
Abstract
Introduction
Burns are most prevalent in low- and middle-income countries but the risk factors for burn contractures in these settings are poorly understood. There is some evidence from low- and middle-income country studies to suggest that non-medical factors such as socio-economic and health system issues may be as, or possibly more, important than biomedical factors in the development of post-burn contractures.
Methods
Four cases are presented to illustrate the impact of non-biomedical factors on contracture outcomes in a low-income setting. The cases were drawn from participants in a cross-sectional study which examined risk factors for contracture in Bangladesh.
Discussion
The two cases had similar burns but different standards of care for socio-economic reasons, leading to very different contracture outcomes The two cases both had access to specialist care but had very different contracture outcomes for non-medical reasons. The risk factors and contracture outcomes in each case are documented and compared.
Conclusion
The impact of non-biomedical factors in contracture development after burns in low- and middle-income countries is highlighted and discussed.
Lay Summary
Burns are common in low- and middle-income countries (LMICs) but the risk factors for burn contractures in these settings are poorly understood. Burn contractures are formed when scarring from a burn injury is near or over a joint and results in limited movement. There is some evidence from LMIC studies which suggests that non-medical factors such as socio-economic (e.g., household income, level of education) and health system issues (e.g., whether specialist burn care could be accessed) may be as, or possibly more, important than non-medical factors (such as the type and depth of burn and the treatments received) in the development of contractures following burn injuries.
Four cases are presented to illustrate the impact of non-biomedical factors on contracture outcomes in a low-income setting. The cases were drawn from participants in a larger study which examined risk factors for contracture in Bangladesh. Two cases had similar burns but different standards of care and different outcomes. Two cases had similar access to specialist care but very different outcomes for non-medical reasons. The risk factors present and contractures outcomes in each case are documented and compared.
The importance of non-biomedical factors in contracture development after burns in LMICs is highlighted and discussed.
Introduction
Burn contractures can be a common morbidity following burn injury and may have a considerable negative impact on a person's quality of life, with wider implications for the family and society.1–6 Contractures reduce available range of movement (ROM) and function and are often a source of pain, visible difference, and disability.7–10 Despite the impact and frequency of burn contractures, surprisingly little is understood about the prevalence and determinants of burn contractures in low- and middle-income countries (LMICs). 11
