
Abstract
Introduction
Keloids are hypertrophic scars that commonly arise in the ear region. The authors’ objectives were to (1) evaluate effectiveness of surgical shave excision followed by intralesional triamcinolone acetonide and onabotulinumtoxinA injections; and (2) evaluate safety and patient satisfaction.
Methods and Materials
This study was a retrospective chart review of patients who received treatment of extralesional surgical shave excision followed by intralesional triamcinolone acetonide and onabotulinumtoxinA injections to treat ear keloids at a single outpatient dermatology clinic. A prospective patient questionnaire was administered to the same patient population to collect recurrence and patient satisfaction.
Results
A total of 45 patients were included, consisting of 84.4% females (n = 38) and 15.6% males (n = 7) with a mean age of 25.5 years. Through retrospective chart review, early recurrence was seen in 6.7% of patients (n = 3), and via the prospective patient questionnaire, 11.1% of patients noted early keloid recurrence (n = 5). Of the patients who expressed their level of satisfaction in-clinic, 96.0% (n = 24) reported being satisfied or very satisfied and 4.0% (n = 1) were dissatisfied. Satisfaction was also assessed through the prospective patient questionnaire; of those who consented to the questionnaire, 100.0% (n = 24) were satisfied or very satisfied. Only 20.0% (n = 9) of all patients reported experiencing side effects, consisting of pruritus (11.1%; n = 5), tenderness (4.4%; n = 2), pain (2.2%; n = 1), and mild atrophy (2.2%; n = 1).
Conclusion
Extralesional surgical shave excision followed by intralesional triamcinolone acetonide and onabotulinumtoxinA injections may represent a promising treatment option for ear keloids.
Lay Summary
Keloids are a type of raised scar, which can be painful and itchy for patients. Keloids can occur on various part of the body, including on the ear. They are challenging to treat and tend to come back. There are many treatment options, however, there is not one universal best treatment for keloids on the ear. We hoped to discover if shave excision followed by intralesional triamcinolone acetonide and onabotulinumtoxinA injections is effective at treating keloids on the ear. In order to answer this we completed a chart review of clinic patients, who have already completed the following combination treatment for keloids on the ear. The keloids were treated first by physically removing the bulk of the keloid with a scalpel, which is called shave excision. After the removal, triamcinolone acetonide and onabotulinumtoxinA were injected directly into the keloid. The rate of patient satisfaction and the rate of the keloid returning were collected during in-clinic visits and an optional post-clinic patient questionnaire. The treatment effectiveness and side effects experienced were reported during in-clinic visits. This indicated that with the low rate of side effects, high patient satisfaction, and low rate of keloid return, this treatment combination should be considered as an option for keloids on the ear. However, since this review was completed at one clinic with a small population of patients, it is not fully known if this treatment combination will work for all patients.
Introduction
Keloids are benign fibrous proliferative tumors that are a result of excessive scar formation that extends past the boundaries of the original injury.1,2 Keloid scars present as firm nodules, they do not spontaneously clear, and patients report pain and pruritus. 1 Keloids are often located on the shoulder, chest, back, neck, ear and the umbilical region. 1 The exact etiology of keloid development is unknown; but it has been suggested to be caused by skin traumas secondary to surgical wounds, burns, body piercings, folliculitis, or acne. 2
The earlobes and helices are common spots for keloid development with an incidence rate of 2.5%. 3 Due to the increased commonality of piercings in the ear region, keloid formation is more likely here than in other body areas. 3 Ear keloids present cosmetic and psychological issues for patients due to their highly visible locations and are often management challenges for physicians. Many treatment options exist; however, there are no specific guidelines toward a single best treatment. Existing methods include surgical excision, laser therapy, corticosteroid injections including triamcinolone acetonide (TA), botulinum toxin injections, radiotherapy, fluorouracil (5-FU), and cryotherapy. 4 Due to high keloid recurrence and treatment resistance, many physicians have opted for the use of multimodal treatments.
Surgical excision removes excess scar tissue and can be used for large keloids as well as debulking or removal of infected regions.5,6 Surgical excision alone leads to high recurrence rates between 45 to 100%, which is why it is seldomly used as monotherapy and rarely the first treatment choice.5,7 In this study, the use of surgical shave excision was used primarily to debulk the keloid.
