
Abstract
Purpose
The average life expectancy in Japan is 81.47 years for males and 87.57 years for females, which is expected to increase, and this has led to an increase in the number of patients aged ≥80 years with burns requiring hospitalization. Herein, we investigated the factors that affect the survival and length of hospital stay of patients aged ≥80 years with burns requiring hospitalization.
Major findings
The participants were patients admitted to our facility between 1 January 2008, and 31 December 2018. Deceased patients had significantly higher burn index, prognostic burn index, total body surface area, and revised Baux score, indicating the severity of burns; moreover, they had a lower Barthel index at admission and higher rates of inhalation injury and dementia. Regarding the length of hospital stay, patients with a higher burn index, prognostic body index, total body surface area, and rBaux scores took a longer period from admission to reach sitting and standing positions, and those who had buttock burns had significantly longer hospital stays.
Conclusions
In patients aged ≥80 years, higher mortality rates were associated with more severe burns, lower activities of daily living at admission, inhalation injury, and dementia. The length of hospital stay was longer in patients with severe burns, buttock burns, and inability to achieve early mobilization.
Lay summary
We investigated the factors influencing the survival rate and hospital stay duration among patients aged 80 years and older who required hospitalization for burns. We compared the records of surviving and deceased patients admitted to our hospital between 2008 and 2018. Our findings revealed that deceased patients experienced more severe burns, reduced activities of daily living at admission, and higher rates of inhalation injury and dementia. Furthermore, patients with severe burns had longer hospital stays, a longer period from admission to sitting and standing, and more frequently had buttock burns. These results indicate that burn severity, activities of daily living, inhalation injury, and dementia are critical factors in the treatment of burns in older patients.
Keywords
Introduction
Patients aged >65 years with burns account for <5% of burn patients in Asia and 20% in the United States. Older adults in Japan numbered 11.6 million in 2020, accounting for 9.2% of the total population, and this percentage is increasing yearly. 1 In Tottori Prefecture, where our hospital is located, people aged ≥80 years accounted for 10.3% of the population in 2017, which was higher than the national average for that year. 2 Of all patients admitted to our hospital with burns, 11% were aged ≥80 years. Older adults are more susceptible to injury due to their slow reaction time, sensory disturbance, medication side effects, and deterioration of cognitive function.3–6 Generally, the hospitalization rate is high, 7 and the length of hospital stay is long. 8 The mortality rate is high when the burn area is extensive or when inhalation injury or severe complications occur.9–12 However, not all older adult patients with burns experience poor outcomes. Nevertheless, few studies have investigated burns in patients aged ≥80 years. In the present study, we aimed to investigate the factors affecting the survival rate and length of hospital stay in patients aged ≥80 years with burns.
Materials and methods
This was a retrospective study.
Participants
The study included 40 patients aged ≥80 years who were hospitalized for burn treatment during the 11-year period between 1 January 2008, and 31 December 2018. All such patients hospitalized for burn treatment in our hospital were included except three patients: one patient with cardiopulmonary arrest at admission, one who died the day after admission, and one who was hospitalized due to extensive cerebral infarction. This study was approved by the institutional review board and ethics committee of our institution (approval no. 21A159). The study conformed to the ethical guidelines of the Declaration of Helsinki for research involving human subjects. All participants or their family members provided written informed consent.
Methods
We recorded the age, sex, length of hospital stay, burn index (BI: Superficial Dermal Burn + Deep Dermal Burn/2 + Deep Burn), prognostic burn index (PBI: BI + age), total body surface area (TBSA), revised Baux score (rBaux score), Barthel index at admission, inhalation injury, dementia, buttock burns, the period from admission to initiating nutrition administration, the period from admission to achieving a sitting position, the period from admission to achieving a standing position, and the period from admission to surgery.
Fisher's exact test and the Mann–Whitney U test were used to compare surviving and deceased patients. Spearman's correlation coefficient and the Mann–Whitney U test were used to investigate factors related to surviving patients.
All statistical analyses were performed using EZR (version 1.61, Saitama Medical Center, Saitama, Japan). 13 EZR is statistical software with extended R and R commander functions. Statistical significance was assumed if two-tailed P-values were <0.05.
We accessed the data for research on 29 April 2019, and did not have access to information that could identify individual participants during or after data collection.
Results
The patients’ mean age was 85.2 (80–97) years, with 14 males and 26 females. The mean length of hospital stay was 54.0 (2–290) days, BI was 14.4 (0–90), PBI was 99.59 (80–178), TBSA was 18.31% (0–92%), rBaux score was 106.89 (84–197), and Barthel index at admission was 22.64 (0–80). Eight patients had inhalation injury, 12 had dementia, and 17 had buttock burns. The mean period from admission to initiating nutrition was 3.18 (0–22) days, the mean period from admission to achieving a sitting position was 12.0 (0–126) days, and the mean period from admission to achieving a standing position was 13.9 (0–135) days. In the 28 patients who underwent surgery, the mean period from admission to surgery was 14.7 (0–71) days (Table 1). Regarding outcomes, 18 patients were discharged, 17 were transferred (of whom seven were later discharged, and 10 were transferred to other facilities), five died, four developed sepsis, and one experienced shock.
