
Abstract
Keloids are pathological scars that grow over time and extend beyond the initial site of injury after impaired wound healing. These scars frequently recur and rarely regress. They are aesthetically disfiguring, can cause pain, itching, discomfort as well as psychological stress, often affecting quality of life. Many treatment modalities, including surgical and non-surgical, have been explored and have been reported to be beneficial; however, none have been absolutely satisfactory or optimal for the treatment of all keloid subtypes to date. This poses a major challenge to clinicians. Often, a combinational therapeutic approach appears to offer the best results with higher patient satisfaction compared to monotherapy. The aetiopathogenesis of keloids is not fully elucidated; however, with recent advances in molecular biology and genetics, insight is being gained on the complex process of scar formation and hence new therapeutic and management options for keloids. In this paper, we explore the literature and summarise the general concepts surrounding keloid development and review both current (corticosteroids, surgical excision, silicone-based products, pressure therapy, radiotherapy, cryotherapy, laser therapy, imiquimod and 5-fluorouracil) and emerging (stem cell therapy, mitomycin C, verapamil, interferons, bleomycin, botulinum toxin type A and angiotensin-converting enzyme inhibitors) treatments. Increased knowledge and understanding in this area may potentially lead to the discovery and development of novel therapeutic options that are more efficacious for all keloid types.
Lay Summary

Keloids are problematic scars that are difficult to treat and manage. The aetiopathogenesis of keloids is not clear; however, recent advances in molecular biology and genetics are beginning to shed light on the underlying mechanisms implicated in keloid scar formation which will hopefully lead to the development of treatment options for all keloid types. This review summarises current and emerging therapies.
Introduction
Wound healing is an intricate and complex series of processes comprising overlapping phases of inflammation, granulation tissue formation and tissue remodelling, and results in tissue structure integrity and damage being restored. 1 Abnormal wound healing can give rise to keloids, which are benign dermal fibroproliferative nodular lesions that tend to recur after excision. Keloid scars arise from skin trauma or inflammation and may develop years after the initial insult and rarely regress. 2 The scar tissue extends beyond the original wound site and can be disfiguring and cause psychosocial issues impairing quality of life. 3 In addition, patients may present with symptoms such as burning, pain, pruritus, movement limitation and hyperaesthesia. 2
Aetiology
The aetiology of keloids is still poorly understood. The most common regions of the skin for keloids include upper arms, skin overlying joints, chest, shoulders and head–neck regions, particularly the ear lobes (Figure 1). The anatomical location of a keloid appears to alter its morphological characteristics. Some keloids can develop spontaneously; however, most occur years after local trauma and other events including inflammation, surgery, burns, elective cosmesis, foreign body reactions, acne, insect bites, vaccinations or mechanical force.4,5

Earlobe keloids as a consequence of ear piercing.
Epidemiology and keloid genetics
The incidence of keloids is highest among darker-pigmented persons of African, Asian and Hispanic descent and is estimated to be in the range of 5%–16%. 3 Males and females have an equal risk of developing keloids, 6 although incidence is slightly increased in females, likely attributable to them having more cosmetic procedures like ear piercing. 7 Persons aged 10–30 years are also at a higher risk of developing keloids. Additional risk factors include having blood type A, hyper-IgE and hormonal peaks during pregnancy or puberty. 8
Familial keloid case studies and twin studies support the notion that genetic factors have an influence in keloid aetiology. 9 Although no one specific gene has been associated with the development of keloids, a number of genes and gene loci have been identified.6,10 Genome-wide association studies and admixture mapping studies have identified single-nucleotide polymorphisms across certain loci genetically linked to keloid development including the NEDD4 gene, which encodes E3 ubiquitin ligase enzyme, and the myosin genes, MY01E and MYO7A.10 –13 Studies have also reported the involvement of several human leucocyte antigen (HLA) alleles, p53, bcl-2 and fas genes.10,14 –16 Furthermore, rare genetic disorders have been reported to present with spontaneous keloids including Dubowitz syndrome, Bethlem myopathy, Rubinstein-Taybi syndrome, Noonan syndrome, Geominne syndrome and others.10,17 These lines of evidence suggest that genetic factors play a role on keloid predisposition.
Pathophysiology of keloids
Keloid pathology is complex, involving both genetic and environmental factors. Keloids form as a result of abnormal wound healing and excessive dermal fibrosis. Development of keloids has been linked to over-proliferation and reduced apoptosis of dermal fibroblasts, over-production of collagen fibres and other extracellular matrix (ECM) components as well as abnormal ECM production and remodelling. 1 Various cytokines, growth factors and proteolytic enzymes have been implicated in the formation of keloids including transforming growth factor-β (TGF-β), epidermal growth factor (EGF), vascular endothelial growth factor (VEGF), platelet-derived growth factor (PDGF), connective tissue growth factor (CTGF), tumour necrosis factor-α (TNF-α), insulin-like growth factor-1 (IGF-1), fibroblast growth factor-β (FGF-β), interleukin-6 (IL-6) and matrix metalloproteinases (MMPs).3,14,18 Furthermore, signalling pathways such as Toll-like receptor signalling, SMAD signalling and fibronectin have been reported to be associated with keloid development.18,19
Histopathology of keloids
Histologically, keloids comprise an abundance of unordered dermal collagen and vasculature with high inflammatory-cell infiltrate and over-active mesenchymal cells.14,15 In addition to collagen, elastin, fibronectin and proteoglycans are deposited in excess amounts in keloid scars. 9 Collagen creates frequent cross-links in ordinary wounds, whereas collagen is irregularly organised in keloids, forming nodules in the dermis. 20 During normal wound healing, the early wound immature collagen type III can be modified into mature collagen type I. In keloid tissue, it mostly comprises disorganised collagen types I and III, made up of pale-staining hypocellular collagen clusters, lacking nodules or surplus myofibroblasts. 21 Furthermore, recent research has provided four distinct findings only present in keloid specimens: (1) presence of keloidal hyalinised collagen; (2) presence of a tongue-like advancing edge underneath normal-appearing epidermis and papillary dermis; (3) a horizontal cellular fibrous band in the upper reticular dermis; and (4) a prominent fascia-like band. 22
Treatment of keloids
Currently, various forms of treatment for keloids exist; however, no single treatment has proven to be the most effective. This review will explore and discuss current and emerging treatment modalities (Figure 2). Some of the ongoing or completed clinical trials of keloid therapy registered on https://clinicaltrials.gov/ and accessed on 21 May 2019 are summarised in Table 1. 23 Studies with the status ‘terminated’, ‘suspended’ or ‘withdrawn’ were excluded.
