
Abstract
Background
Surgical decompression of the carpal tunnel is considered the method of choice for its treatment with satisfactory results documented. Various methods and suturing materials have been used for closure of the surgical wound. In the present study, we compared interrupted mattress closure by means of nylon suture to running subcuticular closure with vicryl rapide suture. As far as we know, there is no similar study in the literature.
Methods
A total of twenty patients were included in the study. Ten of them had their surgical wound closed with 3.0 nylon suture in an interrupted fashion and for the rest, a running subcuticular 3.0 vicryl rapide was used. All patients filled in a questionnaire about VAS perceived pain and a Quick DASH score sheet, preoperatively, at two and six weeks postoperatively. The cosmesis of the scar was assessed using the POSAS v2.0 system at two and six weeks after surgery and overall incidence of infections was noted as well.
Results
There was no statistically important difference between the two groups of patients in regards to postoperative VAS pain levels at two and six weeks. Likewise, no statistically significant difference was evident as far as Quick DASH score, POSAS score and infections were concerned.
Conclusions
Our results suggest that the use of running subcuticular vicryl rapide suture is an attractive alternative to interrupted nylon sutures for closure after open carpal tunnel decompression, lacking any significant drawbacks.
Lay Summary
Surgery for carpal tunnel decompression is considered the method of choice for its treatment with documented satisfactory results. Various methods and suturing materials have been used for closure of the surgical wound. In the present study, we compared the use of a non-absorbable suture, placed intermittently to an absorbable continuous intradermal suture. A total of twenty patients were included in the study. Half of them had their wound closed with the absorbable suture and the other half with the non-absorbable suture, as described above. All patients were evaluated as far as pain, scar characteristics, functional outcomes of the operated hand and incidence of infection, at two and six weeks after surgery. After analysis of the data, no significant differences were found between the two groups, suggesting that both of these techniques are equally safe and efficacious.
Introduction
Carpal tunnel syndrome belongs to a group of peripheral neuropathies of the upper extremity, and is one of the most common hand disorders.1–4 Although various therapeutic approaches are described in the literature, 3 both conservative and surgical, dissection of the transverse ligament is the treatment method of choice, leading to decompression of the carpal tunnel contents including the median nerve.
Several closure techniques have been reported in the literature for reapproximating the surgical incision made for carpal tunnel release.5–13 Absorbable, non-absorbable and surgical steel sutures have been implemented and various suturing techniques have been used for carpal tunnel syndrome.
As far as we know there are no studies in the literature comparing interrupted mattress closure with nylon suture to running subcuticular closure with vicryl rapide, in terms of reapproximating the wound after open carpal tunnel release and this was the scope of this study.
Materials and methods
This was a prospective cohort study involving twenty patients diagnosed with carpal tunnel syndrome.
In all patients the diagnosis of the syndrome was based on both clinical examination as well as confirmation by electrophysiological study.
Patients with a previous distal radius fracture, previous carpal tunnel surgery, pregnancy, diabetes mellitus and rheumatic diseases were excluded from the study.
The patients were pooled from the elective surgery waiting list of the General District Hospital of Ioannina Hatzikosta one of the authors and were divided into two groups of ten individuals each, using a table of random numbers. In one group the surgical wound approximation was performed using interrupted mattress nylon 3.0 suture, and in the other group running subcuticular vicryl rapide was used.
The patients were operated by the same orthopedic surgeon and were aware of the surgical technique about to be applied. All patients were informed of their participation in this study and the capture of photographic material and agreed by signing a consent form. All procedures followed were in accordance with the ethical standards of the committee on responsible human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008 (5). Informed consent was obtained from all patients for being included in the study (VT).
Carpal tunnel release was performed with the application of a pneumatic tourniquet inflated to 220mmHg.
Local anesthesia was applied, using 10ml of a mixture with equal volumes of 5% lidocaine and 75mg/10ml ropivacaine, with a 22G needle. All patients received a prophylactic dose of cefoxitin 1gr i.v prior to the application of tourniquet cuff pressure.
The sutures used for the patients were 3.0 nylon for the interrupted mattress sutures and 3.0 PGLAR polyglactin rapid absorption (vicryl rapide) for the running subcuticular suture.
