
Abstract
Background:
The pathophysiology of keloid scars is still not fully understood and a universally reliable effective treatment has not been identified. Pharmacogenetics explores how drug response to a particular therapy can relate to genetic variations.
Purpose:
To investigate how pharmacogenetics could be applied to keloid scars and the relevance of this to clinical practice.
Methods:
We reviewed the literature and discuss our current knowledge of pharmacogenomics in the treatment of keloid scars. A literature search was performed using the terms ‘Pharmacogenetics’, ‘Pharmacogenomics’, ‘Keloid’ and ‘Scar’. We searched the PubMed, MEDLINE and EMBASE databases to find the relevant articles. Only articles in English were chosen. The level of evidence was evaluated and selected accordingly listing the studies with the highest level of evidence first.
Results:
Treatments including corticosteroid injections and 5-fluorouracil can be effective in some patients, but less so in others. Polymorphisms of the glucocorticoid receptor and variants of CCL2, YAP1, miR-21-5p and NF-κβ might be responsible for different responses to treatments used in keloid scars such as 5-fluorouracil. Small molecule inhibitors might be utilised to target other implicated genes.
Conclusion:
Pharmacogenetics aims to produce the most efficacious patient outcomes while reducing adverse effects. Understanding the pharmacogenetics of keloid scars could lead to a new era of personalised medicine in the treatment of keloid scars. At present, there is some evidence (level 3b/4) to suggest genetic variations that are responsible to drug response in keloids, but further research in this field is required.
Lay summary
The varied response to similar therapeutic treatments in keloids has prompted the consideration of the role of genetic variants on response in the form of pharmacogenetics. Pharmacogenetics refers to drugs and their metabolism and action based on genetic influences. The ideal scenario would involve the selection of treatment based on the individual’s specific genetic variants to ensure maximum efficacy with minimal toxicity. Some evidence currently points to genetic variations in some keloid patients that might be of relevance to the treating clinician.
Introduction
Pharmacogenetics is the discipline that explores whether a genetic variation can predict drug therapy response.1,2 This has been applied in aspects of medicine including targeted treatments in oncology. 3 It has also been used for predictive assessment of those at risk of adverse drug reactions, such as thiopurine methyltransferase (TPMT) deficiency—secondary to TPMT gene defect—predisposing to agranulocytosis in thiopurine drugs. 4
Keloid scars are fibro-proliferative lesions manifesting as disfiguring, protuberant scars extending beyond the bounds of the original trauma. 5 Typical sites include the earlobes, shoulders and sternum. While there is a recognition that certain ethnic groups are predisposed to keloid scars (higher Fitzpatrick skin types), the precise pathophysiology has not been fully elucidated. Genome-wide association studies (GWAS) have allowed for identification of several genetic loci in families of different ethnicities such as African Americans who are susceptible to developing keloid scars. 6 Substantial evidence implicates mechanobiological factors such as pressure and tension in the pathogenesis and sustainment of keloids. These factors exert changes at intracellular and extracellular levels with signalling pathways involved in scar formation and fibrosis. Histological analysis has also shown increased angiogenesis and inflammation at sites of high tension such as the keloid edges. 7
A broad range of therapies are used for patients with keloid scars, none of which are universally successful. Non-invasive treatments tend to suppress fibroblast proliferation rate and genesis of extracellular matrix and collagen. 5 They also induce apoptosis and suppress inflammation and upregulate matrix metalloproteinase to prevent keloid scar formation. 5 Non-invasive therapies include pressure garment therapy, silicon gel sheeting, onion extract and heparin gel, intralesional corticosteroid and 5-fluorouracil (5-FU) injections, bleomycin and mitomycin C. 5 Corticosteroid therapy remains the mainstay of treatment. 8
Surgical excision can be used with a reduction in relapse rates achieved when combined with adjunctive steroid treatment. 9 Combination of surgery followed by radiation and corticosteroid tape was found to be most efficacious for maintaining long-term disease control and suppression of regrowth. 10
Lasers have shown to play a role in the management of keloids, albeit limited, and are most effective in combination with corticosteroids. 11
More recently, pharmacogenetic studies have investigated differing treatment response among patients. There is a paucity of literature investigating pharmacogenetics of keloid scars and how treatment response can be influenced by pharmacogenetics. Our review addresses these apparent gaps in the literature and supports the need for personalised medicine in the treatment of keloid scars. The aim of the present study was to review the pharmacogenetics and investigate how personalised and targeted medications could be used for improved clinical outcomes in keloid scars.