Clinical trials of keloid therapy on ClinicalTrials.gov (accessed on 21 May 2019). 23 .
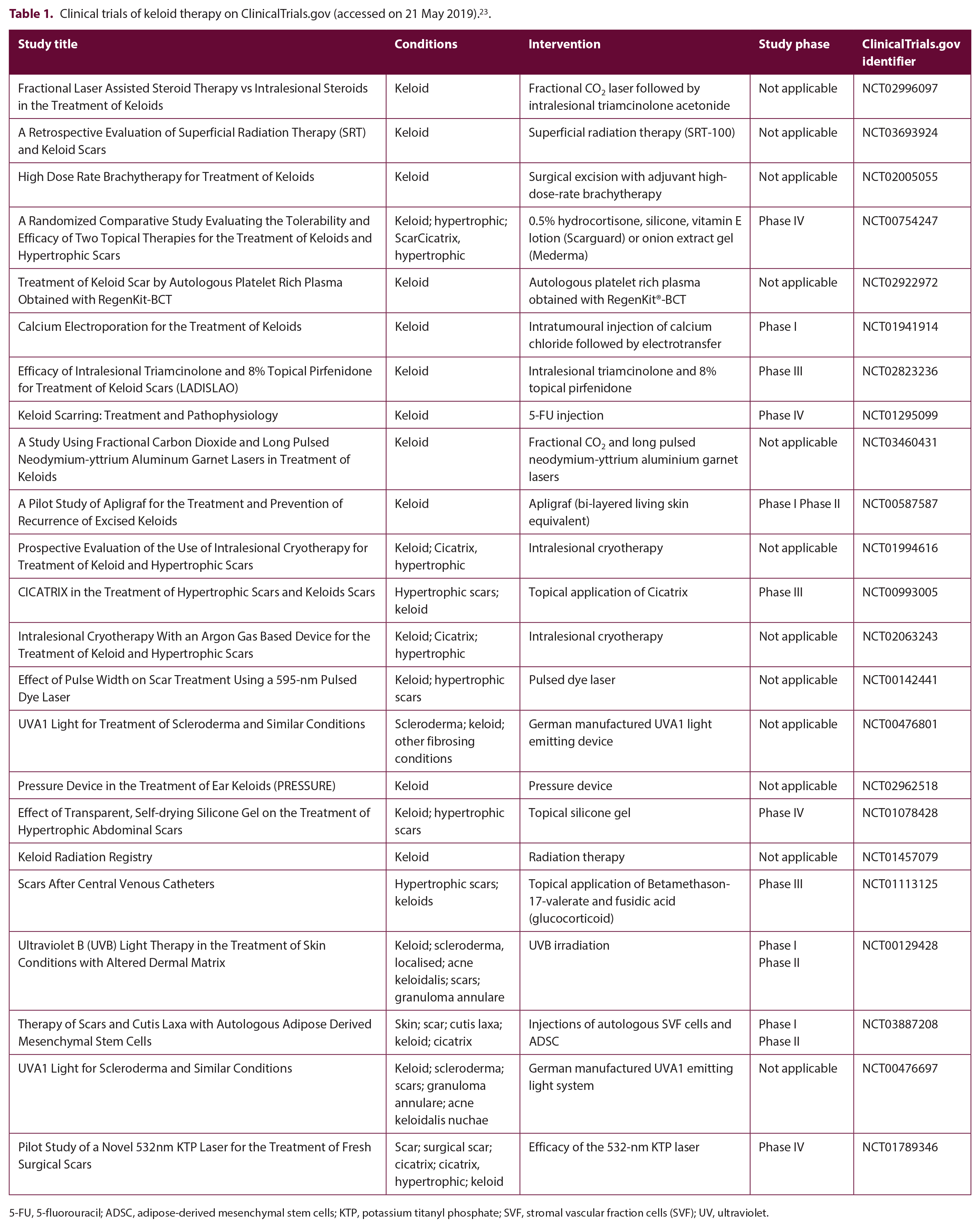
5-FU, 5-fluorouracil; ADSC, adipose-derived mesenchymal stem cells; KTP, potassium titanyl phosphate; SVF, stromal vascular fraction cells (SVF); UV, ultraviolet.

Current and emerging treatment strategies.