Most studies of risk factors influencing burn contractures are from high income countries (HICs) and focus on biomedical factors. Some factors are reported to increase contracture risk (such as deep burns, high total burn surface area (TBSA) and intensive care unit (ICU) stay, while others may have a protective effect in reducing contracture development (such as early skin grafting, appropriate positioning/splinting, and early physiotherapy.12–21 There is little or no published information about the relative weight of different risk factors, nor about how their interplay may affect outcomes. 11
Studies exploring contracture risk factors in LMICs are few, 11 but review of the available literature indicates that contracture outcomes are not only related to biomedical or treatment factors, but also to socio-economic and health system factors, which are not routinely considered in HIC literature.22–25 The authors recently conducted a cross-sectional study in Bangladesh to analyse the effect of 48 potential risk factors on major joint contracture outcomes; 22 contractures were defined as any loss of measured ROM as a result of scarring in at least one plane of movement of any major joint at risk. In that population, anatomical joint location, socio-economic factors and health system factors were significantly related to contracture occurrence and/or severity, while other accepted biomedical risk factors were not (Table 1). 22
Risk factors examined in the cross sectional study from which Cases 1–4 were selected. 22
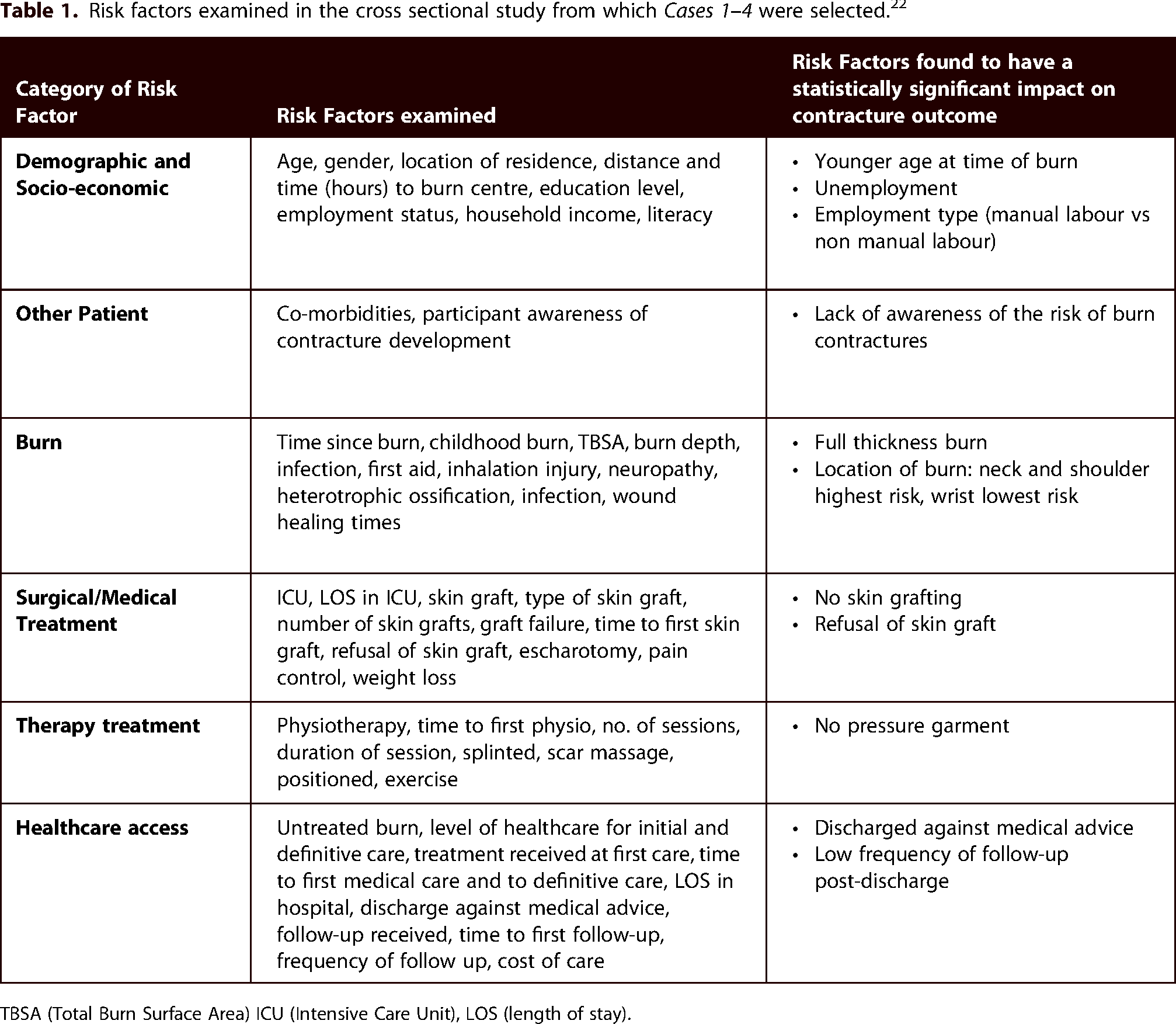
TBSA (Total Burn Surface Area) ICU (Intensive Care Unit), LOS (length of stay).
This article presents the details of four participants from a previous study in Bangladesh, 22 to illustrate how contracture outcomes can vary in patients with similar burns, highlighting those non-burn and non-medical risk factors which likely affected the outcomes.
Method
The original cross-sectional study was conducted at Dhaka Medical College Hospital (DMCH) and the Sheikh Hasina National Institute for Burn and Plastic Surgery (SHNIBPS) in Bangladesh in late 2019. 22 Risk factor data were collected on 48 participants with 126 major joints at risk through semi-structured interviews using interpreters. Eligibility criteria and recruitment for the study are explained in more detail elsewhere. 22
For illustrative purposes, Cases 1 and 2 were selected because they had burns of similar location, size, and age, but had access to different levels of care resulting in very different outcomes. Cases 3 and 4 both had similar deep burns with early access to specialist care, but had very different outcomes for other reasons. Contracture risk factors are described for each participant, highlighting those factors which may have contributed to the different outcomes. Data presented for all four reported cases were extracted from the same database used to complete quantitative analysis for the cross-sectional study. 22
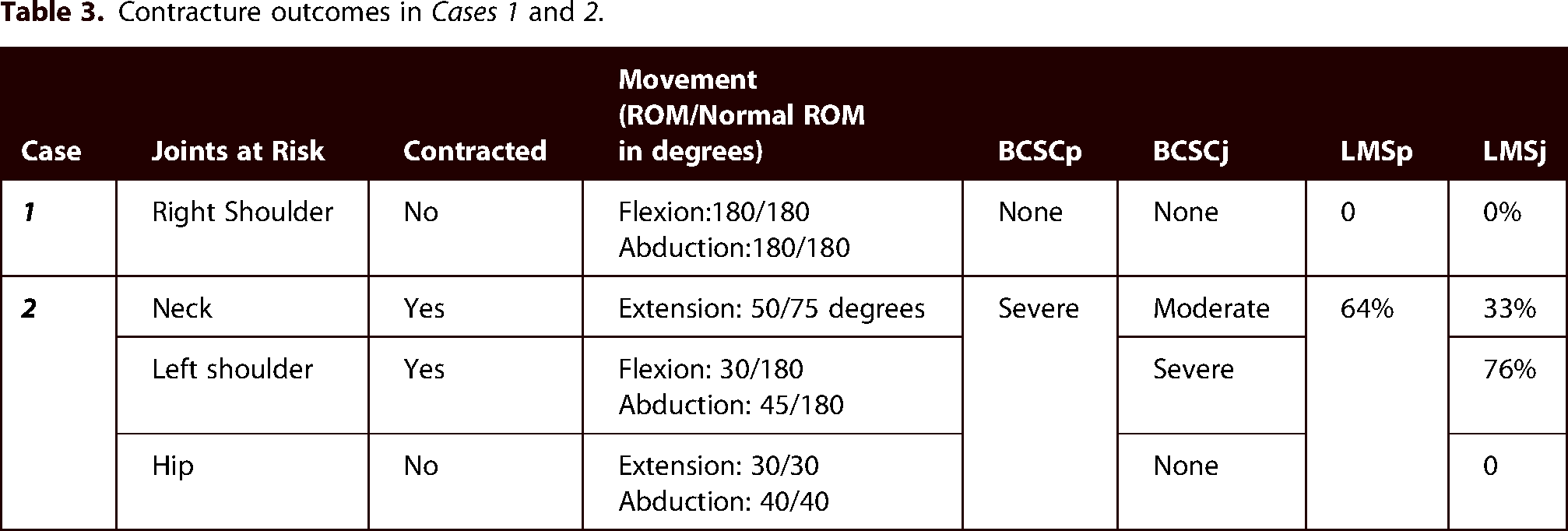
Contracture was defined as any measured loss of movement due to scarring in at least one plane in a major joint at risk as described in the main study. 22 Contractures were graded in severity using both categorical and continuous scales at both whole person and individual joint levels (Table 2); 22 these outcomes are reported for each of the cases presented.