Intralesional (IL) TA as an adjunct to excision has low morbidity, is cost-effective, is easy to administer, and provides reliable and long-lasting results. 8 Corticosteroids work by suppressing wound inflammation, decreasing collagen synthesis, and minimizing fibroblast proliferation.9–14 Side effects are minimal but may include hypopigmentation or hyperpigmentation, telangiectasis, skin atrophy, or pain.13,14 The main role of IL injections post-surgical shave excision is to prevent keloid recurrence. On its own, IL TA injections have great response rates ranging from 50 to 100% as well as recurrence rates of 9 to 50%. 14 When used in conjunction with surgical excision, corticosteroid injection resulted in 94% of patients being successfully treated with no lesion recurrence after six months. 9 Similarly, injections of onabotulinumtoxinA following surgical shave excision has good response rate, high patient satisfaction, high tolerability, minimal adverse sequelae, and low to no recurrence.14,15 Botulinum toxin works by inhibiting connective tissue growth factor expression and decreasing transforming growth factor-β1 in fibroblasts.16–18 In a randomized double-blinded study done by Shaarawy et al., there was a complete absence of reported side effects. 18 The lack of side effects could be attributed to small sample size of 12 female patients. There are very few studies that examined the efficacy and safety of botulinum toxin on keloid treatment and no further studies have been completed with a larger and more diverse population sample.
Currently, there are no studies evaluating the use of surgical shave excision followed by IL corticosteroid and botulinum toxin injections for ear keloid treatment. Due to the lack of evidence, physicians are providing a range of treatment options with limited efficacy and high recurrence rates. The primary objective of this study is to evaluate the effectiveness of the concomitant surgical shave excision with IL TA and onabotulinumtoxinA injections in order to make recommendations for using this treatment combination for the management of ear keloids. The secondary objectives are to evaluate the safety and patient satisfaction of this treatment system.
Patients and materials
Data collection
A retrospective medical chart review was conducted followed by a prospective patient questionnaire. The retrospective review consisted of patients who received treatment of concomitant surgical shave excision followed by IL TA and onabotulinumtoxinA injections for the treatment of ear keloids. All patients received treatment at one outpatient dermatology clinic site. Dosages of TA ranged from 10 mg to 50 mg per treatment, with the most commonly used dosage being 10 mg. Dosages of onabotulinumtoxinA ranged from 2 units to 15 units per treatment, with the most commonly used dosage being 5 units. Clinician determines the ideal dose for each keloid based on size of keloid. The electronic database was used to identify all patients who met the study criteria from 1 January 2015 to 24 February 2021. This was followed by a prospective patient questionnaire in the same patient population. The patient questionnaire was administered via a telephone call during which the patient had the option to provide or deny consent to the prospective questionnaire portion of the study. The site attempted to reach each patient four times. A research ethics board approved the study protocol, patient questionnaire, and questionnaire verbal consent form prior to all study activities. A waiver for consent was obtained for the retrospective nature of the study, with patients included in the photo figures providing additional written consent for the use of these photos for research purposes, and patients who participated in the prospective questionnaire portion of the study providing verbal consent. Patients were not incentivized to receive treatment and both the surgical shave excision and intralesional injections were paid for as cosmetic procedures. Exclusion criteria included patients who received the study treatment for any indication other than ear keloids, patients who did not receive IL TA or onabotulinumtoxinA after surgical shave excision, and patients who did not return to the site after initial treatment. Surgical excision can be performed intralesionally or extralesionally. In this case, surgical shave excision is an extralesional complete removal of the keloid. A carbon steel scalpel blade #15 sterile #3 fitting (Lance) was used to perform multiple repetitive, long, unidirectional, horizontal cuts to remove to the mid-dermis of the keloid. The demographic data of study participants is included in Table 1.
Demographic data for 45 patients with ear keloids treated with surgical shave excision followed by intralesional triamcinolone acetonide and onabotulinumtoxinA.

SD, standard deviation.
Clinical evaluations for early results of effectiveness, chart-reported patient satisfaction, and safety and tolerability of surgical excision followed by IL TA and onabotulinumtoxinA were completed from the retrospective review of chart notes. Prospective patient satisfaction and recurrence rate were completed from the patient questionnaire.