Current treatments
Corticosteroids
Several corticosteroids can be used for the treatment of scars including triamcinolone acetonide (TAC), hydrocortisone acetate, dexamethasone and methyl prednisolone. 24 However, since 1961, 25 TAC has been the most widely used corticosteroid for the treatment of keloids.26,27 Intralesional TAC injections have been shown to reduce scar volume and height, improve scar pliability, and diminish associated scar pain and itching 8 as well as prevent recurrence. 3 Corticosteroids have anti-inflammatory and anti-mitotic properties. 1 Several other mechanisms have been reported by which corticosteroids reduce keloid scar including inhibition of fibroblast growth, attenuation of procollagen and glycosaminoglycan synthesis, reduction of endothelial budding and enhancement of collagen and fibroblast degeneration.28,29 Corticos-teroids inhibit TGF-β1 expression and induce apoptosis in fibroblasts, inhibit VEGF and alpha-globulins, which are involved in the wound healing process.28 –31 VEGF, which promotes angiogenesis, was reported to be highly expressed in keloid fibroblasts compared to controls but exogenous addition of the glucocorticoid dexamethasone suppressed its expression in vitro. 32 Furthermore, VEGF expression was overexpressed in keloid tissue which later reduced following intralesional TAC injections in vivo. 33
TAC is typically administered at intervals of 4–6 weeks until pruritic and pain-associated symptoms diminish and the scar flattens. 34 The dose of TAC is in the range of 10–40 mg/mL, depending on the size and anatomical location of the lesion and the age of the patient. 34 TAC is used either alone as a monotherapy or in combination with other treatment modalities.1,3 The response rates to corticosteroid injections vary clinically with regression rates in the range of 50%–100% reported after one year and recurrence rates in the range of 33%–50% reported after five years. 3 Combined therapy comprising surgical excision followed by TAC treatment also varied with reported recurrence rates in the range of 8%–50%. 35 Previous clinical studies, where TAC was used alone, reported efficacy and good clinical outcome with this treatment including reduced keloid height, length, width, related pruritus and erythema, and improved pliability.36,37 A recent randomised parallel-group study that compared the role of intralesional TAC, fractional CO2 laser or intralesional verapamil in the treatment of keloid in 60 patients showed reduction in scar height, vascularity and pliability in all three groups using the Vancouver Scar Scale score; however, pigmentation was not completely resolved with any of the treatments. The response was fastest with TAC followed by verapamil and laser and this was statistically significant. 38 However, intralesional TAC in combination with other treatment modalities, such as 5-fluorouracil (5-FU), pulsed dye laser (PDL), surgery, interferon (IFN)-α-2b, verapamil and surgery, all yielded significant improvements compared to treatment with TAC monotherapy.3,39 –43
Intralesional steroid injections can cause several adverse side effects, such as telangiectasis, atrophy, steroid acne, pigmentary changes, necrosis, ulcerations and systemic side effects. 3 There is also significant pain associated with intradermal corticosteroid injections that can be reduced when local anaesthetic lidocaine is administered to control the pain. 44 Furthermore, the side effects have been reported to diminish when intralesional TAC is used in combination with 5-FU. 45
Surgical excision
Surgical excision is a traditional method of removing keloids (Figure 3). 46 However, excision creates a new wound and can result in a similar or larger keloid. 47 Therefore, surgical excision is not recommended as a monotherapy as it results in high recurrence rates in the range of 45%–100%.2,48 For better postoperative surgical outcomes, surgical excision is often combined with other forms of treatment including radiotherapy, intralesional corticosteroid injections, IFN injection, bleomycin, cryotherapy, pressure therapy and silicone gel or sheeting.8,26,49 Successful use of dermal substitutes and epidermal skin grafting with keloid excision has also been reported. 50 A recent case series study, in which 141 patients with anterior chest wall keloids were given a treatment protocol consisting of complete excision, Z-plasty, postoperative adjuvant radiotherapy and postsurgical wound self-management, reported excellent outcomes with a recurrence rate of only 10.6%. 51 The use of steroid tape and injections helped to resolve the recurrence of keloids. 51

Auricular keloid surgical excision used as monotherapy. Auricular keloid before (a) and after (b) surgical excison.
A variety of methods can be used for the surgical removal of keloids depending on the size of the keloid, anatomical location, skin type and age of patient. 52 These include linear closure and flap coverage, excision with grafting, W-plasty and Z-plasty. 53 To reduce risk of keloid recurrence, the surgeon performing the excision should establish tension-free wound closure. As a general rule, closure of the wound should be accomplished with minimal tension and sutures, leaving everted wound borders. Z-plasties, three-layered sutures, subcutaneous/fascial tensile reduction sutures or local flap surgery can be employed on a case-by-case basis.54,55 The final outcome of the scar is often positively correlated with the experience of the operating surgeon and technique utilised, as well as the patients’ active participation in their wound care. 52
Silicone-based products
Since the 1980s, silicone-based products have been used in the treatment of keloids and hypertrophic scars, with silicone gel or silicone gel sheeting considered as first-line therapy for minor keloids and hypertrophic scars.26,35 There are various other forms of silicone including creams, sprays, gel cushion and liquid. 24 The precise mechanism of action of silicone products is not fully understood but it is proposed that they enhance hydration and create an occlusive environment 53 which influences fibroblast regulation and decreases collagen synthesis. 56 Silicone gel sheeting has been shown to have minimal side effects including local irritation which can be resolved quickly. 24 Studies have shown that the beneficial effects of silicone gel sheets include pain reduction, tenderness and pruritus and flattening the keloid. 57 The silicone gel sheeting is recommended to be worn from two weeks, after primary wound treatment, for 12–24 h for 2–3 months. 58
Studies have demonstrated an improvement of up to 90% in keloid scars after using silicone gel sheeting 35 and a decrease in the incidence rates of keloids and hypertrophic scars after surgery. 59 In addition, controlled studies have reported the clinical effectiveness of silicone gel and silicone gel sheeting in the prevention and treatment of keloids.35,58 However, a recent meta-analysis review 60 and Cochrane review 61 found that even though studies published data in support of the efficacy of silicone gel sheeting in the treatment and prevention of keloid and hypertrophic scarring, they provided weak evidence and were of poor quality.60 –62 Therefore, given the lack of substantial evidence, well-designed clinical trials and studies are required to gain a better understanding of the effectiveness of silicone-based products in preventing and treating keloids.