Background of 40 burn patients aged ≥80 years who were hospitalized.
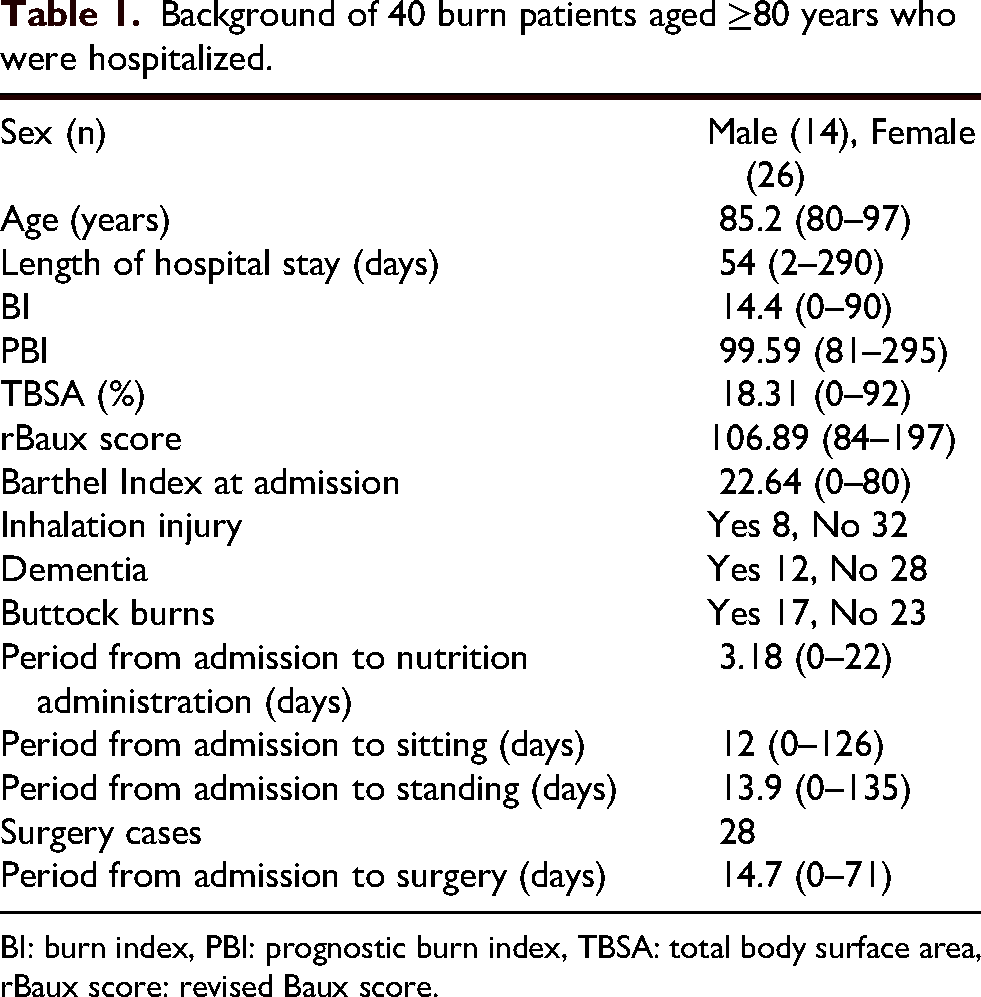
BI: burn index, PBI: prognostic burn index, TBSA: total body surface area, rBaux score: revised Baux score.
Comparing the surviving and deceased cases, no significant differences were observed in age (P = 0.15), sex (P = 1), the period from admission to surgery (P = 0.62), or buttock burns (P = 0.14). In contrast, significant differences were noted in BI (P < 0.01), PBI (P < 0.01), TBSA (P < 0.05), rBaux score (P < 0.01), Barthel index at admission (P < 0.05), presence of dementia (P < 0.05), and presence of inhalation injury (P < 0.05) (Tables 2 and 3).
Comparison of surviving and deceased cases.

IQR, Interquartile Range.
BI: burn index, PBI: prognostic burn index, TBSA: total body surface area, rBaux score: revised Baux score.
Comparison of surviving and deceased cases.

M: male, F: female.