Categorical (BCSC) and continuous (LMS) outcome measures used.

Ethical approval for the main study was granted by Swansea University (230719b) and by the Ethical Committee of DMCH/SHNIBPS.
Results
Cases 1 and 2: Similar burns but different treatment
Case 1 was female, 27 years old at the time of interview, lived in Dhaka (one hour from DMCH/SHNIBPS), was married, and had no children. She had been educated to Honours level and worked in Marketing. The combined household income (between herself and her husband) was 120,000 BDT/month (equivalent to £1021/month) which is much higher than the reported average monthly household income in Bangladesh (22,574 BDT, equivalent to £175/month). 26 She had no previous medical history and had full range of movement in all joints prior to the burn.
Case 2 was also female, was 18 years old at the time of interview, had no previous medical history and had full range of movement in all joints prior to her burn. However, she lived in a rural area in Mymensingh Region (180 kms and 7-h single journey from SHNIBPS) and was not married. She was non-literate and had not attended any education. At the time of interview, she was unemployed, her father was a street seller and the household income was 5000 BDT/month (equivalent to £43/month).
Both women had sustained significant flame burns of 15–30% TBSA 9–18 months prior to evaluation, but their treatment journeys and outcomes were very different.
Case 1 received appropriate first aid (immediate application of water) and presented immediately to a private hospital in Dhaka where she was admitted. Although the hospital was not a specialist burn service, her consultant was an experienced Burn and Plastic Surgeon who also worked in a Government specialist burn service.
She did not have an inhalation injury or require any ICU stay or escharotomy. She had no infection or weight loss during the acute period. Her pain was well-managed with paracetamol and injections for any procedural pain. She underwent excision and grafting to all areas of the burn nine days after admission. All wounds healed within two to three weeks of the skin graft (four to five weeks post-burn).
Effective positioning (90 degrees of shoulder abduction) and effective shoulder exercises were initiated on day 1 of admission and were adhered to throughout her admission. She did not wear a splint. Pressure was worn over the graft donor site, but not over the burn scar. All therapeutic interventions during her admission were provided by the treating doctor; no in-patient physiotherapist was involved. The patient did not have any specialist psychosocial support, apart from the support of her family and the treating doctor.
Her length of stay (LOS) in hospital was 26 days. On discharge, she had weekly follow-ups for 20 weeks with the treating doctor. She continued with positioning advice for six weeks after discharge and also did axillary stretches, creamed the scar, and wore a silicone gel sheet over the scar. She had one consultation with a physiotherapist at 28 days post burn, but felt she was managing independently and did not require further physiotherapy. The overall cost of her care was 650,000 BDT (equivalent to £5530).