Pressure therapy
Pressure therapy has been used to treat and manage keloids and hypertrophic scars for decades.35,63 It has been routinely employed as first-line treatment in the treatment of hypertrophic scarring resulting from burns. 64 The underlying mechanisms of action of compression techniques remain unclear; however, several hypotheses exist, some of which include increased pressure to the scar surface reduces perfusion and decreased oxygen to the location of injury reduces collagen synthesis. It is also thought that pressure increases apoptosis, reduces scar hydration stabilising mast cells and decreases angiogenesis.1,65 The application of pressure can be achieved using a variety of materials such as adhesive plaster moulds, pressure earrings and custom-fitted splints, 16 which have improved scar cosmesis and rates of keloid recurrence.66 –68 A continuous pressure of 20–40 mmHg, preferably at the lower range, soon after wound re-epithelialisation for 12–23 h per day for > 6 months is recommended.16,68,69 The efficacy of pressure therapy depends mainly on the anatomical location of the scar, with trunk and limb areas being more appropriate sites for pressure therapy. In addition, a pressure garment is predominantly used for auricular keloids where pressure clips are commonly utilised after surgery.66,70 As an adjuvant therapy, this form of pressure garment has also been successfully used to prevent the recurrence of keloids.66,67 In contrast, a meta-analysis review that analysed the effectiveness of pressure garment therapy for the prevention of abnormal scarring after burn injury was unable to demonstrate any beneficial effects of pressure garment therapy on prevention or treatment of abnormal scarring. 59 Notwithstanding, success rates of pressure therapy are contingent upon patient compliance 69 which can sometimes be low due to discomfort. Overall, pressure therapy is tolerated better and is devoid of the pain often associated with intralesional therapies and hence can be considered as a good adjuvant therapy for keloid scars.
Radiotherapy
In 1906, the treatment of keloids using superficial X-ray irradiation was first described. 71 Since then, it has been used less frequently as a monotherapy and more widely as an effective adjunct treatment after surgical excision72 –75 with success rates in the range of 67%–98% 76 and recurrence rates of about 22%. 77 Radioactive skin patches have also been used in combination with other treatment modalities for keloids.78,79 Radiotherapy is most commonly used 24–48 h after surgical excision74,80 and acts by suppressing angiogenesis and inhibiting fibroblast activity. 1 Decreased fibroblast proliferation, induced cell senescence and apoptosis, leading to reduction in collagen production and suppression of keloid development have also been reported.81 –83
Different radiotherapy modalities have been used after surgical excision including electron beam radiotherapy, brachytherapy, superficial and orthovoltage radiotherapy with varying degrees of success. 84 Mankowski et al. conducted a literature review of 72 studies to compare the clinical outcome of different forms of radiation treatment used for the management of keloids. 77 The meta-analysis demonstrated that radiation used as monotherapy yielded higher rates of recurrence (37%) compared to combinational therapy with post-surgery excision (22%). Comparison between the different radiation-based treatments revealed that the lowest rate of recurrence was observed with brachytherapy (15%), followed jointly by X-ray (23%) and electron beam (23%). The authors also reported that the rate of recurrence was dependent on anatomical site of the keloid with chest keloids having the highest recurrence rate. 73
The adverse effects of radiotherapy, often linked with dose of radiation used, can be grouped into acute skin reactions and late complications. Acute reactions arise as early as seven days after keloid treatment and include oedema, necrosis, ulceration, desquamation, erythema and pigmentary changes, with the latter two being the most common. Late complications, which include changes in pigment, atrophy, telangiectasis and alopecia, may present several weeks after radiotherapy. Emollient and steroid ointment used after radiotherapy can help alleviate the side effects. 19 A recommended radiation dose > 30 Gy over several sessions can also minimise adverse effects.19,80 Radiotherapy carries a risk of malignancy.85,86 Therefore, caution should be used in radiation-vulnerable sites such as the head, neck, thyroid and breast, and in patients aged < 18 years. 2 Protecting fragile organs and selecting the most appropriate site-dependent dose protocol can help minimise further complications of radiotherapy. 87
Cryotherapy
Cryotherapy is a low-temperature treatment that causes vascular damage, resulting in tissue necrosis. 88 It has been used to treat keloids as a monotherapy or in combination with other treatment methods such as intralesional steroid injections. 89 Various delivery methods used for cryotherapy include spray and contact probes, or the intralesional-needle cryoprobe method. Compared to contact and spray methods, intralesional-needle cryoprobe was found to be the most effective method in treating keloid scars. 90 Positive outcomes were observed in a number of studies that used liquid nitrogen and cryotherapy, to treat keloids with success rates in the range of 32%–74%.91 –93