Methods
Using the keywords ‘Pharmacogenetics’, ‘Pharmacogenomics’, ‘Keloid’ and ‘Scar’, we searched the PubMed, MEDLINE and EMBASE databases to find the relevant literature in English language articles only. Our review was conducted in June 2020 and the time period of evidence was collected from the inception of these databases till 16 June 2020.The level of evidence was evaluated and selected according to the highest level and working our way downwards. Using the Oxford Centre of Evidence-Based Medicine 2011 guidance, we analysed and listed the evidence based on its strength from level 1 to level 5 with systematic reviews and meta-analyses considered first, randomised controlled trials second, cascading down to weaker evidence such as case reports.
Pharmacogenetics and keloids
Pharmacogenetics is used in reference to genes and their relation to drug metabolism, 12 whereas pharmacogenomics refers to all genes in the genome that may determine the drug response. 13 Pharmacogenetics explores single genes and their effect on the action of drugs, while pharmacogenomics studies many genes and their patterns alone and in combination. Pharmacogenomics therefore acknowledges that the response to a drug may be multifactorial. 12
GWAS are used to discover whether single nucleotide polymorphisms (SNP) may be associated with a particular phenotype such as the response to a particular medication. 14
In addition to the DNA coding section for proteins (genes), increasing evidence highlights the role of non-coding sections of DNA playing a role or be associated with a particular phenotype. Epigenetics involves heritable DNA gene function and expression changes without modifying the gene DNA sequence. Epigenetic mechanisms reported include histone and covalent DNA modification and regulation of non-coding RNA and DNA methylation 15 with different gene expression altering patterns of DNA methylation and histone modification. 16 This process of epigenetics affects not only cell phenotypes, but also the heterogeneity in drug response. Newer drugs have been designed to regulate epigenetic processes in disease states, further developing the notion of personalised medicine. 17
Identifying patients likely to respond to treatments
Some keloid scars appear sporadic, but others are likely to represent a familial genetic disease in which multiple genetic mutations each confer varying degrees of predisposition to keloid scar development. 18 Mendelian inheritance is described in keloid-associated syndromes such as Rubinstein-Taybi, Goeminne syndrome, lateral meningocele, Leigh necrotising encephalomyelopathy, Ullrich congenital muscular dystrophy and Ehlers-Danlos syndrome. These all have a dominant inheritance pattern in common.18,19
Linkage and GWAS studies have found associations on chromosomes 2q23 and 7p11 in Japanese and African American families, respectively (Table 1). 18 Two possible susceptibility loci found in a Chinese Han family were 18q21.1 and 10q23.31. 20 In a GWAS involving Japanese patients, three susceptibility loci were found. These were 1q41, 3q22.3-23 and 15q21.3. 21
Implicated chromosomes and variants for keloid susceptibility and 5-FU response.

5-FU, 5-fluorouracil.
The role of pharmacogenetics and the varied response to treatments has been studied with 5-FU and glucocorticoids in the treatment of keloids.
Results
The results of this review are summarised in Table 2.
Results of pharmacogenetic studies.