In contrast, Case 2 received no specialist burn care. Her mother provided appropriate first aid (immediate application of water) and she was taken on the day of the burn to the local District Hospital where she had basic care only (fluids and dressings). No skin grafting was offered. Doctors advised her to transfer to DMCH for further care, but she was unable to do so due to lack of funds. After 15 days in the District Hospital the patient went home.
At home, ointment was used on the wounds, but she had no dressings and no further medical input. The wounds were reported to have taken eight weeks to heal. It is not known if there was any wound infection or whether she lost any weight during the healing of the burn. She had no splinting, pressure, scar massage, or positioning of any joints at risk. She was not assessed or treated by a physiotherapist. She kept her arm by her side and did not move it because the pain was too great. The costs of her care are unknown.
In addition to these marked differences in care, there were also differences between these two patients in terms of their awareness of the potential for subsequent contracture complications. Case 1 had heard the word “contracture” early in her care from her treating surgeon, and she was very aware that a contracture could develop following a burn injury. She believes that she did not develop a contracture as she adhered fully to her doctor's advice to avoid any risks. Conversely, Case 2 was not aware that a contracture could develop, and neither she nor her father had heard of one. Her father believes she got the contractures due to “lack of treatment”.
Outcomes
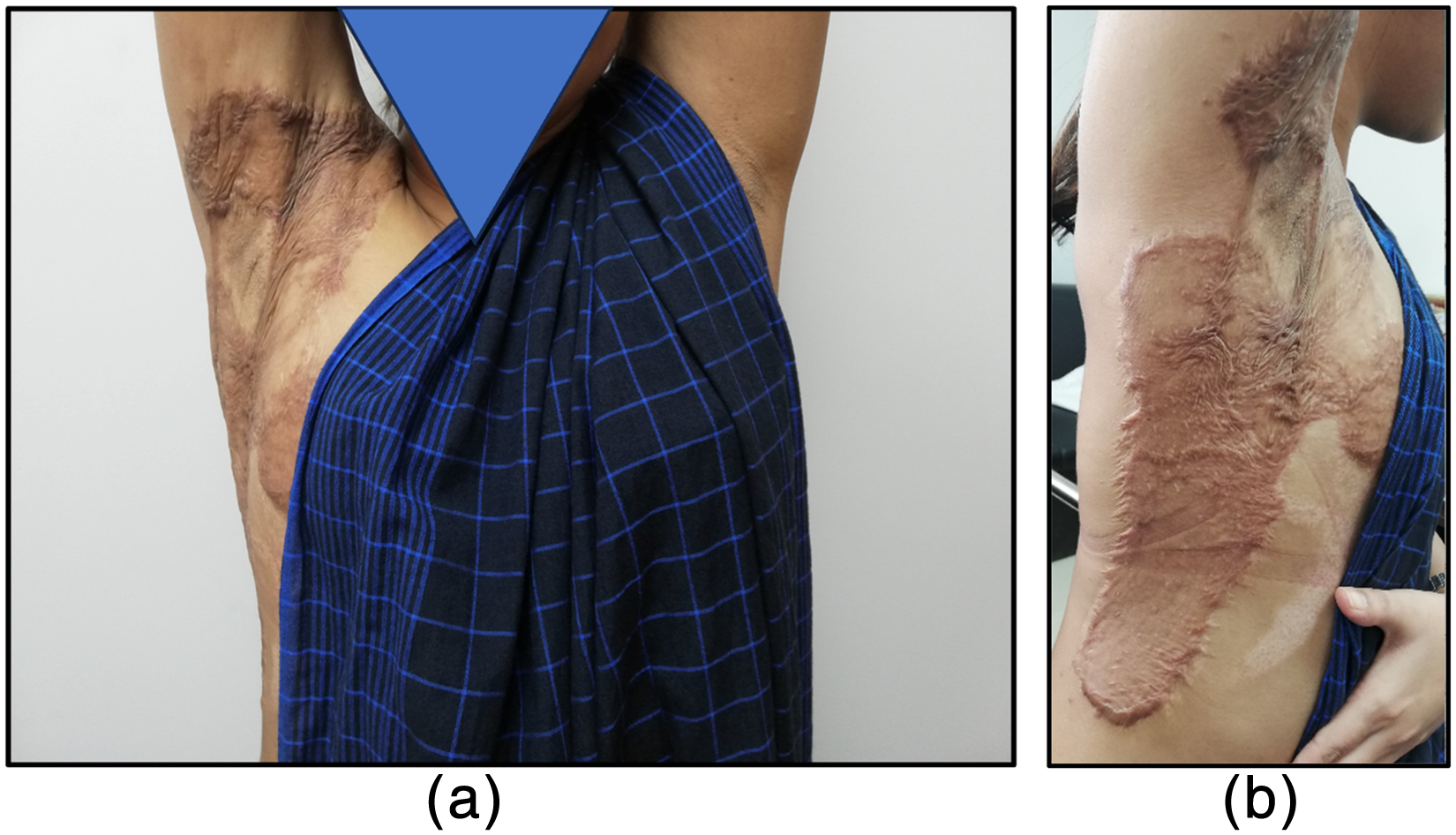
The outcomes for Case 1 are illustrated in Figure 1 and detailed in Table 3. She had full movement of her right shoulder in all measured ranges, equivalent to the movement available in her left shoulder. She had no pain and moved to the end of range at her shoulder with ease. Her scars were pliable and and non-vascular. In contrast, Case 2 had extensive and severe scarring over the burned areas. Two of her three joints at risk were contracted with significant loss of movement (Figure 2, Table 3). The scarring was very rigid; active and passive ROM were equal; no improvement in range of movement would be possible without surgical intervention.