External cryotherapy has been associated with several side effects including hypopigmentation, blistering, pain, delayed healing and infection.90,93 Moreover, larger keloids have been shown to need multiple cryotherapy sessions.90,93 To minimise side effects, intralesional cryotherapy was introduced and there are now a number of nitrogen-based cryodevices that have been described for the treatment of keloid scars, with two commercially available: a liquid nitrogen-based device 88 and an argon gas-based device. 94 The intralesional cryotherapy was designed to overcome the hypopigmentation seen mostly in dark-skinned individuals with external cryotherapy. It works by destroying the core of the keloid, sparing the surface epithelial cells including melanocytes.95,96 As a result, it enhances volume decrease while minimising the risk of hypopigmentation and other surface reactions. 90 A recent comprehensive review based on the preferred reporting items for systematic reviews and meta-analysis was performed to investigate the efficacy of intralesional cryotherapy on keloid scars. 90 The review of eight studies that met the inclusion criteria revealed that average scar volume decreased in the range of 51%–63%, but complete eradication of the scar on average was lacking. Recurrence of keloid scars was in the range of 0%–24%. 90 The authors also reported that patients’ complaints of pain and pruritus was considerably reduced; however, hypopigmentation was seen mostly in Fitzpatrick 4–6 skin type patients after treatment. 90
Laser therapy
Laser therapy for keloid treatment was introduced in the 1980s. 97 Since then, different systems have been used for the treatment of keloid and hypertrophic scars.48,98 These lasers target skin chromophores like haemoglobin and melanin, based on the principle of selective photothermolysis. 99 Lasers can be classified as ablative and non-ablative. The most common ablative lasers include the 2940-nm erbium-doped yttrium aluminium garnet (Er:YAG) laser and the 10,600-nm carbon dioxide (CO2) laser. These emit a laser beam that is absorbed by water in the skin leading to local tissue destruction and reduction of lesion volume. 3 Common examples of non-ablative lasers include 585-nm or 595-nm PDLs, 1064-nm neodymium-doped:yttrium-aluminium-garnet (Nd:YAG) laser, 532-nm neodymium-doped:vanadate (Nd:Van) laser and 1064 nm Q-switched Nd:YAG laser with low fluence. 100 These lasers induce thermal injury to the scar’s microvasculature leading to thrombosis and ischaemia which result in collagen denaturation and collagen fibre realignment.101 –103
Laser therapy requires several treatments at intervals of 4–8 weeks, depending on scar type and type of laser used98,104 with possible side effects including itching, pigmentary changes, blister formation and postoperative purpura. 98 The use of the non-fractional, vascular 585–595 nm PDL in the treatment of keloid and hypertrophic scars has been well-documented105 –108 and has response rates in the range of 57%–83%. 109 PDL monotherapy has been shown to be effective108,110 as well as CO2 laser monotherapy.38,111,112 In a clinical study where 50 patients with moderate to severe keloids were treated with high-energy pulsed CO2 laser, the treatment was efficacious and well-tolerated with minimal side effects. 112 In other studies where CO2 laser ablation was compared with other forms of treatment, CO2 laser was as efficient as the other forms.38,111 It must be noted, however, that these studies are small and randomised controlled studies are lacking. 98
Laser therapy such as PDL, CO2 and Nd:YAG have been associated with a high rate of recurrence at 6–24 months.111,113 –115 However, optimal results can be achieved with combination treatment especially with intralesional TAC injections.116 –118 Kumar and co-workers conducted a cohort study on 17 patients with keloids previously treated with an Nd:YAG laser and reported complete scar resolution and flattening in seven patients only when intralesional TAC was used after laser therapy. 41 Moreover, combined therapy with PDL and TAC 119 and PDL, TAC and 5-FU 36 were shown to produce better clinical results. In a recent study that evaluated and compared the efficacy of combination therapy of fractional CO2 laser and intralesional TAC injection or TAC injection alone in keloid and hypertrophic scars, statistically significant improvements were reported in overall scar quality with the combined treatment options compared to TAC monotherapy. 120 Moreover, combined CO2 laser and IFN-α-2b injections given to patients with auricular keloids resulted in no recurrence in 66% of patients three years after treatment. 121 Laser therapy can also be combined with other laser treatment, topical corticosteroids and cyanoacrylate glue 98 and have shown promising results; however, larger, controlled clinical studies are needed to further evaluate their efficacy and safety.
Recently, lasers are also being explored as tools for assisted drug delivery. Kraeva et al. proposed an alternative technique of corticosteroid administration of laser-assisted drug delivery of topical TAC. This was shown to be effective when used on a keloid on the posterior scalp of a patient after each CO2 laser session. 122 More efficient intraepidermal drug delivery options are also being investigated. Singhal et al. developed TAC-containing polymeric microparticles that were prepared using a cryomilling technique for freezing fracture. After ablation with a fractional Er:YAG laser, these microparticles can be deposited in cutaneous micropores and provide high-dose intraepidermal reservoir systems with minimal transdermal permeation, leading to sustained and targeted local drug delivery. 123
It must be noted that one of the biggest limitations in studies available at present is the lack of histological definition between keloid and hypertrophic scars, so conclusions are not 100% valid on efficacy.