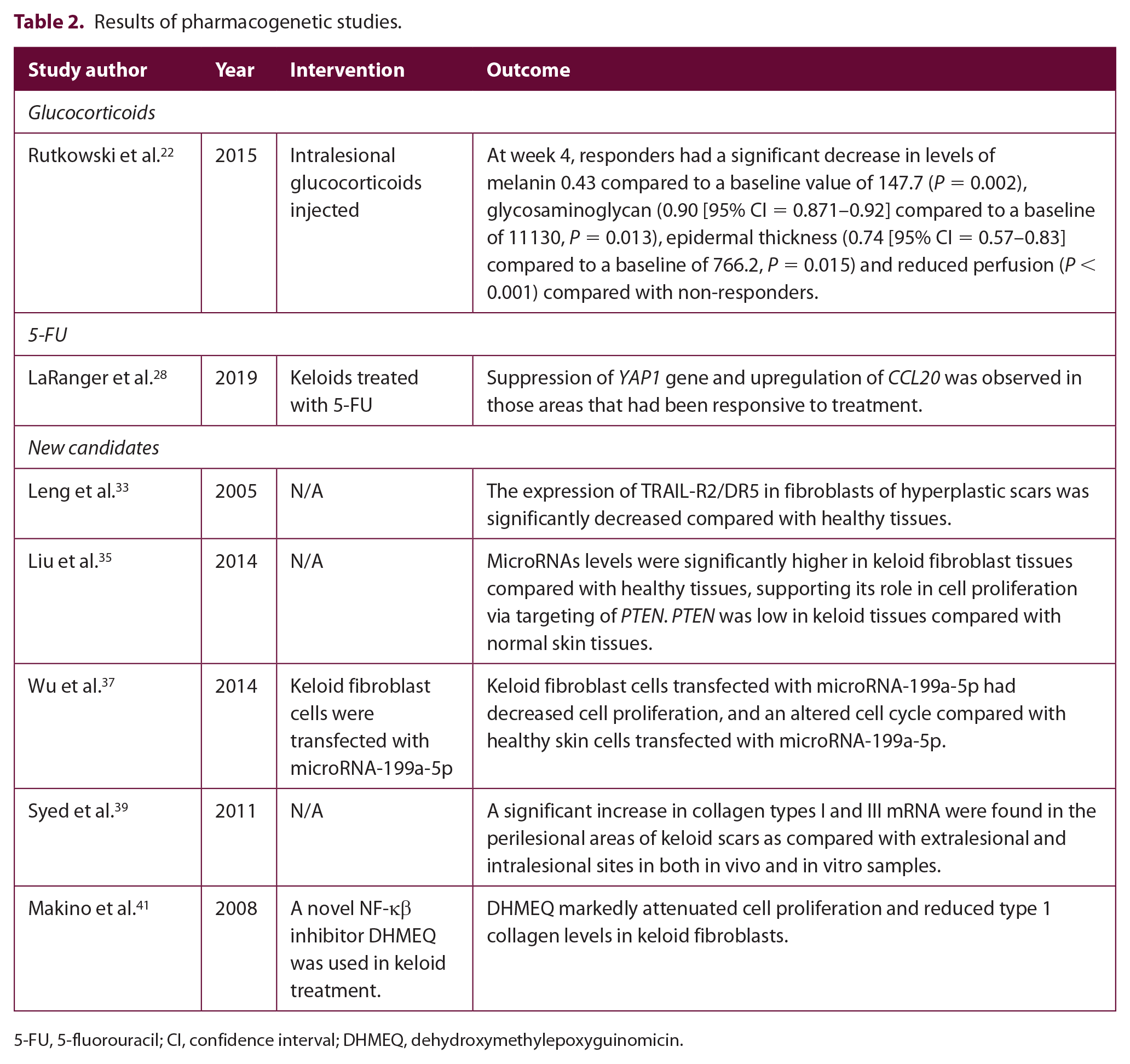
5-FU, 5-fluorouracil; CI, confidence interval; DHMEQ, dehydroxymethylepoxyguinomicin.
Corticosteroids
Glucocorticoids are most commonly used as first-line treatment for keloid scars with variable responses and relapse rates. In a study involving 19 patients (later categorised as 12 steroid-responsive and seven steroid-non-responsive), intralesional glucocorticoids were injected in keloids and their response monitored over four weeks. 22 Response was quantified using full-field laser perfusion imaging, spectrophotometric intracutaneous analysis of collagen and melanin, immunohistochemical studies, in addition to clinical response. Histological methods assessed alterations in epidermal thickness and glycosaminoglycan expression. Reverse transcriptase polymerase chain reactions (PCR), immunoblotting and immunohistochemistry were used to examine changes in expression of the glucocorticoid receptor in keloid tissues. 22
At week 4, responders had a significant decrease in levels of melanin (0.43 [range = 0.32–0.50] compared to a baseline value of 147.7 measured with spectrophotometric intracutaneous analysis SIAscopy, P = 0.002), glycosaminoglycan (0.90 [range = 0.871–0.92] compared to a baseline of 11130, P = 0.013), epidermal thickness (0.74 = 0.57–0.83] compared to a baseline of 766.2, P = 0.015) and reduced perfusion (P < 0.001) compared with non-responders. The decreased melanin content observed in some dark-skinned individuals after glucocorticoid treatment might relate to mechanisms of pharmacoge-netics. The authors speculate that darker-skinned individuals experience glucocorticoid inhibition of melanogenesis through apprehension of the melanocyte cell cycle. 22 This is consistent with the fact that darker-skinned individuals exhibit greater hypopigmentation in response to steroid treatment,23,24 possibly, related to the size gradient of melanosomes with the largest found melanosomes in keratinocytes found in dark skin, followed by Asian and then Caucasian skin. 24 It is still unclear whether the level of hypopigmentation relates to the effects of corticosteroids or a combination of this and the above mentioned effects.