Statistical analysis
Data was analyzed using SPSS version 20.0.0 Software (SPSS Inc, Chicago, Illinois). The outcomes of the categorical variables were summarized as frequencies and percentages for the group of patients. The numerical values, which consisted of follow-up, age and number of IL TA and onabotulinumtoxinA injection treatments were summarized by means, standard deviations, medians, and ranges.
Results
A total of 45 patients were identified as having received surgical shave excision followed by IL TA and onabotulinumtoxinA injections to treat ear keloids after applying the inclusion and exclusion criteria. The patient population consisted of 84.4% females (n = 38) and 15.6% males (n = 7). The mean age at initiation of treatment was 25.5 years (SD ± 7.2), with a median age of 24 years (range 18–59). The size of the keloid was assessed by induration; with keloids 1 cm or shorter being considered small and keloids greater than 1 cm considered as large. The majority of patients had keloids that were classified by the clinician as large in size (71.1%; n = 32); 24.4% of patients had keloids classified as small in size (n = 11), and 4.4% of patients had both small and large keloids present (n = 2). The location of keloids per patient was classified by three criteria: side (left, right, or bilateral), position (anterior or posterior), and ear location (earlobe, helix, or triangular fossa). In this study, 40.0% of patients had keloids located on the left side only (n = 18) and 37.8% on the right side only (n = 17); 22.2% of patients had bilateral keloids (n = 10). The majority of patients had keloids only posteriorly (51.1%; n = 23), with 35.6% both anteriorly and posteriorly (n = 16) and 13.3% with keloids only anteriorly (n = 6). Patients mainly had keloids located on the helix and earlobe (48.9%; n = 22 and 46.7%; n = 21, respectively). Other less common locations consisted of the triangular fossa and both earlobe/helix combined (2.2%; n = 1 each).
All patients received the treatment of surgical shave excision. The mean number of IL TA injection treatments was 2.7 (SD ± 2.2), with a median of 2 treatments (range 1-treatment and a maximum of 12). The mean number of IL onabotulinumtoxinA injection treatments was 2.8 (SD ± 2.3), with a median of 2 treatments (range 1-and a maximum of 12) treatments. The mean follow-up time for was 229.6 days (SD ± 325.3 days), with a median of 92 days (range 28–1673) days. Follow-up time was calculated from the date of surgical shave excision to the last date of contact with the patient as per normal practice, including clinic visits or clinic phone calls. Concomitant therapies consisted of fusidic acid topical ointment (n = 37) and bacitracin-polymyxin B topical ointment (n = 2) for infection prophylaxis following surgical shave excision. Six patients (n = 6) used a silicone-based scar gel (Dermatix® Ultra; Valeant Pharmaceuticals, Laval, Que.) for healing assistance starting 14 days after the initial healing of the surgical shave excision. This was used concomitantly with IL injections. Of these six patients, one also concomitantly used hydrocortisone valerate 0.2% topical and another one concomitantly used hydrocortisone butyrate 0.5% topical since additional healing assistance was determined necessary by the clinician.