Regarding the length of hospital stay, there were no significant differences in terms of age (P = 0.56), sex (P = 0.72), Barthel index at admission (P = 0.12), presence of dementia (P = 0.29), presence of inhalation burns (P = 0.36), the period from admission to initiating nutrition (P = 0.95), or the period from admission to surgery (P = 0.52). In contrast, significant differences were observed in BI (P < 0.01), PBI (P < 0.01), TBSA (P < 0.01), rBaux score (P < 0.01), the period from admission to sitting (P < 0.01), the period from admission to standing (P < 0.05), and buttock burns (P < 0.01) (Tables 4 and 5).
Comparison of length of stay in surviving cases using Spearman's correlation coefficient.

BI: burn index, PBI: prognostic burn index, TBSA: total body surface area, rBaux score: revised Baux score.
Comparison of length of hospital stay (days).
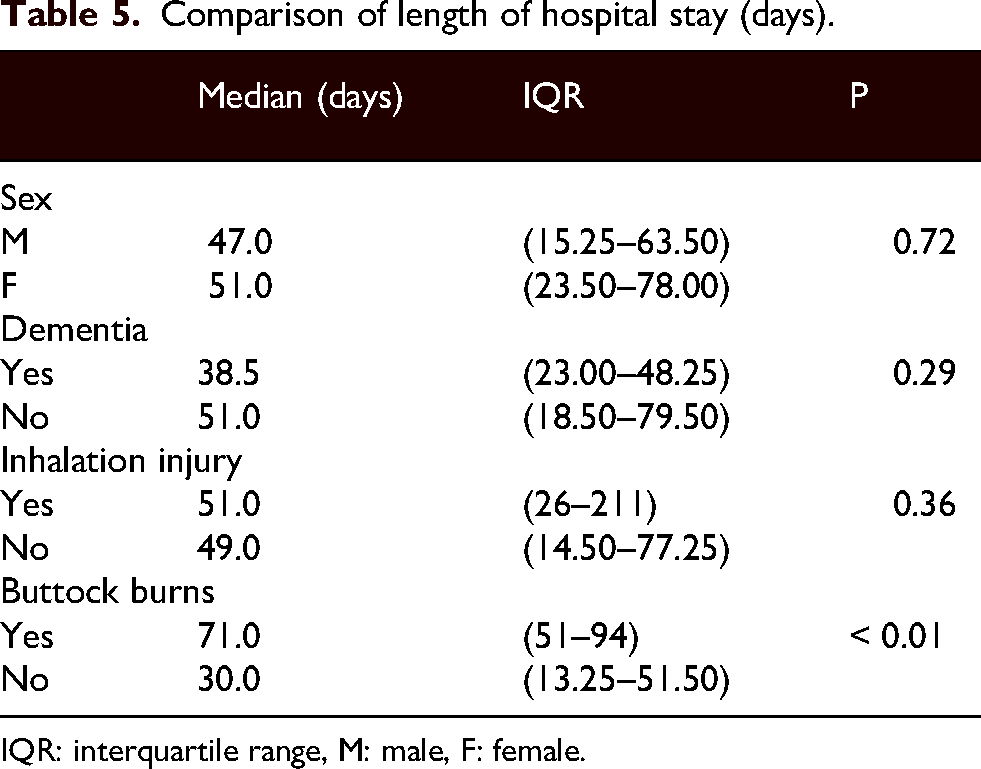
IQR: interquartile range, M: male, F: female.
Discussion
Compared to surviving patients, we found that deceased patients had significantly higher BI, PBI, TBSA, and rBaux scores, indicating a high severity of burns; in addition, they had a lower Barthel index at admission and higher rates of inhalation injury and dementia.
In Japan, BI and PBI14–16 are commonly used to measure burn severity. However, we could not accurately judge the depth of burns at admission because burns are progressive after injury, and even burn specialists have difficulty assessing second- and third-degree burns immediately after the injury.14,17,18 BI and PBI are not widely used in other countries for judging severity 19 ; assessments are based on TBSA6,12,20–25 and rBaux score26,27 indexed by age, airway burns, and TBSA. The results of deceased patients from our hospital revealed significantly higher BI, PBI, TBSA, and rBaux scores compared to those in survivors. We found that older patients with widespread burns had a high mortality rate. This finding agrees with that of previous studies showing patients with severe burns to have a high mortality rate.6,12,21,24,26,28–30 Larger burns and older age have also been shown to increase the risk of death.31,32
In our study, patients with burns who had dementia had a significantly higher mortality rate than those without dementia. This is in agreement with previous studies demonstrating that the mortality rate of burn patients increases in patients with a mental illness. 33 The mortality rate triples because of dementia 33 and worsens when TBSA increases in patients with mental illness. 34 However, one study has reported that, although dementia onset increases in older adults, and patients with dementia have a tendency toward a wider burn area, there is no significant difference in the survival rate. 33 At our hospital, we found no association between dementia and TBSA; therefore, this does not explain the higher mortality rate in patients with dementia. In patients with dementia aged ≥65 years, the duration of hospitalization is reportedly more than doubled. 33 However, we found no significant difference in length of hospital stay between patients with and without dementia.
