
Abstract
Background
Keloids are elevated, painful scars that extend beyond the original wound's boundaries and can cause significant emotional distress for patients. While combining surgical excision with radiation therapy has shown potential in treating these scars, its effectiveness in local populations remains unclear.
Methods and Methodology
The study was conducted from January 2015 to December 2019 in the Plastic Surgery Department at a tertiary care hospital in Karachi, Pakistan. Twenty-five patients who were treated at the hospital were recruited, while 17 out of 25 fulfilling the inclusion criteria were selected. Patients were treated according to a defined treatment protocol and evaluated after a 2-year follow-up. A survey questionnaire was administered after obtaining consent from the patients via telephonic interviews at a 2-year follow-up.
Result
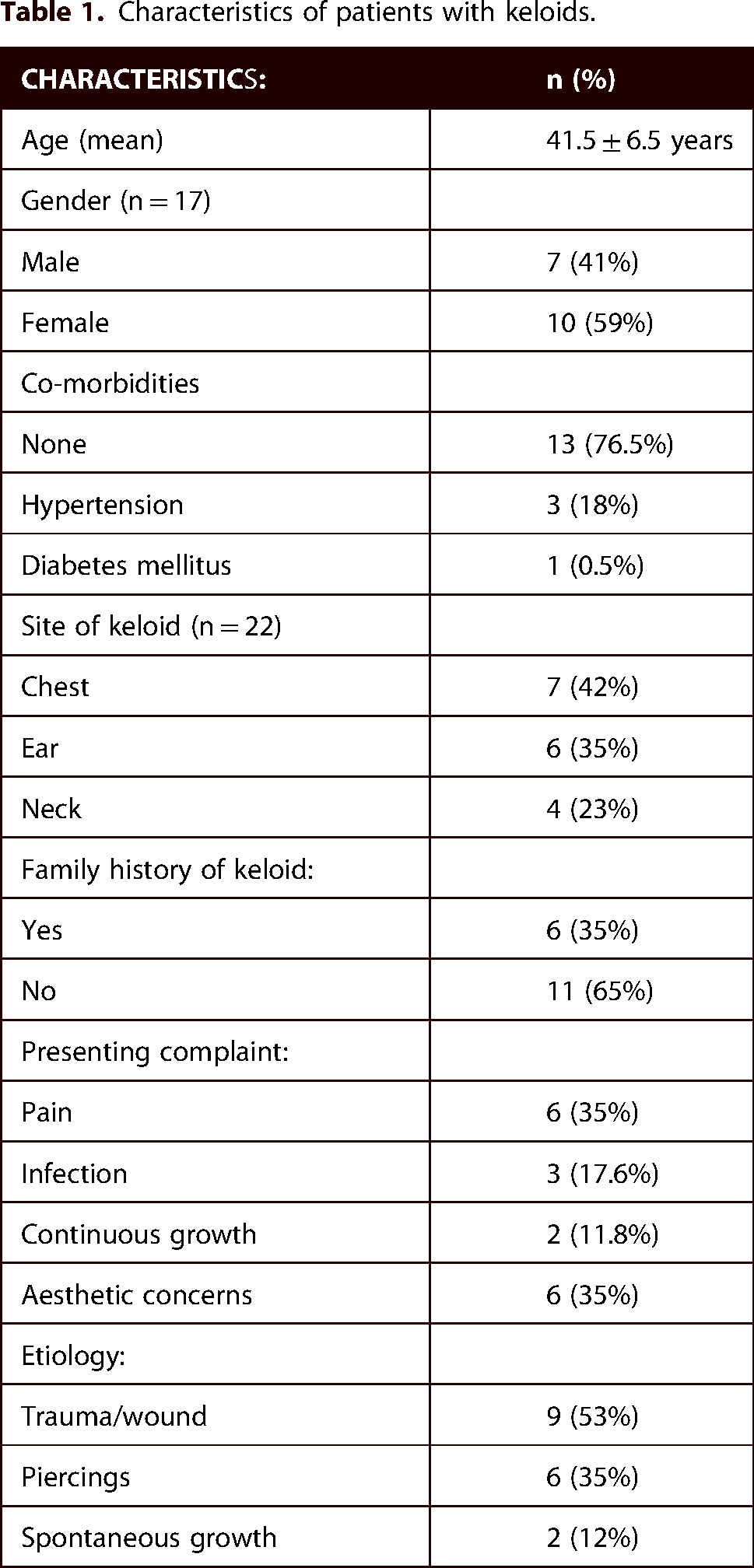
Out of 25 patients, 17 (68%) met eligibility criteria, eight (32%) were excluded due to lack of follow-up. The patients that presented with keloids, were seven (41%) males and 10 (59%) females. Six (35%) had a family history of keloids. Etiological factors included injury/trauma (n=9, 53%), spontaneous growth (n=6, 35%), and wound site growth (n=2, 12%). Recurrence post-surgery and radiation therapy occurred in 11 (65%) cases, while seven (35%) remained recurrence-free over 24 months. Recurrence frequency was noted in six (55%) patients within six months, three (27%) within 12 months, and two (18%) within 24 months.