(a) Anterior view demonstrating full ROM Case 1. (b) Lateralview of right shoulder demonstrating full shoulder abduction Case 1.

(a) Anterior view of left shoulder demonstrating maximum available shoulder abduction Case 2. (b) Lateral view showing maximum available left shoulder flexion Case 2.
Contracture outcomes in Cases 1 and 2.
Cases 3 and 4: Similar burns with specialist treatment
Case 3 was male and 40 years old at the time of interview. His injury was a full thickness 21% TBSA flame burn to both upper limbs, sustained eight months previously. He lived in a rural area within Dhaka District (38 kms and 1 h from DMCH) with his wife and four children. He had been a rickshaw puller prior to the injury but subsequently became an auto-rickshaw driver as this involved less manual work. He had no education and was non-literate. He was the head of the household and earned 10,000 BDT/month (equivalent to £85/month). Prior to the burn he had no past medical history or any loss of range of joint movement.
Case 4 was female and 25 years old at the time of injury and interview. She also lived in a rural area, two hours from DMCH. She was a married housewife with one new-born child; her husband was garments worker, and the household income was 15,000 BDT/month, equivalent to £128/month. She had studied to secondary school level, had no previous medical history and had full range of movement in all joints prior to the burn. Nine months prior to interview, she sustained a 15% TBSA full thickness flame burn to her chest, flank and both axillae.
Case 3 received appropriate first aid (immediate application of water) and presented immediately to DMCH. He did not have an inhalation injury but reported a four day stay in ICU which was confirmed by medical notes. Due to the depth of burns on his right upper limb, escharotomy was required. Four weeks post-admission he had a skin graft to all affected areas of his right arm (sheet graft over the anterior aspect of his elbow and meshed skin grafting over the remainder); there was no graft failure. All wounds were healed by two months.
His pain was well managed with injections of paracetamol or diclofenac five to six times/day as required. He did have a wound infection; he knew this because he had to purchase ‘special’ antibiotics for infection, and medical notes reported pseudomonas infection. He reported that he did lose weight through the acute phase, but he was not able to specify the loss.
Although Case 4 did not have appropriate first aid (egg was applied to burn), she sought immediate medical care at her local Medical College Hospital where she received basic care and was referred to DMCH, arriving on the day of injury. She had an inhalation injury (confirmed by medical notes), but no ICU care or escharotomy was required. Her chest and shoulder wounds were grafted two weeks after admission; there was no graft failure. A second skin graft was advised for the remaining wounds, but this was refused by the patient and family due to lack of funds and because she had a baby at home. The grafted area took four weeks to heal, and the remaining areas took four months to heal.
In contrast to Case 3, Case 4 reported experiencing very severe pain which made her feel unable to move. She reported that she did not have any wound infection. She lost weight over the acute period but was unsure of how much.
Case 3 was discharged two months post-burn and had his first physiotherapy contact at this time (day 60 post-burn). He was advised on effective positioning on day 1 of admission by the doctor, and strictly adhered to the positioning advice for two months. He had been advised on appropriate exercise by his doctor, which involved flexing and extending his elbows and wrists through full range of movement, which he completed three to four times a day. He was advised to start scar massage at four months, which he adhered to. He had no splint or pressure garments. There was no input from a counsellor or psychosocial support. He had four follow-ups, the first at six weeks post-discharge; at each appointment he saw the physiotherapist for 10 min. The cost of his care was 300,000 BDT, equivalent to £2552.
Case 4 was discharged against medical advice after 14 weeks; she reported she left hospital because she did not have sufficient funds, she could not afford further surgery, she needed to care for her three-month-old baby at home and that she did not feel that the nursing staff treated her with dignity. She did not have any physiotherapy; although she was advised about positioning and exercise by the doctor, she was in too much pain to implement either. She was advised to purchase an axilla splint, but did not have funds for this. She reported the lack of funds and need to care for her baby as the reasons for not returning for follow-up. She had no input from a counsellor and the cost of her care was unknown.