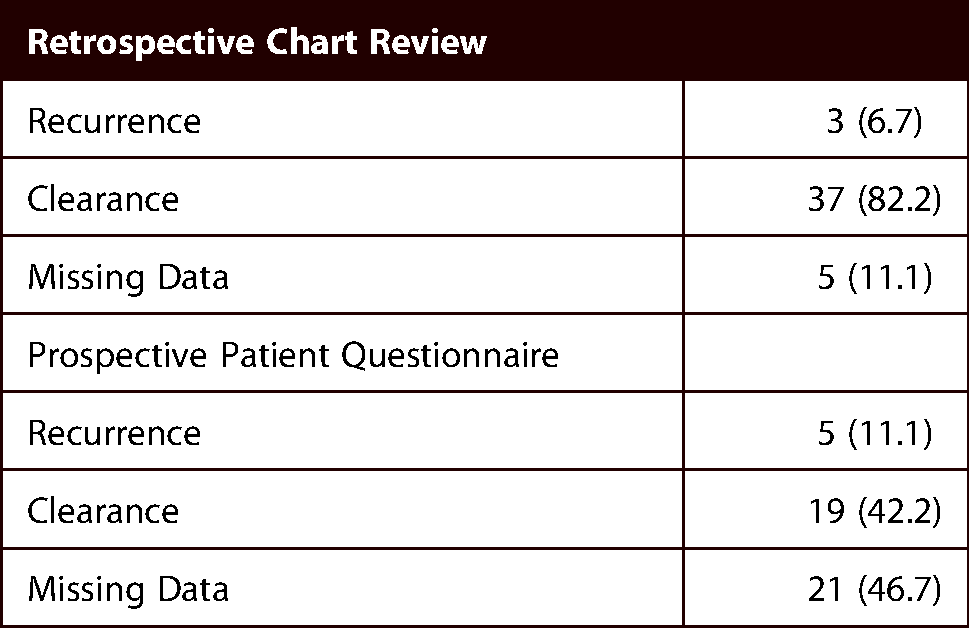
Recurrence was primarily measured through clinician chart notes. No early recurrence was seen in 82.2% of patients at the most recent clinic follow-up (n = 37), though the keloid recurred in 6.7% of patients (n = 3). Response was not noted in the chart notes for 11.1% of patients (n = 5). Additionally, recurrence was also measured via the prospective patient questionnaire, which took place after the most recent clinic follow-up. Here, 42.2% of patients reported that the keloid did not recur (n = 19), and 11.1% reported that the keloid did recur (n = 5). There were 46.7% (n = 21) of patients that did not consent to participate in the prospective questionnaire portion of the study. Early recurrence of the keloid is summarized in Table 2, and the effectiveness and cosmetic results are visually demonstrated in Figures 1–3.

The keloid on the ear treated with surgical shave excision followed by one set of triamcinolone acetonide and onabotulinumtoxinA injections. The length of follow-up time for resolved keloid was 49 days.

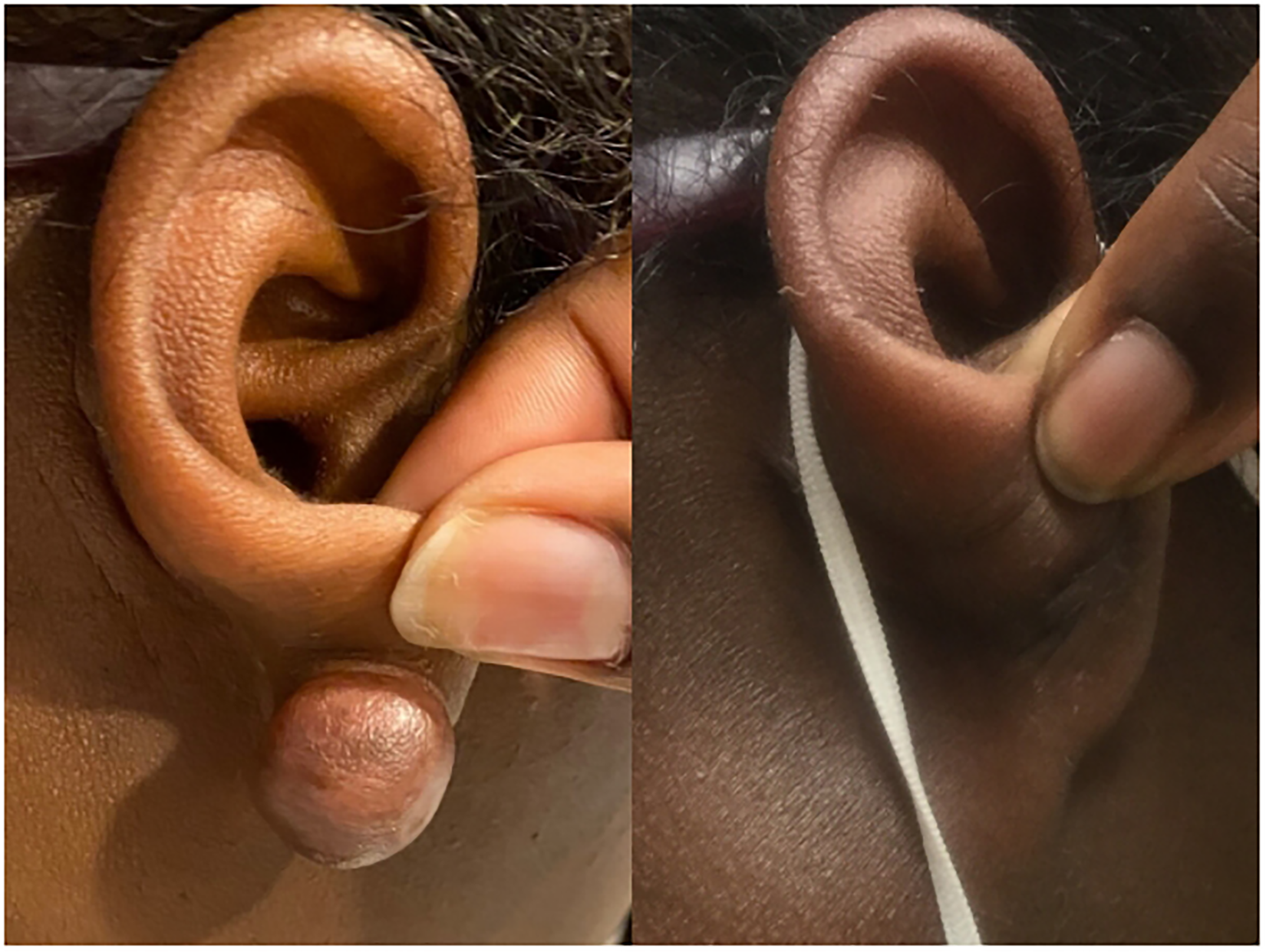
The keloid on the ear treated with surgical shave excision followed by five separate sets of triamcinolone acetonide and onabotulinumtoxinA injections. The length of follow-up time for resolved keloid was 231 days.
The keloid on the ear was treated with surgical shave excision followed by three separate sets of triamcinolone acetonide and onabotulinumtoxinA injections. The length of follow-up time for resolved keloid was 119 days.
Recurrence rates from retrospective chart notes as well as prospective patient questionnaire.
Overall, 20.0% of patients experienced side effects during treatment of surgical excision followed by IL TA and onabotulinumtoxinA injections (n = 9). None of the side effects were classified as serious and all side effects were localized to the location of the excision and/or injection sites. Side effects reported by patients included pruritus (11.1%; n = 5), tenderness (4.4%; n = 2), and sharp pain (2.2%; n = 1). Site effects reported by clinician was mild atrophy (2.2%; n = 1). As per the clinician notes in the patient chart, the sharp pain noted by one patient was due to nerve regeneration. Side effects are summarized in Table 3.