Imiquimod 5% cream
Imiquimod 5% cream is approved for the treatment of basal cell carcinoma, actinic keratoses and genital warts. 21 As an immune-response modifier, it stimulates the production of proinflammatory cytokines such as TNF-α, interleukins and IFNs by activated T-cells 124 thereby changing the expression of genes associated with apoptosis 125 and reducing collagen production. 16 Studies have reported conflicting findings regarding efficacy of imiquimod 5% cream postoperatively following keloid excision, likely due to keloid location. Many studies have reported reduced recurrence of earlobe keloids in patients following treatment with postoperative imiquimod 5% cream.126 -128 A recent study has also tested the use of a fabricated imiquimod-poly(MEO2MA) hydrogel dressing on cell viability of cultured keloid fibroblasts and showed a 34% reduction of cell viability after 2 days, suggesting its benefit in keloid therapy. 124 By contrast, other studies have reported the recurrence of presternal keloids 129 and trunk keloids 130 post keloid excision. Imiquimod 5% cream is widely used in clinical practice as a topical application for 8 weeks post-surgery. It is cost-effective, simple and safe to use with minimal side effects including mild irritation, hyperpigmentation and clinical impetiginisation. 126 For these reasons, it has generally been considered as an effective adjuvant treatment alternative for the prevention of recurrences in excised keloids. However, larger controlled studies are needed for further investigation.
5-Fluorouracil
5-FU is a pyrimidine analogue that inhibits thymidylate synthase enzyme leading to suppression of nucleic acid synthesis and cell proliferation. It inhibits fibroblast proliferation, angiogenesis and TGF-β-induced collagen type I expression while increasing fibroblast apoptosis without necrosis.1,131 In the last 30 years, this chemotherapy drug has been used to treat keloids although some controversy exists regarding its efficacy. 132 Intralesional injections of 5-FU can be used alone or in combination with other forms of therapy. One study reported the successful use of intralesional injections of 5-FU (50 mg/mL) weekly for 12 weeks. 133 Bijlard et al. conducted a systematic review of the clinical evidence on the efficacy of 5-FU in keloid treatment and showed that this form of treatment was effective in 45%–96% of patients and that combination therapy of intralesional 5-FU and TAC injections produced better results. 131 Similarly, other studies have also demonstrated that a combinational treatment approach of intralesional 5-FU and TAC injections led to improved clinical outcomes.40,45 Meta-analysis of scar height and erythema, and patient satisfaction after treatment demonstrated improvements using combined therapy. 45 Moreover, a recent double-blind randomised controlled trial study with 43 patients with 50 keloids reported that TAC and 5-FU injections did not differ in their clinical effectivity, but 5-FU injections alone led to increased fibroblast proliferation rate and did not affect vascular density in histological assessment. 134 However, as more adverse effects were observed after TAC treatment compared to 5-FU injections, it was suggested that 5-FU injections may be preferable for cosmetically sensitive skin areas. 134 Haurani et al. demonstrated the efficacy of surgical excision and 5-FU combined therapy on patients with a recurrence rate of only 19% at one-year follow-up. 135 Intralesional 5-FU has possible side effects including skin erythema, pain and ulceration 136 but is safe and is proving to be a promising mode of keloid therapy. 40
Emerging treatments
Stem cell therapy
Adult stem cells have been gaining traction over the years as potential candidates for cell-based wound repair and scar therapy. Mesenchymal stem cells (MSCs) have been well described with numerous studies having demonstrated their potential to accelerate wound repair by increasing migration, angiogenesis and re-epithelialisation via paracrine signalling.137,138 MSCs secrete growth and differentiation factors that regulate inflammatory and immune responses during wound healing.139,140 The cells can be delivered to the wound either directly (e.g. through injecting, spraying or systemic administration) or via skin scaffolds. 138 Recently, the antifibrotic properties of MSCs, though paracrine signalling, have been demonstrated in vitro in keloid fibroblasts and in a dermal fibrosis murine model.141,142 These findings have provided new understanding and MSC-based therapeutic application for scar treatment. Some studies, however, have reported possible pro-inflammatory effects of MSCs, which promote formation of keloids. 143 Hence, more studies are needed to elucidate their efficacy in keloid treatment.
Fat grafting has recently been explored as an adjuvant therapy for keloid and hypertrophic scars. 144 It has been shown to improve scar cosmesis and enhance tissue regeneration in burns patients with keloids.145,146 The underlying mechanisms by which fat grafting augments scar quality are not clear. However, it is known that these grafts contain adipose stem cells (ASCs) which have the ability to differentiate into a variety of tissues and exhibit a number of properties including angiogenic and anti-apoptotic properties, which aid in soft-tissue maturation and scar remodelling.147,148 In vivo studies have also demonstrated the effect of ASCs in the quality of wound repair and scar formation by modulating fibrogenesis through increased collagen production and by inhibiting fibroblast proliferation. 149 These inherent biology properties of ASCs contained in fat grafts render these grafts a potentially valuable adjunct therapy for keloid scars.
Mitomycin C
The antibiotic mitomycin C (MMC), isolated from Streptomyces cespitosus, has traditionally been used as a chemotherapeutic agent and more recently as an anti-scarring agent used in ophthalmologic and otorhinolaryngologic surgery. 150 MMC inhibits nucleic acid and protein synthesis and thereby inhibits cell proliferation. 151 MMC has been shown to hinder proliferation of human cultured fibroblasts in vitro 152 and reduce scar formation in vivo. 153 In a prospective experimental study, topical application of MMC impeded wound healing in rats within the first month after treatment; however, three months after treatment, both treated and untreated wounds displayed similar histological characteristics. 154 The authors therefore suggested that MMC initially delayed wound healing but, ultimately, did not alter the final fibrosis outcome. 154 In another study, topical application of MMC to full-thickness wounds in a murine model reduced the rates of wound contraction. 153
MMC has been administered topically or intralesionally to treat keloids with varying degrees of success.155 –158 A retrospective study involving 10 patients treated with topical MMC (0.4 mg/5 mL) for 4 min followed by head and neck keloid excision, demonstrated recurrence in only one patient. 158 In another study, keloid and hypertrophic scars treated with topical MMC showed good results while lesions treated with intralesional MMC increased ulceration. 156 With regard to keloid recurrence, one study conducted by Sanders et al. reported no difference in prevention of keloid recurrence after surgical excision when MMC was applied topically or used in combination with intralesional TAC. 155 Taken together, findings from these studies indicate that MMC can be viewed as a potential agent in the treatment of keloids. However, larger randomised clinical trials are needed to further elucidate its efficacy and best mode of administration.