Glucocorticoid receptor (GR; encoded by gene NR3C1) expression in steroid responders was significantly greater than non-responders at baseline. In steroid-responders, GR expression decreased, as measured by mRNA and protein expression (gauged by reverse transcriptase-PCR and western blotting) after glucocorticoid treatment. It is thought that glucocorticoids are responsible for the downregulation of GR in cells and tissue. 25 Keloid responsiveness to glucocorticoids is thought to therefore be related to baseline glucocorticoid receptor levels and downregulation of these glucocorticoid receptors. 22
An alternative isoform of GR, GR-β, inhibits GR-facilitated expression. 26 GR-β could be responsible for reduced GR expression in non-responders and the absence of GR downregulation after glucocorticoid treatment. 27
5-Fluorouracil
The gene expression of keloid scars treated with 5-FU was analysed in a study by LaRanger et al. 28 The microarray results from treated and untreated areas of keloid scars were investigated. Using Random Forest analysis, distinct expression profiles were found in the treated and untreated areas. Random Forest analysis is a type of machine-learning algorithm that can carry out thousands of rounds of gene analysis on global gene expression arrays to increase statistical power. Using this method enabled thousands of gene analytics to be produced to create an extrapolative gene expression profile with fewer false positives. This was visualised through multidimensional analysis and a selection of genes most likely to influence keloid treatment was suggested. In keloids treated with 5-FU, suppression of YAP1 gene and upregulation of CCL20 was observed in those areas that had been responsive to treatment. 28 YAP1 gene is thought to have pro-fibrotic capabilities involved in the positive feedback loop that augments and maintains fibrosis. 29 CCL-2 is a regulator of T cell activity downstream of TGF-ß.
No changes in genes previously associated with keloids were found in the study by LaRanger et al. 28 For example, no changes in the genes coding for TGF-β, PDGF, MMPs, IL-1, IL-6 and IL-10 were found. These proinflammatory cytokines have previously been associated with fibroinflammatory disease.30,31 In addition, gene networks were disrupted, such as the IL-17A pathway. 28
New candidates
The formation of keloid scars could be related to the imbalance of fibroblast apoptosis of scar tissue and tumour necrosis factor related apoptosis inducing ligand (TRAIL) of fibroblasts. 32 TRAIL is thought to bind to its receptor, acting as an intermediary in fibroblast apoptosis. 32 The investigation of TRAIL and TRAIL-R2/death receptor 5 (DR5) for treating keloids has been reviewed. 32 The expression of TRAIL-R2/DR5 in fibroblasts of hyperplastic scars has been found to be significantly decreased compared with healthy tissues leading to the lack of apoptosis and uncontrolled fibroblast activation. 33
MicroRNAs are non-coding RNAs that play a role in the regulation of gene expression. 34 MicroRNAs levels were significantly higher in keloid fibroblast tissues compared with healthy tissues, possibly supporting its role in cell proliferation via targeting of phosphatase and tensin homolog deleted on chromosome 10 (PTEN). 35 PTEN has been found to inhibit cell proliferation, survival and growth 36 and was low in keloid tissues compared with normal skin tissues. 35 The present study highlighted the possible associations between microRNA-21 expression, keloid fibroblast apoptosis and cell proliferation.