Conclusion
Keloid management is a complex field requiring ongoing research to optimize treatment strategies, reduce recurrence rates, and improve patient outcomes through evidence-based protocols in the Pakistani population.
Lay summary
In a recent study conducted at a tertiary care hospital in Karachi, Pakistan researchers investigated the frequency of keloid recurrence following surgical removal and radiation therapy over a period of two years.
Keloids are a type of raised scar that can form after an injury or surgery, often causing discomfort and aesthetic concerns for patients.
The study aimed to understand how often keloids come back after treatment, particularly when surgery and radiation therapy are combined. This approach is commonly used to manage keloids, but its effectiveness in preventing recurrence over the long term is not fully understood.
Over the two-year follow-up period, the researchers tracked a group of patients who had undergone surgical excision (removal) of their keloids followed by radiation therapy. They observed how many of these patients experienced the return of keloids at the site of the original scar.
By analyzing the data, the researchers were able to determine the frequency of keloid recurrence in this specific group of patients. This information is important for healthcare providers and patients considering treatment options for keloids, as it helps to better understand the potential outcomes and risks associated with surgical excision and radiation therapy.
Overall, the study provides valuable insights into the management of keloids and contributes to our understanding of the long-term effectiveness of combined surgical and radiation therapy in reducing the recurrence of these troublesome scars.
Introduction
Keloids, a consequence of proliferative scar formation, are benign growths that develop at the site of skin injury or trauma. Abnormal proliferation of fibroblasts and collagen fibers 1 occurs after skin injury, resulting in raised, firm, and often painful scars that extend beyond the boundaries of the original wound. Keloids can cause significant cosmetic disfigurement, pain and functional impairment, leading to distress in affected individuals. While the exact pathogenesis of keloids remains unknown, several factors have been implicated, including genetic predisposition, mechanical stress, and inflammation. 1
Various treatment modalities have been described in medical literature for the management of keloids. This includes pressure therapy, silicone gel sheets, surgical excision, intra-lesional steroid injections, carbon dioxide laser ablation, cryotherapy and radiation therapy. 2 Most of these modalities alone have variable, often suboptimal results. Surgical excision has been a popular approach due to complete removal of keloid tissue, but the recurrence rate following surgery alone is reported to be between 50–80%. 3 Hence, adjuvant therapies like radiation have been combined with surgery to improve treatment outcomes with results showing a decrease in recurrence rate with overall recurrence rate of 29.3% using 15 Gy 3fractionated radiation for three consecutive days. 3
There is a large geographical variation in the incidence of keloids 4 with a genetic component as a proposed reason for this variation and limited data in our population. Recent studies conducted amongst various populations have examined the incidence of keloid recurrence after surgical excision and radiotherapy. For instance, according to a research study by Shih et al., 4 patients who had this combination treatment had a 32% recurrence rate. 5 Studies have also shown this to be a safe and effective method with minimal side effects 4 with no second malignancy or no associated severe or life threatening complications reported. 6
Surgical excision followed by radiation therapy has shown promise in controlling keloid recurrence but its efficacy in our population is unknown. Given the challenges associated with managing keloids and the lack of a universally effective treatment approach, this study aims to evaluate the effectiveness of this combined treatment approach in our population and contribute to the development of more effective management options for keloids. We have included a two-year follow-up in our design for the assessment of keloid recurrence. This is due to the high likelihood of keloid recurrence during the initial two-year period following treatment 7 to allow adequate time for the development of the keloid. Thus, combining surgery with radiation therapy is found to be beneficial, but efficacy in local populations is unknown. This study was conducted to evaluate the frequency of keloid recurrence with combined treatment approach of surgical excision followed by radiation therapy on a two-year follow-up in our population.
Materials and methods
Study design and settings
This cross-sectional study was conducted in the plastic surgery department of a tertiary care hospital, in Karachi, Pakistan with a retrospective approach from January 2015 – December 2019. The study was reviewed and approved by the Departmental Review Committee and Ethical Review Committee of the Aga Khan University Hospita, Karachi, Pakistan.