Verapamil
Verapamil is a calcium channel blocker that accelerates degradation of scar tissue by inducing procollagenase secretion. This alters fibroblast shape, induces TGF-β1 apoptosis, reduces ECM production and depolymerises actin filaments. 159 Intralesional verapamil is safe and has been used in the treatment of keloid scars. 160 Its use in abdominoplasty and mammoplasty scar treatment was shown to avoid the development of keloids and hypertrophic scars after plastic surgery. 160 Another study comparing effectiveness of intralesional TAC and verapamil, accompanied by cryotherapy on scar outcome, indicated that both groups displayed a reduction in scar height and pliability; however, better improvement was reported with TAC. 161 Moreover, a recent double-blind randomised controlled trial also reported that verapamil was not as effective as TAC in preventing keloid recurrence after surgical excision. 162 When used as a part of combinational therapy with pressure therapy, 163 PDL, 107 TAC, 164 nifedipine 165 and others, verapamil was shown to be effective. Combined therapy with verapamil and pressure therapy improved pigmentation, vascularity, elevation, flexibility and pruritus of keloids arising from burn injuries. 163 A recent study conducted by Khattab et al. that used a combinational approach of verapamil and PDL in the treatment of keloids showed superiority in efficacy with improved height and length of the lesions with the combined therapy approach compared to intralesional verapamil used alone. 107 Furthermore, a retrospective study in which the efficacy of combined TAC and verapamil treatment for hypertrophic and keloid scars in 58 patients was investigated, scar surface area, scar relief, pain, itchiness, as examined by means of the Patient and Observer Scar Assessment Scale, reported vast improvements with combined therapy. 164 Morelli et al. also reported in their study that combined use of TAC and verapamil was more effective on keloid scars in the long term, whereas, alone, treatment with TAC had a faster and more effective response but with increased complication rates compared to verapamil alone. 3 Findings from these studies therefore indicate that intralesional verapamil, which is safe to use with minimal adverse effects, is more effective and offers long-term stable results when used as a part of combinational therapy.
Interferons
IFNS are cytokines that have many functions including attenuating fibrosis. 166 There are three IFN isoforms, namely, IFN-α, IFN-β and IFN-γ, and these, particularly IFN-α and IFN-γ, have been shown to decrease collagen and other ECM expression while increasing collagenase activity.1,167 IFN-γ has been found to have antiproliferative properties in vitro 168 and in vivo; IFN-α and IFN-γ were shown to have beneficial effects on keloid regression and recurrences.121,169,170 Conversely, a prospective controlled clinical study reported that IFN-α-2b treatment was not effective as a post-excisional adjuvant therapy for keloids as a 54% recurrence rate was seen. 171 When used as combinational therapy with intralesional TAC and CO2 lasers, IFN effects appear to improve, leading to lower rates of recurrence and favourable outcomes.34,168 Intralesional IFN injection is typically used at 1.5 million IU twice daily for four days in keloids. 8 Side effects in-clude pain at injection site, flu-like symptoms, 170 myalgia, 167 local erythema and oedema. 34 Based on findings obtained from experimental and clinical studies, IFN remain promising candidates for the treatment of excessive scarring; 21 however, further controlled studies are needed.
