterogeneity between studies (I2 = 0%).
Age
Based on this meta-analysis, the pooled effects two studies explained that being aged less than 5 or > 60 had a 2.22 times higher odds of mortality than those individuals who were found in the age range of 5 to 60 years (AOR: 2.22, 95% CI: 1.45, 3.40) with no heterogeneity between studies (I2 = 0%).
Extent of injury
The combined effect of three studies in this meta-analysis demonstrated that those patients with burn injuries of >20% average total body surface area (TBSA) of burn had 5.17 times odds of mortality than those patients with burn injuries of <20% (TBSA) (AOR: 5.17, 95% CI: 2.47, 10.80) with no heterogeneity between studies (I2 = 0%).
Discussion
Burn injuries are a global problem in the WHO-defined African region and bear most of the burden of global morbidity and mortality. Burn-injury mortality is also a priority for Ethiopian health facilities. Enhancing the quality, effectiveness, and efficiency of health services is imperative, and compilation of evidence regarding the level of mortality and associated factors in burn injuries is crucial for achieving this goal. Therefore, this systematic review and meta-analysis was performed in Ethiopia using available small-scale primary studies. In this review, the pooled mortality of burn injuries was found to be 6.99% (95% CI: 4.8, 9.41) meaning approximately 7 out of 100 patients admitted with burn injuries in Ethiopian hospitals die. This result highlights the substantial impact of burn injuries on patient outcomes, emphasizing the need for comprehensive and effective treatment approaches associated with burn care in Ethiopian hospitals.
The finding is in line with the study conducted by Opriessing et alin Austria in 2023, in which the mortality of burn injuries were in Europe (12.40%), South and Middle America (10.60%), Australia (7.5%), Asia (6.76%) and North America (5.0%). 42 However, this result is lower than that study conducted by the same author in Austria, in which the largest proportion of deaths was recorded in Africa (23.5%), surpassing the global prevalence (18.27%). 42 This was also lower than the study conducted in Iran (14.23%). 43 The reason for this difference could be that study setting in which papers from low- and middle-income nations could not be found, and the majority of the papers in this study came from Addis Ababa, Ethiopia, where burn centers provide the majority of specialized care compared to other regions. This implies that the presence of specialized burn centers in Addis Ababa most likely contributes to lower mortality rates. The fact that the research came from both ordinary hospitals and specialized facilities hampered the ability to compare various investigations. In Iran, a large number of participants were included (n=61,662) and the study period was long (10 years).
The results of this study are also lower than the review study conducted in sub-Saharan Africa, with mortality of 17%. 15 This difference may originate from the sample size, in which a total of 54 publications with 32,862 participants were included in the scope of the study; the publications came from 14 countries with three sub-regions – western, eastern, and southern Africa–and the year of study, and as mortality due to burn injury has decreased in recent years.
Currently, there is a general decline in the mortality rates and admissions for burn injuries. 11 According to the Global Burden of Disease Project, there was a 6% decrease in burn mortality globally, even in the short timeframe between 2000 and 2004.11,44 In another review of 22 studies from 13 countries, a decrease in burn-related mortality was reported. 45
In contrast to this, only 2% of worldwide deaths occur in high-income nations (HICs), which include the Americas, the Eastern Mediterranean, and the Western Pacific. The regions’ respective mortality rates are 1.3, 0.02, and 0.6%. This was also higher than the review study conducted in United Kingdom (1.59%). 46 The reduction in mortality rates of burn victims in HICs is attributed to recent advancements in burn care, including improved fluid replacement therapy for resuscitation, enhanced intensive care, and nutritional support. 47
Factors influencing treatment outcomes in Ethiopian hospitals were also explored. Inadequate fluid resuscitation significantly increased mortality, with patients lacking timely resuscitation having 3.73 times higher odds of death. This emphasizes the critical role of timely and appropriate fluid resuscitation in improving the survival rate of patients with burns. This finding is similar to that of the Global Review Study conducted in 2017, in which advancement in burn care, including improved resuscitation of burn victims through fluid replacement therapy, specialized facilities, and intensive care, reduced burn-related mortality. Inadequate fluid resuscitation in burn patients is typically defined based on the failure to meet key physiological goals and outcomes associated with fluid management such as urinary output and improvement in metabolic parameters.45,47
In this meta-analysis, those with pre-existing illnesses had 5.26 times higher odds of mortality than those without pre-existing illnesses. This implies that individuals with preexisting health conditions face additional challenges when dealing with burn injuries. Chronic diseases can compromise the body's ability to respond effectively to trauma, potentially exacerbating the impact of burn injuries and increasing the risk of fatal outcomes. This is consistent with a review conducted in Europe, in which chronic illnesses were the major risk factors for mortality due to burn injuries. 48