Recurrence was defined as a “Scar on previous surgical incision that grows beyond the margins of initial scar at least at the following time intervals of 6 months/12 months/24 months, presenting with complaints of pain and/or infection.”
Retrospective data of all adult patients (>18 years old) with keloid/s presenting to the Outpatient Department during the study period was collected, provided that they gave verbal consent for participation and met the inclusion criteria. If deemed eligible, patients were contacted telephonically regarding the study and then requested for verbal consent for participation. Upon consent, they completed the survey questionnaire (Online Appendix 1).
By using medical records of all patients with keloid coding from the Health Management Information System, patients presenting with a history of not receiving primary treatment of keloids were treated with surgical excision followed by radiation therapy for keloid > 2 years ago were selected . However, in addition, patients were excluded who had recurrent keloids at initial presentation at the clinic and prior treatment for the scar, so as to create a more homogeneous study population and to evaluate the efficacy of post-operative radiotherapy regimen on primary keloids, to minimize confounding factors that might arise from previous treatments and varying treatment histories.
Study data analyses were done using SPSS software version 25.0. Descriptive quantitative variables were reported as mean and SD / median IQR. Frequencies/Percentages were reported for qualitative variables.
Treatment protocol
All participants were treated on a pre-defined protocol.
Results
Of the 25 patients treated, complete data including follow-up were only available for 17. Analysis was performed on these 17 patients.
Table 1 shows the demographics features and characteristics of patients included in the study.

Treatment protocol for the study.

Rate of recurrence, time interval of recurrence.

Keloid neck (no recurrence).

Keloid neck (recurrence).
Characteristics of patients with keloids.
The recurrence of keloid post primary surgical excision followed by radiation therapy was observed in 11 (65%) patients, while six (35%) patients had no recurrence over the time period of 24 months. Table 2 shows the demographic features and characteristics of patients with keloid recurrence.
Characteristics of patients with keloid recurrence.

Discussion
Keloid management presents a significant challenge in dermatology and surgery due to high recurrence rates and the mixed success rates of different treatments. Our study evaluated the effectiveness of radiation therapy after surgical excision in a group of Pakistani patients and compared the findings with existing literature.
In this study, we followed up with 17 out of 25 patients, with a recurrence rate of 65%; 11 patients experienced keloid recurrence, while six remained recurrence-free over a 24-month period. This rate is considerably higher than the 27% reported by Bennett et al. 6 and the 32.7% reported by Ogawa et al. 8 in patients who received surgical excision followed by radiation therapy. The higher recurrence rate in our study could be attributed to differences in patient demographics, keloid characteristics (e.g., size and tension-prone locations), or radiation therapy protocols. Gender did not significantly impact the recurrence rate in our study, which aligns with the findings of Nangole et al., who stated that fibroblast and inflammatory factors play a greater role in keloid formation than gender. 1 Similarly, our study supports Marneros, who highlighted the role of genetic predisposition in keloid formation and treatment response, particularly in the absence of a familial history of keloids. 3
Interestingly, our findings showed that co-morbidities, such as diabetes or hypertension, did not correlate with lower recurrence rates. This is consistent with Carr et al., who suggested that other factors might play a more crucial role in keloid recurrence. 4 Several factors could explain the higher recurrence rate in our study, including differences in patient demographics, keloid characteristics (e.g., size, tension-prone areas, and location), and radiation therapy protocols.5,6 For instance, Bennett et al. 6 reported a 27% recurrence rate in 69 patients treated with surgical excision followed by radiation therapy. 7 This shows that even combined treatments cannot guarantee complete prevention of recurrence, emphasizing the need for long-term monitoring. 9
Our findings also differ from those of Hu et al., who reported a 6.7% recurrence rate using a combination of surgical resection, tension-reducing sutures, and superficial radiation therapy. 10 The significantly lower recurrence rate in their study highlights the importance of prompt radiation therapy, although differences in treatment regimens must be considered when comparing outcomes.2,11 In contrast, Aljodah et al. found that surgical excision combined with perioperative corticosteroid injections for auricular keloids resulted in a lower recurrence rate of 9.6%.12 This suggests that corticosteroid injections could be a viable alternative to radiation therapy in settings where radiation facilities are unavailable, particularly for specific keloid locations like the auricle.
The lack of data on keloid size and its potential influence on recurrence due to increased tension warrants further investigation. This aligns with Hultman et al., who indicated that while anatomical location is a key factor, tension in high-risk areas could significantly affect outcomes. 13 Future studies should prioritize data collection on these parameters to better understand their roles in keloid management.