Reported side effects by patients or clinician during or post-treatment with surgical shave excision followed by intralesional triamcinolone acetonide and onabotulinumtoxinA injections.

Patient satisfaction was recorded in the chart notes by the clinician or nurse from verbal reports by patients during clinical visits or phone calls. Patients provided subjective feedback on their satisfaction with no standardized questions, response ranges, or prompting by the clinician. The majority of patients expressed that they were satisfied or very satisfied with the treatment (53.3%; n = 24). One patient (2.2%) expressed that they were dissatisfied with the treatment process; however, this report was made towards the start of IL injections and the full results of the treatment had not yet been determined at that time. The remainder of patients (44.4%; n = 20) did not provide any feedback regarding their level of satisfaction. Therefore, of the patients who reported satisfaction during in-clinic visits, 96.0% (n = 24) patients reporting being satisfied or very satisfied while 4.0% (n = 1) reported being dissatisfied. Patient satisfaction was also measured through the prospective patient questionnaire. Here, the patients were presented with a five-point Likert scale ranging from extremely dissatisfied to extremely satisfied (1 being ‘extremely dissatisfied’ and 5 being ‘extremely satisfied’). There were no reports of patients being extremely dissatisfied, dissatisfied, or neither satisfied nor dissatisfied, whereas 31.1% of patients reported being extremely satisfied (n = 14) and 22.2% reported being satisfied (n = 10). As with the reported early recurrence, 46.7% (n = 21) did not consent to participate in the prospective questionnaire portion of the study. Thus, of those who consented to the patient questionnaire, 100.0% (n = 24) of patients reporting being satisfied or very satisfied (Table 4).
Patient satisfaction from retrospective chart notes as well as prospective patient questionnaire.