Immediately after surgery, Steri-stripsTM were placed over the incision site along with a sterile gauze and the operated limb was bandaged with cotton and gauze roll, with simultaneous placement in suspension. All patients were instructed to mobilize the fingers freely postoperatively, take paracetamol 1 gr orally three times daily for two days, present themselves for dressings change on the second postoperative day in the outpatient clinic settings and avoid strenuous activities involving the operated hand for a total of four weeks. Sutures in the group with interrupted nylon suture were removed on the 15th postoperative day.
In the present study, we recorded the reported pain of patients due to carpal tunnel syndrome, based on Visual Analog Scale (VAS), both preoperatively and at two weeks and six weeks postoperatively. The VAS scale uses a 0 to 10 rating to assess pain and is widely used in clinical practice as well as research methodology.14–17
At the same time, the patients completed preoperatively and postoperatively at two and six weeks, the Quick Disability of Arm Shoulder and Hand (DASH), which is a widely accepted tool for the assessment of upper limb function and is used in the literature to document function and quality of life after upper limb interventions.
Regarding the third parameter that we studied concerning the assessment of the postoperative scar, we submitted an application presenting the design and aim of the study and eventually received official permission to use the Patient and Observer Scar Assessment Scale (POSAS) v2.0.
Several assessment scales for postoperative scars are mentioned in the literature and this issue has been a thoroughly examined field of research in plastic surgery and orthopedics, but mainly in hand surgery .18–23
The POSAS form concerns both the examiner and the examinee. The examinee evaluates pain, itching, thickness of scar, color, stiffness and relief of scar. The observer examines vascularity, pigmentation, thickness relief, pliability and surface area of the scar. The POSAS system methodology provides clear instructions for evaluating each parameter, which cannot be done using photographs since some parameters are clinically assessed by feel and applying pressure over the scar area. Each parameter in the POSAS system gets a score from 1 to 10, with 1 corresponding to normal skin and 10 to skin that differs by far from normal. The total score results from the sum of all scores of the six parameters and can range from 6 to 60.
In the present study we solely used the POSAS Observer scale as not all patients were happy to provide this information, due to lack of confidence.
Results
Twenty patients participated in this study; 14 females and 6 males. Mean age for the nylon suture group was 45.7 (26–71) and 50.3 (25–75) for the vicryl rapide group.
All patients in both groups exhibited a statistically significant improvement after the surgical decompression of the carpal tunnel, as measured by the results of the VAS and Quick DASH score sheets independently.
The mean preoperative VAS score for the nylon group was 7.6 (6–10), followed by 4.8 (3–7) and 1.5 (0–4) at two and six weeks after surgery respectively. The mean VAS score for the vicryl rapide group was 8.3 (3–10) preoperatively, 4.6 (3–7) at two weeks and 1.4 (0–5) at six weeks postoperatively. Performing the Mann-Whitney test between the two groups, no statistically significant differences were noted as p value was 0.187 preoperatively, 0.724 at two weeks and 0.523 at six weeks, all greater than p value 0.05 level of significance (see Table 1).
VAS score comparison between nylon and vicryl rapide group.

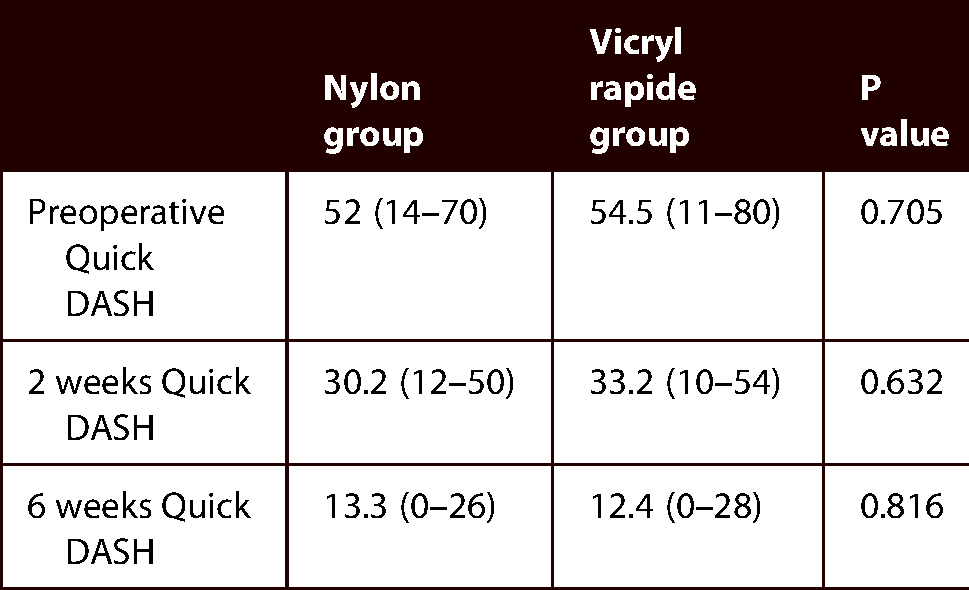
The mean preoperative Quick DASH score for the nylon group was 52 (14–70), 30.2 (12–50) at two weeks and 13.3 (0–26) at six weeks after the operation. The mean preoperative Quick DASH score for the vicryl rapide group was 54.5 (11–80)and 33.2 (10–54) at two weeks and 12.4 (0–28) at six weeks respectively following surgery. No differences were found after comparing the two groups since individual comparison preoperatively showed a p value 0.705, p value of 0.632 at two weeks and p value of 0.816 at six weeks postoperatively (see Table 2).