Age proved to be a crucial factor influencing burn injury outcomes, with individuals aged less than 5 or > 60 years exhibiting 2.22 times higher odds of mortality than those aged between 5 and 60 years emphasizing the vulnerability of the very young and elderly populations. Understanding age-related variations in response to burn treatment is essential for tailoring interventions to specific age groups. This result is in agreement with a study in Europe, in which older age was associated with a higher risk of death. 48 The association between older age and death could be explained by the general physiological vulnerability that is often accompanied by aging. Older individuals may have weakened immune systems, reduced organ function, and slower healing processes, rendering them more prone to complications from burn injuries. 49 Another review also supported that those under five years of age have a high risk of mortality from burn injuries. 50 Children under the age of five have less developed physiological systems, including the skin, which is less resistant to burns. Their skin is thinner, making them more prone to injury, and their bodies have a higher surface-area-to-volume ratio, making them more prone to fluid loss and heat-related complications. 51
Patients with burn injuries covering more than 20% TBSA had 5.17 times higher odds of mortality than those with injuries affecting less than 20% TBSA. This result aligns with that of a study conducted in Europe, in which individuals with a higher percentage of burned surface area had a high risk of mortality. 48 This may be because larger burn areas can lead to more severe physiological stress, fluid loss, and a higher risk of infection, contributing to a higher likelihood of mortality. 52
Additionally, individual factors such as malnutrition, lack of insurance, and electrical and flame burns were identified as independent contributors to the mortality of burn injuries. This is in accordance with previous studies in which the type of burn (electrical), low economic status, and nutritional support contributed to an increased burn-related mortality rate.45,47,50 This is unsurprising, given that electrical burns are known to pose an elevated likelihood of death due to the unique nature of electrical injuries causing both external and internal damage, affecting vital organs and leading to complications such as cardiac arrhythmias, respiratory distress, and neurological issues. 53 Low economic status, and no medical insurance, can influence burn-related mortality in several ways, such as by hindering access to quality healthcare and delaying treatment. 54 Nutritional support also plays a significant role in burn-related mortalities. Malnutrition can compromise the body's ability to heal, impair immune function, and increase the susceptibility to infections. 55
Limitation
Conducting a systematic review of the mortality due to burn injuries and associated factors in public hospitals in Ethiopia is a valuable endeavor. However, as in any study, some limitations should be considered when interpreting the findings. The limitations of this meta-analysis include the number of articles/studies reported, and the fact that the associated factors considered in the studies may not cover the entire spectrum of variables influencing burn injury mortality. Additionally, the severity of burn injuries can vary widely, which may not be consistent across studies. The variability in burn severity can affect the generalizability of our findings. Finally, owing to the small number of articles available, we are unbale for further discussion.
Implication of the study
The findings of this systematic review and meta-analysis have significant implications for health care practices in Ethiopian hospitals. By identifying the prevalence of mortality and its associated factors, this study helps healthcare providers to make informed decisions to enhance burn care. The study highlights the urgent need to refine treatment protocols based on empirical evidence, optimize resource allocation to critical areas, and implement effective preventive measures to mitigate the burden of burn injuries. Fostering interdisciplinary collaboration among surgeons, nurses, and emergency care providers is crucial for a holistic approach to burn management.
Conclusion
In conclusion, this systematic review and meta-analysis provides insights into the treatment outcomes of burn injuries in Ethiopian hospitals, emphasizing the prevalence of mortality and associated factors. These findings emphasize the importance of addressing inadequate fluid resuscitation, pre-existing illnesses, age-related vulnerabilities, and extent of injury in burn care protocols. By leveraging this knowledge, healthcare stakeholders can collaboratively enhance the quality of burn care services and mitigate the impact of burn injuries on individuals and communities. Establishing regional pediatric burn units and tailoring interventions for individual risk factors can enhance the overall effectiveness of burn treatment strategies, ultimately improving patient outcomes in Ethiopian health care settings.
Supplemental Material
sj-docx-1-sbh-10.1177_20595131251321772 - Supplemental material for Treatment outcome and associated factors of burn injury in Ethiopian hospitals: A systematic review and meta-analysis
Supplemental material, sj-docx-1-sbh-10.1177_20595131251321772 for Treatment outcome and associated factors of burn injury in Ethiopian hospitals: A systematic review and meta-analysis by Asnake Gashaw Belayneh, Ousman Adal, Sosina Tamrie Mamo, Alamirew Enyew Belay, Yeshimebet Tamir Tsehay, Henok Biresaw Netsere, Sileshi Mulatu, Gebrehiwot Berie Mekonnen, Wubet Tazeb Wondie, Tiruye Azene Demile, Gebremeskel Kibret Abebe and Mengistu Abebe Messelu in Scars, Burns & Healing
Footnotes
Acknowledgements
We thank the authors and publishers for providing open-access articles for reviewing this study.
Authors’ contribution statement
A.G.B., O.A., and A.E. were involved in conceptualization, protocol development, study selection, data curation, formal analysis, and editing of the final draft of the manuscript. A.G.B., O.A., Y.T.T., M.A., and S.T. were involved in the data extraction, quality assessment, and analysis. S.M., W.T., G.B., T.A., G.K., and H.B. participated in the validation, analysis, drafting, and editing of the manuscript. All the authors approved the final manuscript.
Data availability
The datasets used and analyzed during the current study are available from the first author upon reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.