Discussion
Keloids are benign, but can significantly impact an individual's quality of life. In addition to being cosmetically and physically troubling for patients, these scars are therapeutically challenging for physicians to treat. In the management of keloids, there are various treatment modalities ranging from surgical to non-surgical methods, including intralesional or extralesional surgical excision, laser therapy corticosteroids, radiation therapy, cryotherapy, silicone cream, 5-FU, and any combination of these treatments.7,19–21 To date, no gold-standard treatment or clear guideline on the appropriate management plan has been published. IL TA with 5-FU is a common dual therapy used for keloid treatment. 22 One randomized-control trial compared IL TA injections against IL TA and 5-FU injections found that the dual therapy had statistically significant keloid height reduction. 22 In addition, the keloid recurrence was much lower at 17.5% for the dual therapy in comparison to 39.2% for IL TA alone. 22 The present study has lower recurrence rates than the combination of IL TA and 5-FU; however, the mean follow-up time was much shorter at 9 months compared to 22 months. 22 A 2018 comparator study observed IL TA and 5-FU offering a balanced benefit of faster and more efficacious result while minimizing side effects; telangiectasia, skin atrophy, and skin ulceration adverse events were experienced at lower frequencies with dual therapy in comparison to either monotherapy. 23 Another common treatment combination is surgical excision with postoperative radiotherapy. This treatment has low recurrence rates of 14.3% with transient pigmentation, erythema, hypopigmentation, and nausea as side effects. 24 A 2016 systematic review compared results from 25 studies for surgical excision followed by TA and surgical excision followed by radiotherapy. 25 The estimated recurrence rate for the excision with TA group was 15.4% and 14.0% for the excision with radiotherapy group. 25 Although radiotherapy as an adjunct is more efficacious, there are more potential complications from radiotherapy as an adjunct. 25 The complications can be severe, such as hyperpigmentation, hypopigmentation, radiation dermatitis, paresthesia, and carcinogenesis. 25 Despite the low recurrence rate, radiotherapy may not be used an adjunct due to its high cost and use of lead. 25 Another study found excision with radiotherapy had a recurrence of 6% and high patient satisfaction, however, the sample size was only 16 keloids. 26 CO2 laser is another treatment option commonly used for keloids. 27 A 2016 study that performed CO2 laser monotherapy for four sessions had mixed results. While showing a significant improvement in the keloid, patient satisfaction was low. 27 In comparison, the present study offers a high level of patient satisfaction while still displaying improvement of the keloid. Another study compared IL TA monotherapy to IL TA in combination with CO2 laser. 28 The combination group displayed a significantly higher percentage of keloids achieving at least 50% improvement in terms of overall appearance, hypertrophy, dyschromia, and texture. 28
Surgical excision can be completed intralesionally or extralesionally. 29 Extralesional, or complete, excision removes the entire keloid with its margin, resulting in a larger scar. 29 Intralesional, or intramarginal, excision removes the central keloid and leaves a narrow margin at the junction between keloid and normal skin. 29 The standard surgical excision method for keloids is extralesional, which leaves the hyperproliferative core intact. 30 This intact core has been known to contribute to increased recurrence rates as the keloidal fibroblasts within the center have lower levels of apoptosis compared to the rest of the keloid. 30 One study supports intralesional excision of keloids due to removing the most proliferative fibroblast portion of the scar, keloidalrim acts as physical restraining splint against tensile forces and avoids injury to deepest layer of the dermis. 30 Additional collagen may be stimulated by the excision of a keloid, resulting in a larger keloid. 31 Intralesional excision has been recommended to prevent additional collagen synthesis. 31 One study showed that leaving a small margin of keloid skin may stimulate keloid recurrence, similar to residues of tumor excision stimulating tumor regrowth. 31 Another retrospective study compared intralesional versus extralesional excision of hypertrophic scars on the lower limbs; the results revealed a statistically significant difference in favor of extralesional method (100% vs. 33% rate of recurrence; P = 0.011). 30 There is insufficient evidence to support intralesional is better than extralesional and that emerging evidence supports extralesional excision; however, rates of recurrence remain high for excision monotherapy. 30
OnabotulinumtoxinA is not FDA or Health Canada approved for keloid management; however, there are many off label applications on scars and keloids. 32 One study directly compared TA and onabotulinumtoxinA injections on keloids after surgical excision; there were no statistically significant difference found, suggesting that onabotulinumtoxinA has comparable results to TA as a primary management agent for short-term reduction in keloid volume, height, redness, and vascularity. 33 However, the study design had a single dose of onabotulinumtoxinA in one treatment arm and repeated TA injections in the control arm. 33 One study found higher patient satisfaction and more favorable pain and itch control when compared to TA injections alone. 18 Thus, the addition and cost of onabotulinumtoxinA to keloid management may be warranted depending on the patient's financial situation, tolerability to side effects, and desired cosmetic outcome.