Bleomycin
Bleomycin is a chemotherapy agent with antiviral and antibacterial properties. 15 It has been shown to diminish TGF-β1-induced collagen expression and increase apoptosis.34,172 The levels of lysyl-oxidase, a cross-linking enzyme involved in collagen maturation, is also decreased by bleomycin. 173 Bleomycin inhibits the synthesis of DNA, RNA and proteins, and is cytoxic to keratinocytes and eccrine epithelium. 174 In recent decades, it has been used in the treatment of keloids and hypertrophic scars. The recommended dose for intralesional bleomycin injection begins at 0.1 mL (1.5 IU/mL) and can be administered to a maximum dose of 6 mL, to obviate toxicity risks, for 2–6 sessions per month. 34 Treating patients whose keloid and hypertrophic scars were refractory to intralesional steroids with bleomycin injections for this length of time was shown to be effective and safe.73,175 Bodokh and Brun reported a regression of 84% of 31 keloids after 3–5 intralesional infiltrations of bleomycin were administered to patients within one month. 176 Since then, other studies have also demonstrated good outcomes with bleomycin treatment.175,177,178 In a recent study, Huu et al. evaluated the efficacy of bleomycin injections on 55 patients with 120 keloids of different sizes and location at monthly intervals with an average of four injections. Of scars, 70.8% became completely flat, 8.3% fairly flat, 17.5% comparatively flat, 3.3% averagely flat and there were no poorly flat scars. However, a high rate of recurrence up to 18 months after treatment was observed. The authors also reported local side effects including pain, blisters, ulceration and hyperpigmentation. 5 Bleomycin has been shown to be equally effective when administered via intralesional injection,176,179 dermojet injection, 179 multiple needle punctures 177 or tattooing techniques. 178 Although safe, side effects of the drug can include pain at injection site, cutaneous issues, hyperpigmentation, ulceration and dermal atrophy.15,174,175
Botulinum toxin type A
Botulinum toxin type A, isolated from Clostridium botulinum, is a potent neurotoxin that blocks neuromuscular transmission. It has been shown to improve scar cosmesis by decreasing tension on healing wound edges, 180 accumulating fibroblasts in GO and G1 of the cell cycle 181 and reducing TGF-β1 expression. 182 In a prospective, uncontrolled study, 12 patients with keloids were treated with intralesional botulinum toxin type A injection at a concentration of 35 units/mL, with the total dose in the range of 70–140 units per session, at three-month intervals for 3–9 months. 183 This led to good treatment outcomes, high patient satisfaction with no serious adverse effects or signs of keloid recurrence. 183 Similar outcomes have also been reported from two prospective clinical studies184,185 and one randomised controlled trial. 186 However, other studies have shown conflicting results and found no major benefits of botulinum toxin type A injections for the treatment of keloids.187,188
ACE inhibitors
The local renin-angiotensin system has been shown to modulate collagen production and wound healing, and plays a role in fibrotic diseases.189,190 Angiotensin-converting enzyme (ACE) inhibitors, are drugs that are widely used in the treatment of hypertension and inhibit the generation or action of angiotensin (Ang) II at tissue sites. 191 A variety of ACE inhibitors are available and include captopril, enalapril, ramipril, lisinopril, fosinopril among others. 192 Niazi et al. recently evaluated the concentrations of Ang II and one of its major receptors, AT1, in patients with keloids, hypertrophic scars and in a normal group using enzyme-linked immunosorbent assay techniques. Elevated AT1 receptor concentrations were seen in patients with keloids compared to hypertrophic scar and normal groups, whereas Ang II was higher in the hypertrophic group compared to the normal and keloid groups. The authors suggested that keloid and hypertrophic scars could be stimulated by Ang II and AT1 receptor concentrations and therefore use of Ang II receptor blockers and ACE inhibitors could be potential agents for scar treatment. 190
ACE inhibitors have been shown to inhibit collagen synthesis and deposition and delay healing of chronic wounds in patients.193,194 However, healing rates are improved when collagen-based dressings are applied to the ulcers.193,195 In vitro, the effect of the ACE inhibitor captopril on keloid fibroblasts was found to reduce the expression of Ang II, TGF-β1, PDGF-BB, heat shock protein 47 and inhibit fibroblast proliferation and collagen synthesis, known key players in keloid formation. 196 ACE inhibitors have been successfully used to treat patients with keloids,192,197 with keloids of shorter duration showing better improvements compared to long-standing lesions. 192 However, to date, only few clinical studies have been conducted; hence, further research is required to investigate the efficacy of ACE inhibitors as a therapeutic potential in keloids.
Conclusion
In this review, we have provided a comprehensive summary of the common concepts surrounding keloid formation and discussed current and emerging therapies to date. Keloids are problematic and disfiguring scars that result from abnormal wound healing and excessive fibrosis. Fibroblast over-proliferation along with over-production and deposition of collagen and other ECM are key players in the development of keloids. Genetic and other factors also contribute to keloid formation. These scars are difficult to treat and manage and present a major clinical challenge. While progress has been made over the years in elucidating some of the underlying mechanisms surrounding keloid aetiopathogenesis, much remains to be translated into the clinical setting.
Various modes of keloid therapies are currently available and emerging therapies are also being investigated. To date, no one therapy has been universally accepted as the gold standard for the treatment of all keloids nor has the capability of complete scar resolution. Some of these treatments offer more benefits and are more efficacious than others. Treatment with corticosteroid injections have been shown to reduce keloid scar size and irritation and show regression rates in the range of 50%–100% after one year; however, injections are painful. Surgical excision has been used traditionally but creates a new wound which can result in a similar or larger keloid. It is also not recommended as a monotherapy as it results in high rates of recurrence. Radiotherapy is used as an effective adjunct treatment after surgical excision with good success rates and low recurrence rates; however, it remains controversial as it carries a risk of cancer. The rate of success for cryotherapy is in the range of 32%–74% but this form of treatment is often associated with several side effects, in particular, hypopigmentation. Silicone-based products and Imiquimod 5% cream offer safe methods of treatment with minimal side effects; however, larger, controlled clinical studies are needed to further evaluate their efficacy and safety. Hence, with keloids, combinational therapy offers the best approach and has shown greater efficacy with fewer side effects compared to monotherapy.
Carrying out a comprehensive clinical assessment and full medical history 24 is important before deciding on the best treatment option for the patient. A well-planned treatment that is tailored to the patient’s specific needs is essential in producing good clinical outcome. The physician’s role in educating the patient on keloids, emphasising the importance of self-active participation in wound care 52 and compliance, and explaining any potential adverse effects are equally important for achieving good scar cosmesis. Patients’ pain, pruritus and inflammation should be kept under control 24 and the scar site should be closely monitored with regular follow-ups to prevent the recurrence of keloids. Adopting these approaches, as well as conducting well-designed research and clinical studies to gain further insight into the underlying mechanisms of keloid development and to evaluate the clinical efficacy and safety of various treatments, will hopefully lead to better patient outcomes and treatment options for these pathological scars.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.