The inclusion of additional studies in this discussion provides a broader perspective on keloid treatment. In a study, it was observed that the adjuvant treatments after keloid excision, emphasizing the lack of consensus on the best adjuvant therapy. 14 It is noted that almost 100% of keloids recur without adjuvant therapy and highlighted the potential of treatments such as intralesional triamcinolone, radiotherapy, silicone gel, and pressure therapy in reducing recurrence rates. However, they stressed the importance of minimizing dosages to avoid adverse effects, which aligns with the need for personalized treatment plans.14,15
An innovative approach by Ma et al. combined fractional CO2 laser therapy with electron beam irradiation, reporting a 12.1% recurrence rate over 18 months and high patient satisfaction, suggesting that this combination could offer an effective treatment for keloids. 15 Meanwhile, Chen et al. proposed using a tension offloading device post-surgical excision, which reduced recurrence rates to 7.9%. 10 This method could serve as an alternative to radiation therapy, especially for patients unsuitable for radiation. 16 Additionally, although high-tension areas are often associated with keloid recurrence, our data revealed a diverse distribution of recurrence sites, supporting the view of Hultman et al., who indicated that anatomical location alone is not always a determining factor for recurrence. 13
The significance of keloid etiology in treatment outcomes was also evident in our study, mirroring Ogawa et al.’s observation that different keloid types may require tailored approaches for optimal results. 8 Similar to Ogawa et al., the most common site of recurrence in our patients was the chest. The discrepancy in recurrence rates between our study and others highlights the complexity of keloid management and underscores the need for long-term follow-up. Previous research, such as Yang and Jeong, supports the idea that recurrence can manifest later, reinforcing the importance of extended monitoring. 17 This prolonged follow-up in our study may provide a more accurate assessment of recurrence.
The diverse outcomes from these studies demonstrate the complexity of keloid treatment, where factors such as the treatment method, keloid size, location, and timing play critical roles. Although surgical excision followed by radiation therapy generally yields lower recurrence rates than surgery alone, the best approach may vary depending on individual patient characteristics and keloid properties. Our study highlights the need for a multi-modal treatment strategy, considering these factors for optimal management.
Conclusion
Our study highlights the challenges of keloid management, including high recurrence rates despite combined treatments. Factors like size, location, and tension-prone areas may influence outcomes but remain underexplored, emphasizing the need for standardized data collection. Future protocols should prioritize personalized approaches, incorporating strategies like tension-reducing sutures, fractional CO2 laser therapy with electron beam irradiation, or corticosteroid injections as radiation alternatives in resource-limited settings. These efforts can enhance treatment efficacy and advance keloid management.
Limitations
Our study's limitations include its retrospective design, which may introduce selection bias and limit the control of confounding variables, and the reliance on telephone follow-ups, which could lead to reporting bias. Follow-up was conducted via telephone, which may have introduced inaccuracies in patient-reported recurrence, emphasizing the need for in-person assessments or imaging in future studies. Additionally, over 30% of our patients were lost to follow-up, which may have influenced the study's findings. While we performed all analyses on the available data from 17 patients, the absence of follow-up data for the remaining patients could have impacted the overall outcomes. Future studies with more complete follow-up data are necessary to confirm these findings and reduce the potential for missing data to affect the result. Furthermore, the inconsistent recording of keloid sizes across patient medical records prevented a comprehensive analysis of the impact of keloid size on recurrence rates. Future studies should ensure consistent and thorough documentation of keloid characteristics to enable more detailed analyses.
Clinical implications
The study provided valuable insights into the epidemiology of surgical excision followed by radiation therapy for keloid recurrence in Pakistani population on a 2-year follow-up. Our findings indicate that the current regimen of surgery and radiotherapy has led to an unacceptably high recurrence rate, necessitating a thorough reevaluation before it can be recommended as routine treatment in our unit. We emphasize the urgent need for modifications to enhance patient outcomes.
Strength of the study
The study is first of its kind from Pakistani population, even with the limitations it provides valuable insights into the recurrence rate and frequency of keloid in Pakistani population, success or failure rate of surgical excision followed by radiation therapy treatment modality for the population among other treatment modality being practiced by the clinicians.
Supplemental Material
sj-docx-1-sbh-10.1177_20595131251321766 - Supplemental material for Frequency of keloid recurrence post-surgical excision and radiation therapy on a 2-year follow-up: A single center cohort study
Supplemental material, sj-docx-1-sbh-10.1177_20595131251321766 for Frequency of keloid recurrence post-surgical excision and radiation therapy on a 2-year follow-up: A single center cohort study by Ceemal Khan, Nida Zahid, Fizzah Arif, Asim Hafiz, Omair Shaikh and Mohammad Fazlur Rahman in Scars, Burns & Healing
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.