To our knowledge, this is the first study to look at the multimodal combination of surgical shave excision with IL TA and onabotulinumtoxinA injections for ear keloid treatment. Since this study is the first to include surgical excision, IL TA, and IL onabotulinumtoxinA, we compared our results to studies with different combinations of these three potential treatments. The primary objective of this study was to determine the effectiveness of this treatment modality. Due to the short mean and median follow-up time, the recurrence rates relate to early rather than late keloid recurrence. Our study found that 6.7% (n = 3) of patients had their keloid recur as reported and assessed by the clinician until the most recent clinic follow-up. Of those who consented to answering the optional prospective patient questionnaire, the data showed that 11.1% (n = 5) of patients experienced an early recurrence of their keloid. The mean time between the most recent clinician assessment and the prospective patient questionnaire was 145.5 days (SD ± 85.9), with a median of 114 days (range 75–396). The observed early recurrence rates of 6.7% and 11.1% in the present study (from chart review and prospective survey respectively) is significantly lower than studies of surgical shave excision alone, which had high recurrence rates of 45 to 100%. 5 , 7 For the IL injections, the rates in the present study are at the lower end of the spectrum in comparison to studies using only IL TA and IL botulinum toxin which had recurrence rates of 9 to 50% and 0 to 17% respectively.9,33,34 With the use of combination therapy, the early recurrence rates observed in our study were lower than surgical excision with IL TA injections, which had a reported mean recurrence rate of 15.4%. 25 Presently, one prior study has shown that the combination of surgical excision and IL onabotulinumtoxinA was efficacious for keloid clearance and keloid recurrence, though no recurrence rate was reported. 33 The novel three-pronged treatment approach demonstrated in our study could therefore provide a lower early recurrence rate than other existing combination therapies. However, the lower early recurrence rate could potentially be attributed to missing data in the retrospective chart notes or explained by patients who did not consent or could not be reached for the prospective patient questionnaire.
The present study noted a trend between the initial keloid size and location, as assessed by the clinician, with early keloid recurrence, as reported by the clinician or via the prospective patient questionnaire. Of the keloids that recurred early, as assessed by the clinician (n = 3) and as reported via the prospective patient questionnaire (n = 5), 100% were initially reported as large in size and involved the posterior ear. There were no trends found for the presence of early recurrence and any specific locations of the keloid on the ear (earlobe, helix, or triangular fossa).