Quick DASH score comparison between nylon and vicryl rapide group.
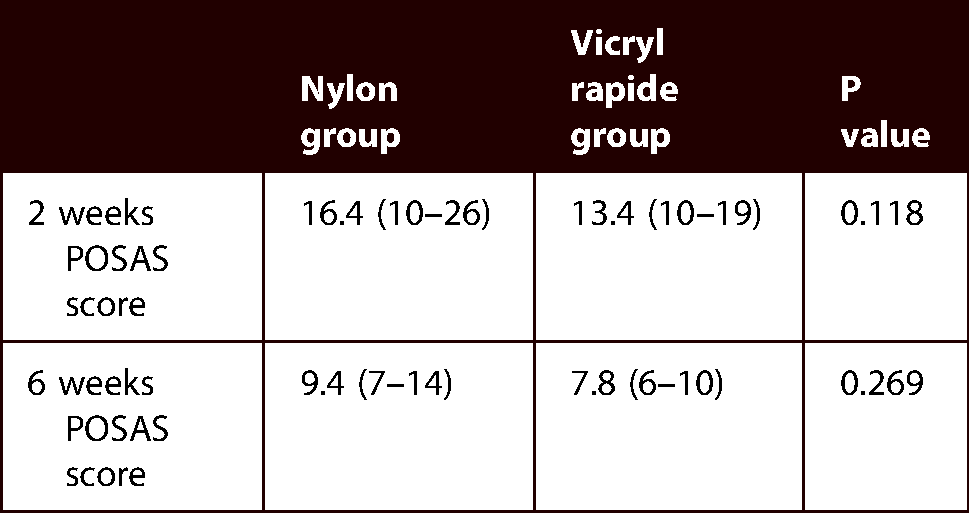
The mean POSAS score for the nylon group was 16.4 (10–26) at two weeks and 9.4 (7–14) at six weeks after surgery. The mean POSAS score for the vicryl rapide group was 13.4 (10–19) and 7.8 (6–10) at two and six weeks respectively. Comparing the two groups showed no significant statistical difference as the p value at two and six weeks after surgery was 0.118 and 0.269 respectively (see Table 3).
POSAS score comparison between nylon and vicryl rapide group.
In regards to the infection rate, there were no differences in the statistical analysis of the two groups at the end of the six weeks follow up in clinic (p = 0.146).
Discussion
Carpal tunnel release is one of the most common upper limb surgeries. Concerning wound closure, although non-absorbable nylon sutures have traditionally been used, the use of absorbable vicryl sutures including vicryl rapide has recently become more frequent.6,8,11
The use of non-absorbable sutures has been tied to disadvantages such as producing suture marks at the needle entry points and the need for removal which causes stress and discomfort to patients, and outpatient visits to the clinic are necessary, thus increasing the workload in healthcare organizations.
Absorbable sutures have the advantage of eliminating the need for removal and this is why they have become the primary choice for orthopedic extremity operations for a significant share of surgeons. On the other hand, they have been associated with an increased likelihood of granulomas and inflammatory reaction, especially when placed intradermally.6–8,10,11
Modern options, in terms of upper extremity interventions and especially carpal tunnel release, include nylon, vicryl and vicryl rapide. Nonetheless, the use of stainless surgical steel is reported in the literature with comparable results to nylon sutures. 5 The difference between the two types of vicryl sutures lies in their absorption rate as vicryl rapide is absorbed much faster. Vicryl rapide is fully absorbed in 42 days, has 50% of its strength in five days and loses all of its strength in 14 days. In contrast, plain vicryl retains 75% of its strength in 14 days and 50% in 21 days.24,25 This difference in their properties has been investigated for their association with postoperative pain, final aesthetic result and also for possible postoperative complications.5–8,10,12,13,24
As far as we know, at the time of writing, even though there are comparative studies between the two sutures that we studied, in the case of the vicryl rapid absorption suture, no studies have been conducted using the running subcuticular technique.