Case 3 was aware that a contracture could develop following a burn injury. He was very definite about the reasons for his good outcome, which were that he had early surgery, knew the doctor personally, fully trusted all the instructions he was given and followed them exactly; he understood the importance of moving and therefore took as much pain control as needed. He reported that knowing the doctor personally had the greatest impact on his good outcomes.
Case 4 had heard of the word contracture before and was aware that that a contracture could develop following a burn injury, but did not know why she had developed the contractures.
Outcomes
Contracture outcomes for Case 3 are illustrated in Figure 3 and summarised in Table 4. Invariably, elbow contractures are flexion contractures, and some degree of full extension is lost. However, this participant had full extension of his elbow and only lacked 35 degrees of elbow flexion. The lack of flexion was not due to a contracture, but to a thick scar in the anterior aspect of the elbow which formed a mechanical ‘block’ to full elbow flexion.
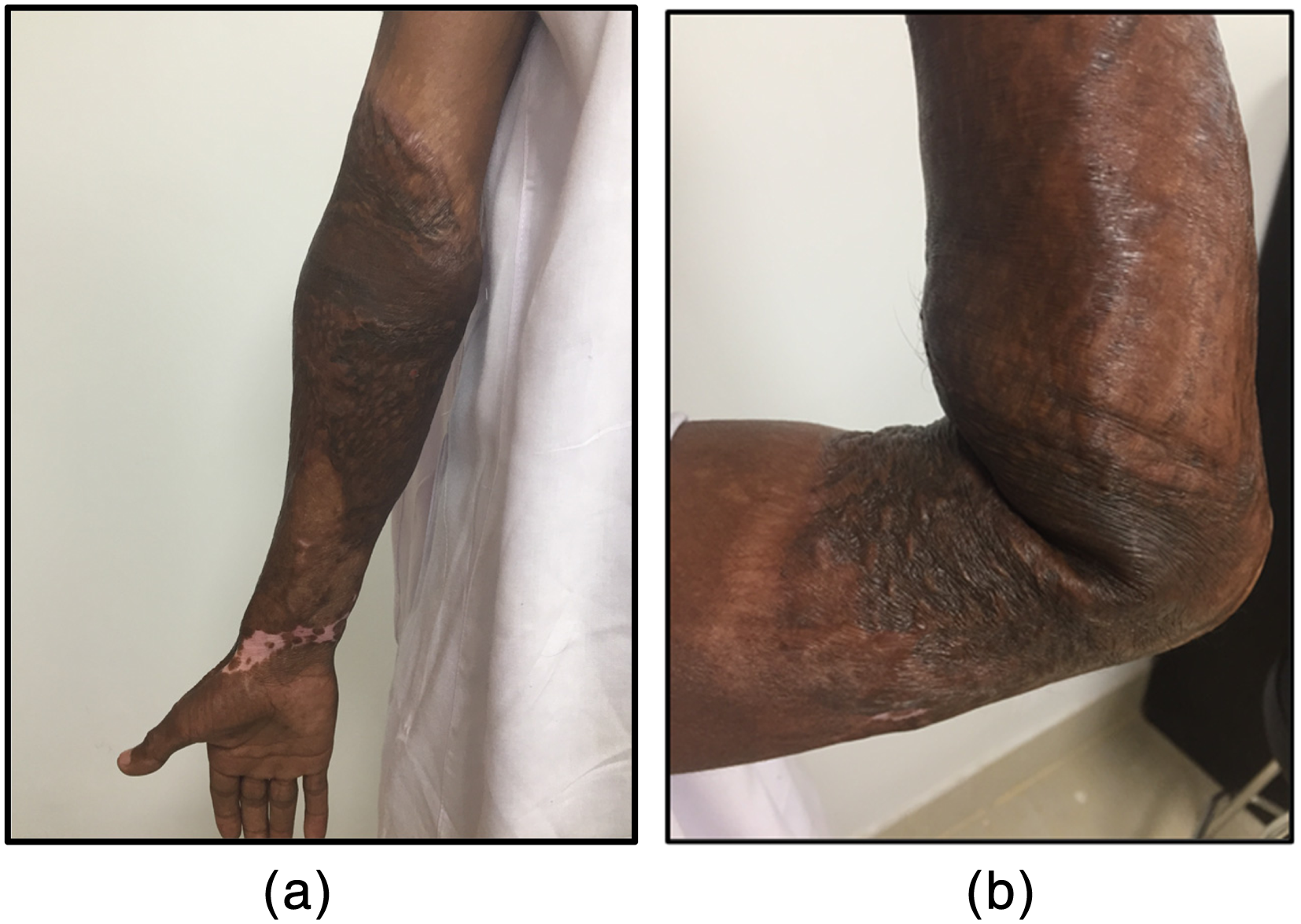
(a and b) Distribution of scarring and available ROM Case 3. (a) Anterior view of right elbow, arm demonstrating full elbow extension. (b) Lateral view demonstrating maximum available elbow flexion ROM.