The low rate of side effects and the absence of serious side effects are consistent with other studies evaluating safety of keloid treatment with any combination of surgical shave excision, IL TA, and IL onabotulinumtoxinA. The use of IL corticosteroids has been previously associated with atrophy, pigmentation changes, skin necrosis or ulcerations, telangiectasia, and pain.35–37 Presently, only one other study has reviewed surgical excision with IL TA injections; and this study reported no complications or adverse events. 38 Of the listed common side effects, only mild atrophy was observed in one patient in this study. The commonly observed side effects of pruritis, tenderness, and pain in our study could potentially be explained by these three symptoms being primary complaints of patients with keloids. 39 The second most commonly reported side effect of pain is also often commonly described after treatment with surgical excision and IL TA. 38 Furthermore, the low rate of pain reported in the present study may be due to either the addition of onabotulinumtoxinA or the clinic's reporting guidelines for pain during surgical shave excision with IL TA and onabotulinumtoxinA injections. IL onabotulinumtoxinA is known to alleviate pruritis and pain caused by the small-fiber neuropathy typically present in keloids as the onabotulinumtoxinA paralyzes the local muscles and reduces scar muscle tension. 39 In addition, all patients are informed by the clinician prior to the treatment that pain or discomfort is a common side effect experienced with this treatment approach to ear keloids. Only exceptional or sharp pain was reported and recorded within the clinician's notes, although more patients likely experienced some degree of pain during treatment, as noted in another study of surgical excision and IL TA. 38
An additional favorable aspect of the described therapeutic combination is the degree of reported patient satisfaction. More than half of patients, 53.3% (n = 24), expressed satisfaction with the treatment in their chart notes. Of particular interest, it was shown that patient satisfaction reported in the prospective patient questionnaire was also 53.3%, identical to the rate in the chart notes, which was reported a mean 145.5 days prior to the questionnaire. This suggests that the treatment modality in our study has lasting effects on both early recurrence and patient satisfaction. Among patients, 44.4% (n = 20) did not report either satisfaction or dissatisfaction in the chart notes and 46.7% (n = 21) did not consent to the patient questionnaire. When removing the missing data from the sample size and analysis, satisfaction rates for in-clinic and patient questionnaire were 96.0% and 100.0% respectively. The high rate of satisfaction reported in the present study is consistent with rates in studies investigating the use of IL onabotulinumtoxinA and IL TA treatments for ear keloids, which have reported satisfaction rates of 92% and 100% respectively. 18 Most critically, only one patient reported being dissatisfied in either the chart notes or the prospective patient questionnaire. This was reported after the surgical excision, but early in the course of IL injections. It is possible that this patient's level of satisfaction could have changed by the end of treatment course. However, the patient did not provide their level of satisfaction again later in the treatment.
There are certain limitations that arise from the retrospective design of the study. Reported effectiveness was based on subjective chart notes and a prospective patient questionnaire, which could have introduced bias due to any missing data within the charts as well as participation bias and recall bias for the questionnaire. Objective measures of the keloid were not included, such as height, volume, pigmentation, vascularity, and pliability. To increase internal validity, future studies should be conducted using only a prospective study design with objective efficacy, satisfaction, keloid characteristics, and the Vancouver Scar Scale for a direct comparison from baseline to end of follow-up. Due to the short mean and median follow-up times, the results in this study can only comment on short-term effectiveness, short-term relative safety and, short-term low recurrence rates. The amount of IL TA and onabotulinumtoxinA varied from patient to patient and from visit to visit, making it unclear what the ideal dose of each injectable would be. In addition, a few patients used other topical products to assist with healing and scar management, such as a silicone gel, which could have contributed to keloid resolution, recurrence rate, cosmetic outcomes, and correspondingly, patient satisfaction. It is not possible to comment on whether the combination therapy of surgical shave excision with IL TA and onabotulinumtoxinA is a better treatment than other individual or combination treatments since there was no comparator cohort acting as a control in this study. Future studies should use the following seven standardized dose comparator arms: surgical excision alone, IL TA alone, IL onabotulinumtoxinA alone, surgical excision with IL TA, surgical excision with IL onabotulinumtoxinA, IL TA and IL onabotulinumtoxinA, and surgical excision with IL TA and IL onabotulinumtoxinA. A very large sample size would be required to power this future study design due to the number of treatment arms. To increase the external validity of the results, a fully prospective study with the suggested comparators, larger cohorts at multiple treatment sites, standardized dosing schedules, removal of any other scar healing agents, that could contribute to scar management as well as long-term follow-up should be considered. This study shows this treatment modality has promising results; however, further prospective work is warranted to delineate the value of this therapeutic modality in keloid management protocols.
Conclusion
This study demonstrates the early results on the effectiveness of concomitant surgical excision and IL TA and onabotulinumtoxinA injections for ear keloids with a low recurrence rate. The high patient satisfaction, minimal to mild side effects, and great cosmetic results suggest this combination should be considered as a treatment alternative for ear keloids. However, future research involving large-scale studies with comparative designs and long-term follow-up is required to determine the value of this treatment modality for keloid management.
Footnotes
Patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published, and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
How to cite this article
Tran JVH, Lultschik SDJ, Ho JSS, Sapra S, Dong K and Gusic K. Concomitant therapy of surgical shave excision and intralesional injections for ear keloids: Early results from a retrospective cohort study. Scars, Burns & Healing, Volume 8, 2022. DOI: 10.1177/20595131221098531