In our study, factors associated with a longer hospital stay included higher BI, PBI, TBSA, and rBaux scores, a longer period from admission to sitting or from admission to standing, and buttock burns. However, the length of hospital stay was not significantly associated with age, duration from admission to initiating oral/enteral nutrition, Barthel index at admission, period from admission to surgery, or presence of inhalation injury.
Our results confirm that the length of hospital stay increases with increases in the burn area and severity in older adults. This is in agreement with studies demonstrating that higher degrees of burns are associated with longer hospital stays in patients with moderate-to-severe burns.35,36 Among older adults, a greater extent of third-degree burns correlates with a longer length of hospital stay in patients aged >60 years. 37 In a study of patients aged ≥55 years, the burn area was greater, and the hospital stay was significantly longer. 38 A previous study reported that the number of complications in older adults correlated with the length of hospital stay 39 ; therefore, other medical conditions should also be considered. The length of hospital stay was significantly longer in the patients with buttock burns. This could be because the length of hospital stays for those aged ≥80 years reportedly depends on the number of surgeries, 22 and patients with buttock burns could have required more surgical procedures than those without buttock burns. 40 One study reported that the length of hospital stay was longer among hospitalized older adults 17 ; however, there was no increase for those aged ≥80 years in our hospital.
We could not find any study correlating activities of daily living (ADLs) on admission with mortality. The deceased patients in our study had poor oxygenation and ventilation and severe pain and dyspnea at admission, so they were administered sedatives and analgesics; therefore, their Barthel index was low. The Barthel index at admission was not associated with any significant survival difference; however, there was a significant difference in the period from admission to sitting or standing. Patients who achieved early rehabilitation had an improved Barthel index and a shorter length of hospital stay. At our hospital, we have recently encouraged patients to get out of bed and ambulate. Research shows that the survival rate can be improved through multidisciplinary rehabilitation. 12 Early rehabilitation interventions shorten the length of hospital stay, 41 and the patients in our study who could sit and stand early had a shorter length of hospital stay. It seems that if the patient can get out of bed soon after hospitalization, the length of stay shortens. In patients aged ≥75 years, recovery of physical and psychosocial function continues for up to 1 year after injury. 42 Continuous rehabilitation is also essential and may be important for older adult patients with burns.
A previous study reported that the length of hospital stay was longer for patients with inhalation injuries22,38; however, no significant difference was observed in our study. This may be because most of the patients with respiratory tract burns that we encountered in our hospital had minor injuries, requiring shorter length of hospital stays. In contrast, inhalation injuries are typically more severe, require extensive hospitalization, and have a higher mortality rate.
We found no significant difference in the period from admission to surgery between surviving and deceased patients. This may be because the period to surgery was ≥2 weeks, and no surgery was performed in the hyperacute phase. Early surgery within 24–48 h43–46 and surgery with intensive care within 72 h 39 have been shown to improve the survival rate in adults aged >65 years. 39 Reducing the period from admission to surgery (for example, from 14.76 to 6.12 days) and early surgery within 48 h have also been shown to shorten the length of hospital stay.12,43–46 In contrast, in a study of cases excluding inhalation injury, the mortality rate increased significantly in the group that underwent surgery within seven days compared to the group that underwent surgery after seven days. 47 Another study reported that early surgery does not necessarily shorten the length of stay in patients aged ≥65 years. 12 In our hospital, the mean period from admission to surgery was quite long, at 14.7 days. Two patients with severe burns did not undergo surgery and died because the policy was not to perform surgery until blood pressure increased after receiving fluids.
No difference was observed between the period from admission to initiating oral/enteral nutrition and the length of hospital stay. Malnourished patients are twice as likely to die and have longer hospital stays than well-nourished patients. 48 The lack of difference between them is likely because, in our hospital, we initiate oral or enteral nutrition as soon as possible for severe patients.
This study had some limitations. First, the sample size was small, and no sample size calculation was performed. Second, the retrospective study design carries inherent limitations and risks of bias. Third, there is a potential for selection bias.
Conclusion
Among patients aged ≥80 years, mortality is high in those with more severe burns, lower ADLs at admission, inhalation injury, and dementia. The length of hospital stay is longer in those with severe burns, buttock burns, and the inability to perform early mobilization.
Footnotes
Acknowledgments
We thank the people who provided guidance and encouragement while preparing this manuscript. We sincerely thank Professor Takahiro Ueda, Department of Emergency and Disaster Medicine, Tottori University School of Medicine, for his guidance. We also thank the Emergency and Disaster Department for their efforts in treating the burns.
Author contributions
T.O.: Conceptualization, Writing – review & editing; T.U.: Supervision; N.M: Data curation; Y.O.: Data curation; M.H.: Supervision.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.