Contracture outcomes in Cases 3 and 4.

In contrast, Case 4 had loss of movement at both shoulders. She had severe contractures of her right shoulder as shown in Figure 4; she was unable to lie flat on a hard surface due to tightness across her chest and shoulders. The measured outcomes for Case 4 are presented in Table 4. Although only nine months post-burn at the time of assessment, her contractures were fixed, and no further movement was available; for any improvement, surgical intervention would be required.

Summary of risk factors and outcomes
Table 5 summarises the main recognised risk factors for contracture in all four cases. Although those with poor outcomes (Cases 2 and 4) had a greater number of statistically significant risk factors as determined by the previous study 22 (unemployed, full thickness burn, burn to the shoulder, lack of/refusal of skin grafting, no pressure garment, discharged against medical advice, low frequency of follow up) and no rehabilitative input, those with good outcomes also had several factors which might have been expected to adversely affect their outcomes (Case 1: full thickness burn and a burn to the shoulder; Case 3: manual employment, full thickness burn, no pressure garment).
Comparison of main risk factors in Cases 1–4.

*Factors found to be statistically significant in previous study. 22
The main areas of difference between the cases with good outomes vs those with poor outcomes were in their socio-economic status, their distance from specialist care, whether they had skin grafting and rehabilitation advice (even if not from a physiotherapist), completion of medically-advised care and follow-up attendance.
Discussion
These four case studies illustrate how risk factors for contracture are complex and interconnected. In low-income settings where access to specialist care is not universal, outcomes are often determined by patients’ social status and ability to pay for necessary care. Even with access to timely, appropriate specialist care, outcomes may still be poor due to the influence of other non-surgical factors such as poverty, poor pain control, lack of awareness of the possibility of contracture development, and the nature of the doctor-patient relationship.
Cases 1 and 2 had similar burn risk factors for contracture; both were young females who suffered deep flame burns to similar areas of the chest and shoulder. However, the acute burn care and rehabilitation therapy offered to Case 1 was far superior to that of Case 2. Despite a lack of formal physiotherapy input and a full thickness burn into her axilla and trunk, Case 1 had an excellent outcome. Conversely Case 2, who had a burn of similar distribution and depth, only had limited and non-specialist care and a very severe contracture outcome. The lower socio-economic status and educational level of Case 2 almost certainly impaired her ability to access appropriate specialist care and follow-up. The much greater awareness and concern about contracture development demonstrated by Case 1 probably also had a positive effect on her adherence to her doctor's instructions.
Cases 3 and 4 were both able to access specialist care at DMCH immediately after injury, had similar lengths of stay and early grafting. Their socio-economic factors were also similar although Case 4 had a higher educational level and a greater household income than Case 3, and might have been expected to have had a better result. The reported inhalation injury of Case 4 (recognised as a risk factor for poor outcome 13 ) was not sufficiently severe to warrant an ICU stay but Case 3 required an ICU stay and escharotomies, both of which might have been expected to negatively affect his outcome. However, at nine months after injury, Case 3 had regained virtually full movement of his affected joints; despite having a similar burn, specialist care and fewer recognised risk factors, Case 4 had a much worse outcome, with severe limitation of movement in two of her three joints at risk.
The main areas of difference between Cases 3 and 4 were in their adherence to post-graft advice and rehabilitative therapy. Case 3 appeared to have had adequate pain control, had a good relationship with his doctor and followed all advice given. Although initiated late, he was also seen by a physiotherapist. In contrast, Case 4 discharged herself against medical advice because of financial constraints, maternal responsibilities and perceived lack of empathy from clinical staff. She had no follow-up and received no physiotherapy advice or treatment. High levels of pain in hospital and at home undoubtedly contributed to her reluctance to move, exacerbating her risk of contracture.
Cases 1 and 3 also demonstrate that non-specialist and Government hospitals can produce excellent outcomes. Both of these patients ascribed considerable importance to their good relationships with their doctors, which resulted in assiduous treatment adherence. In contrast, despite both having treatment in a Specialist Burn Centre, Case 3 had a good relationship with his healthcare staff, while Case 4 did not. The relationship between patients and their treatment provider(s) has not yet been explored as a risk factor for burn contracture formation; it may be of particular importance in LMICs where care is less standardised and could be investigated further.