Conversely, other microarray analysis studies utilising PCR methods found decreased microRNA-199a-5p expression in keloid tissues compared with normal tissue. Keloid fibroblast cells which were transfected with this particular microRNA-199a-5p had decreased cell proliferation and an altered cell cycle (longer S and G2/M stages) 37 compared with healthy skin cells transfected with microRNA-199a-5p. The latter, therefore, might play a fundamental part in inhibiting keloid fibroblast proliferation. 38
A significant increase in collagen types I and III mRNA were found in the perilesional areas of keloid scars as compared with extralesional and intralesional sites in both in vivo and in vitro samples. 39 This suggests that keloid fibroblasts may have heterogeneous activity levels in vitro and in different parts of the keloid. The present study suggests heterogeneity of cellular function and by implication heterogeneity of response to therapy. 30
The NF-κβ pathway has been implicated in the keloid fibroblasts activation. 40 Proinflammatory cytokines such as interleukin-1 and tumour necrosis factor-α are activated by NF-κβ in a positive feedback mechanism. A novel NF-κβ inhibitor dehydroxymethylepoxyquinomicin (DHMEQ) was trialled in keloid treatment. 41 Baseline NF-κβ was inherently raised in keloid fibroblast cells, supporting the concept that the NF-κβ pathway is fundamental for keloid pathogenesis. DHMEQ markedly attenuated cell proliferation and reduced type 1 collagen levels in keloid fibroblasts. Therefore, patients who have NF-κβ elevations could benefit from such therapy. 41
Discussion
Responsiveness to glucocorticoids in keloid patients is likely to be related to the baseline GR level and possibly a lack of GR-β isoform. Screening for the presence of GR and related isoforms could, perhaps, prevent ineffective glucocorticoid treatment and the numerous adverse effects associated with repeated futile treatments in patients who do not appear to respond to initial corticosteroid treatment. 22
In terms of 5-FU, our findings suggest that YAP1 gene and CCL2 genes are candidates for further analysis and studies investigating whether their possession and activity confers greater likelihood of response of keloids to 5-FU are warranted.28,29 CCL2 has also been implicated in multiple sclerosis. 31 Patients with multiple sclerosis treated with methylprednisolone after a relapse were found to have a significant decrease in CCL2 serum levels after five days of treatment with a decrease from 268.35 ± 132.7 to 129.8 ± 50.95 in the serum levels of CCL2 (P = 0.045) (values compared with CCL2 standards). Clinical improvement in patients with multiple sclerosis treated with methylprednisolone after a relapse could be associated with immediate decrease in CCL2 levels. 31
For new treatment candidates, the use of DR5 agonists (such as conatumumab, drozitumab, lexatumumab and tigatuzumab) has been suggested in order to upregulate TRAIL-R2/DR5 and reduce the formation of keloid scars through initiation of apoptosis. 32 This requires further investigation and the risk of hepatotoxicity associated with these medications cannot be overlooked. 42
Further studies are required to elucidate the exact mechanism of microRNA-199a-5p in keloid pathogenesis. Recently, miR-21-5p inhibitors were shown to reduce keloid fibroblast auto-phagocytosis. This was associated with a decrease in expression of miR-21-5p and an increase in expression of apoptosis-associated genes. These laboratory findings have not yet been translated into clinical practice. Nevertheless, they suggest that miR-21-5p might be a useful therapeutic target to reduce keloid recurrence. 39
The strengths of this review include the wide search parameters employed and the depth of literature investigated implicating several gene loci associated with pharmacogenetics in keloid scars. This review is limited by the small number of clinical studies investigating this field of research as well as the lack of inclusion of non-English language articles. Future research will hopefully expand reviews such as this one, enabling better understanding of an interesting and important field of dermatology.
In the present article, we have recommended screening patients with keloids for certain genetic loci. This could revolutionise treatment for patients but is likely to be impractical and unfeasible for current clinical practice in healthcare systems evaluating cost-effectiveness. In the future, we envisage keloid management to be handled with a personalised approach. Increasing understanding of the pharmacogenetics of keloid scars will hopefully lay the foundations for future treatment in which keloid treatment is managed. Targeted therapies of particular gene loci in susceptible individuals could improve patient outcomes and their quality of life.
Conclusion
Keloid scars are likely to represent complex genetic diseases with a number of genes each imparting susceptibility to keloid scars. Initial studies have suggested that screening for polymorphisms of the glucocorticoid receptor may indicate responsiveness to corticosteroids and variants of CCL2, YAP1, miR-21-5p and NF-κβ may indicate response to 5-FU. There are additional genes that could be targeted with small molecule inhibitors. Identifying these loci and further investigation of pharmacogenetics could allow for targeted and personalised treatments of keloid scars. 43
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.