In our study, patients in both groups showed a statistically significant reduction in postoperative pain validating the success of median nerve decompression surgery.
However, no statistically significant difference was observed between the two groups, as far as postoperative pain is concerned, both at two and six weeks, which is in line with the findings of reported studies.5,6,8,11,13 It seems that the type of suture affects neither postoperative pain nor the sensitivity of the surgical wound. In a reported study 26 that stated higher levels of pain, the pain referred to the time of removal of the non-absorbable sutures and not the overall postoperative pain, whereas in another paper, 11 where higher levels of pain were reported on the 10th day in the group with the non-absorbable suture, no differences were observed at the end of the 6th week between the nylon suture and the vicryl suture group.
Regarding the cosmetic evaluation of the surgical scar, the analysis of the POSAS assessments between the two groups in our study, did not show a statistically significant difference. The surgical incision performed for open decompression of the carpal tunnel has the advantage that it is linear and standardized without raising and mobilizing the skin. In those type of incisions, assessment with POSAS questionnaire is quite successful and reliable. 26
When sutures enter human tissues, they are treated as foreign bodies (corpus alienum) inciting inflammation. This inflammatory process leads to redness, heat, swelling and tenderness while granulomatous tissue is accumulated around the foreign body. This inflammatory response is more pronounced in absorbable braided and superficially placed sutures.6–8,10
In our study, for patients receiving running subcuticular suture with vicryl rapide, we hypothesized that the superficial placement and the presence of greater amount of suture material per unit of skin surface compared to interrupted sutures, would translate into a difference in the cosmetic outcome of the postoperative scar and in POSAS assessments, alas this was not observed. These results fall in line with current bibliographic comparisons of absorbable and non-absorbable sutures as far as the final cosmetic outcome of the surgical scar is concerned.5,6,8,10,12,13,26
The beneficial effect of carpal tunnel release in cases of compressive peripheral neuropathy of the median nerve at the level of the wrist is well documented, both in clinical practice and in the literature. In the present study, we wanted to investigate whether surgery using two different sutures could induce measurable differences in the overall functionality of the upper limb. The quantification of the data provided by the patients was done with the widely accepted and reliable Quick DASH score system, even though several evaluation systems are used in the literature.27–30 All patients showed a marked improvement in upper limb function, but no statistically significant difference was observed between the two groups regarding this parameter, an outcome that conforms with the findings of previously reported studies.6,8
The last parameter studied was the incidence of microbial infections in the surgical wound. While braided sutures are associated with a higher probability of microbial infections as they provide a more suitable breeding ground for bacteria 31 and despite the use of running subcuticular suture in the vicryl rapide group that buried more suture material per unit of skin surface, there was no statistical difference between the groups. Nevertheless, a higher incidence of infections in patients with vicryl sutures than in those with steel and nylon sutures has been reported. 5
We recognize that the present study has two limitations. The population of both groups is relatively small and the follow-up period of six weeks is relatively short, yet the six-week mark has also been used in other published studies and we believe the study size and timescales are sufficient to draw the relevant conclusions.
Conclusions
The use of rapidly absorbable polyglactin sutures for closure of the surgical wound after open carpal tunnel decompression is a safe and reliable practice which does not appear to be inferior to non-absorbable sutures even when a running subcuticular suture is applied. A transition to subcuticular sutures in this and other aspects of hand surgery has the potential to reduce the volumes of patient reattendance for suture removal to the benefit of both patients and health services as a whole, freeing up substantial resource. Once less appointments are needed for this common surgical procedure nationally it would likely have a substantial beneficial impact on cost and waiting times.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Informed consent was obtained from all individual participants included in the study. All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008 (5).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article
How to cite this article
Tzimas V, Kotsias C, Galanis C, Panagiotakopoulos G, Tsiampas D, Parnis J, Tilkeridis K and Fiska A. Comparative study of surgical wound closure with nylon interrupted sutures and running subcuticular vicryl rapide suture after open release of the carpal tunnel. Scars, Burns & Healing, Volume 8, 2022. DOI: 10.1177/20595131221128951.