Pain and nutrition have been reported as risk factors for burn contractures; 11 in the previous cross-sectional study 22 both were explored in the interviews as referenced in Cases 1–4. However, neither could be included in the quantitative analysis because these risk factors are continuous and difficult to define retrospectively; the long post-injury period (mean 2.5 years) and the continuously variable nature of pain and nutrition during this period made it impossible to quantify pain or nutritional status at any defined point. Pain control is likely to be an important contracture risk factor, particularly in low-income settings where patients have to pay for all medication; more detailed qualitative or longitudinal studies will be required to accurately capture the impact of pain control and nutritional status on contracture development.
All four case studies highlight the importance of treatment adherence in contracture prevention, which is unsurprising. However, poor adherence with treatment recommendations is not a simple matter of patient will or desire; many factors may contribute to a patient's inability to comply with medical advice in a low-income setting, including poor pain control, fear, lack of trust, lack of awareness of potential consequences, lack of funds and competing pressures such as the needs of other family members. Even one such non-medical factor can negate the benefits of the best specialist care; in low-income settings. such adverse influences are widespread.
Selecting particular participants to use as exemplars is always subject to bias, however these cases were selected from first hand experience of similar burns with very divergent outcomes. The limitations of the main study are covered elsewhere 22 and clearly still apply in terms of selecting from a relatively small number of participants. The purpose of these case studies is simply to add some human details to the complexity of risk factors for contracture in LMICs.
Burns are a global problem, and most frequently occur in LMICs;27–29 it follows that contractures are also likely to affect many LMIC burn survivors, although data on actual prevalence and severity of contractures in LMICs are lacking. 11 Contractures cause not only profound human suffering, diminished function, disfigurement, and social isolation,2,5,7,30 but also result in ‘catastrophic expenditure’ on healthcare (>10% annual expenditure 31 ) for many of the families affected. In the study population from which these illustrative cases were drawn, 22 the costs of care incurred by the participants, even before any reconstructive surgery, ranged from 3 – 125 times the annual family income. 22 Such financial burdens, along with the decreased individual and family earning capacity which often accompanies burn injuries, diminishes not only individual and family financial security but may reinforce the low-income status of a nation through reduced productivity.32,33In the two cases where costs of care were reported, Case 1 (private care) incurred treatment costs 5x her total monthly income, and Case 3 (treated in a Government hospital) paid 30x his total monthly income.
Contracture prevention is therefore likely to be much better and more cost-effective than cure, not only for affected individuals but also for society. Studies of contracture risk factors in low-income settings are few; most research is from HICs 11 where access to standardised and specialist burn care, education, socio-economic and psychological support is much greater, if not universal. While some of the identified non-surgical factors are outwith the control of burns clinicians, others are not; better patient information about the risk of contracture, adequate pain control and advice on movement can all be provided at little expense by clinicians without specialist knowledge, even in low-income settings. Specialist Burns Centres could contribute by emphasising these issues to general clinicians working in more rural settings though outreach educational programmes and agreed clinical protocols. More focused LMIC research is required to clarify the interplay between biomedical, socio-economic, and other non-medical risk factors for contracture in LMICs; until this is achieved, even the best efforts of burn care clinicians are likely to be undermined.
Future research in this area should include a robust qualitative approach, so that in considering risk factors from quantitative data we do not lose sight of the human experiences during treatment journeys. Qualitative research is likely to be useful in exploring the complex interplay of risk factors and the ways in which important social, economic and demographic features can influence outcomes; it may be particularly useful in low resource settings where prospective quantitative studies are challenging to conduct. Recommendations for future studies to examine risk factors for burn contractures are made by these authors elsewhere.11,22,34, 35
Conclusion
The four cases presented demonstrate how contracture severity after burns in a low-income setting can be influenced not only by access to optimal specialist care, but also by non-medical factors such as socio-economic status, pain control, patient awareness, and the nature of the doctor-patient relationship. Until such factors are recognised and considered, contracture prevention in LMICs is likely to be limited, with subsequent adverse effects on individuals, families, and societies. Given the high incidence of burns in LMICs, much more research into contracture prevention in these settings is required.
Footnotes
Acknowledgements
This study would not have been possible without the help of the participants, their relatives and the staff at DMCH/SHNIBPS who gave freely of their time and shared their experiences.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the National Institute for Health Research (NIHR) (project reference:16.137.110) using UK aid from the UK Government to support global health research. The views expressed in this publication are those of the author(s) and not necessarily those of the NIHR or the UK government.
How to cite this article
Fanstone R and Karim Khan MR. Risk factors for burn contractures in a lower income country: four illustrative cases. Scars, Burns & Healing. Volume 10, 2024. DOI: 10.1177/20595131241236190. Scars, Burns & Healing. Volume 10, 2024. DOI: 10.1177/20595131241236190.