
Abstract
Background
Keloids are pathological scars characterized by nodular fibrous tissue that extends beyond the border of initial damage. These lesions do not spontaneously regress and can cause cosmetic disfigurements and functional disabilities. IntraLesional Injection of Triamcinolone Acetonide (ILITA), alone or in combination with other therapy, is one of the first-line treatment modalities. In this study the authors evaluated the objective efficacy of ILITA treatment in keloids management using this new imaging system.
Materials and Methods
37 patients with 45 keloid scars were treated with intralesional injection of triamcinolone acetonide (TAC) 20 mg/ml at an interval of three weeks. Antera3D® camera took the images and dates of the treated area in each patient, before the treatment (T0) and at three weeks after the last injection (T1). The system processed the levels of color, elevations, melanin and hemoglobin expression. All the scars were also evaluated, at the same times, by validated Vancouver Scar Scale (VSS). Comparison of the variables was performed using a Wilcoxon signed-rank test with a p < 0.05.
Results
At T0, mean VSS score was 8.67 ± 1.35 which reduced to 3.62 ± 1.72 at final follow up. Antera3D® scores were statistically significant differences in color (8.14 ± 2.41 vs 9.54 ± 1.81), protrusion (381.3 ± 15.6 vs 198.6 ± 21.3), melanin (0.53 ± 0.02 vs 0.62 ± 0.2) and hemoglobin (1.26 ± 0.41 vs 2.21 ± 0.41) expression levels after the treatment.
Conclusions
In our clinical trial, the data results demonstrated that ILITA seems to be effective in reducing keloid dimensions and symptoms such as itching and pain, even if the treatment has local minimal adverse effects such as pain, telangiectasias and atrophy.
Lay Summary
Keloids are pathological scars characterized by nodular fibrous tissue that extends beyond the border of initial damage. Large keloids can cause cosmetic disfigurements and functional disabilities that affect quality of life. In literature, several treatment approaches have been described but, to date, no single method is considered superior. The International Advisory Panel on Scar Management recommended the use of intralesional steroid injections for keloids treatment. The efficacy of treatment may be evaluated with subjective scale; as no one can guarantee an objective evaluation. To eliminate the observer and/or patient factors, and to obtain a reliable, consistent, feasible, valid and objective evaluation a skin analysis camera system called Antera3D® (Miravex, Dublin, Ireland) can be used.
In this study the authors evaluated the objective efficacy of triamcinolone acetonide treatment in keloids management using this imaging system. In this series, for Antera3D® scores there were statistically significant differences in color, protrusion, melanin and hemoglobin expression levels before and after treatment. The device directly shows the treatment changes, measured objectively and accurately, without bias of traditional evaluation scoring scale.
Antera3D® system guarantees an objective evaluation of effectiveness of scar treatment enabling clinicians to modulate the therapy according to the scores registered.
Introduction
Keloids are pathological scars characterized by nodular fibrous tissue that extends beyond the borders of the initial damage. These lesions do not regress spontaneously, but often have a long uninterrupted evolution and growth, and can recur following surgical excision. African, Asian and Latin ethnicities are more affected. 1 The anatomical areas frequently afflicted are the chest, shoulders and earlobes. Symptoms that can occur include pain, itching, dysesthesia, and restricted movements. Large keloids can cause cosmetic disfigurements and functional disabilities that impact the quality of life (Figure 1). 1

Large earlobe keloid of man after minimal trauma.
Histological examination of keloid scars shows dense fibroblasts and bundles of collagen2,3; the massive extracellular matrix deposition and fibroblasts proliferation (with lower apoptotic rate) result from the lack of control mechanisms during the “remodeling phase” of wound healing.3,4 However, the complete pathological mechanism has not been elucidated.3–5 Recent research indicates that the formation and growth of keloids are clearly associated with genetic, epigenetic, systemic and local risk factors. 6
In literature, several treatment approaches have been described but, to date, no single method is considered superior. There are many options available: occlusive dressings, compression, silicone sheets, intralesional injection of steroid or other drugs (verapamil, 5FU, interferon), cryotherapy, surgical excision, pulsed dye laser, radiotherapy, imiquimod cream and Adipose Derived Stem Cells (ADSCs).7–12 Non-surgical approach is recommended for primary treatment, because keloids have a high recurrence rate after surgical excision. The International Advisory Panel on Scar Management recommended the use of intralesional steroid injections for keloids treatment. IntraLesional Injection of Triamcinolone Acetonide (that we called ILITA treatment), alone or in combination with other therapy, is one of the first-line treatment modalities.7,9,13–20 The efficacy of triamcinolone acetonide in keloids treatment has been demonstrated in various clinical trials since 1960, with efficacy rate from 50 to 100%, and recurrence rate of 50% in five years.18–21
Corticosteroids reduce collagen synthesis, inhibit rapid growth of fibroblasts (antimitotic effect), promote vasoconstriction (reducing the delivery of oxygen and nutrients to the wound bed) and control local inflammation (inhibiting leukocyte and monocyte migration and phagocytosis). Furthermore, they reduce protease inhibitors, alpha1antitrypsine, alpha2macroglobuline, TGF-beta, IGF1 and VEGF. 22
Triamcinolone acetonide is used in different concentrations (ranging from 10 to 40 mg/ml), frequency (the interval between successive injections ranges from one to four weeks), and length of treatment (number of injections may vary from four to eight).7,18,19,21
ILITA therapy may induce adverse effects such as telangiectasias, atrophy, hypo/hyper-pigmentation, ulcers, necrosis, and Cushing's syndrome.13–20
The efficacy of treatment may be evaluated with subjective scales. In literature we identified 10 different scales: Vancouver Scar Scale (VSS), Dermatology Life Quality Index (DLQI), Manchester Scar Scale (MSS), Patient and Observer Scar Assessment Scale (PSAS/OSAS), Bock Quality of Life questionnaire (Bock QoL), Stony Brook Scar Evaluation Scale (SBSES), Patient-Reported Impact of Scars Measure (PRISM), Patient Scar Assessment Questionnaire (PSAQ), University of North Carolina “4P” Scar Scale (UNC4P) (Table 1). 23 However, these scales do not guarantee an objective assessment because they are influenced by observer and/or patient factors. To obtain a reliable, consistent, feasible, valid and objective evaluation, we propose the use of a new skin analysis camera system called Antera3D® (Miravex, Dublin, Ireland). This 3D camera, using a light emitting diodes and a complex software, evaluates skin objective indicators (measuring dimensions, texture, and colors) and reconstructs 3D images.
Rating scales for scar assessment.

In this study the authors evaluated the objective efficacy of ILITA treatment in keloids management using Antera3D® imaging system. To our knowledge, in literature there are no studies comparing the Antera3D® measurements with other methods for keloid evaluation such as VVS or P/OSAS. Our study is the first report of this comparison.
Materials and methods
This open clinical trial was carried out on 37 patients at the Department of Plastic Surgery of OORR Ospedali Riuniti –University of Foggia (Italy) from January 2018 to July 2019.
Inclusion criteria were: keloid scar never treated before, age>18 years. Exclusion criteria were: age<18 years, immunodepression, pregnancy, lactation, diabetes, local/general infection, previous or additional scar treatment, connective tissue disorders, hypersensitivity to lidocaine.
The study conformed to good clinical practice guidelines and followed the recommendations of the Declaration of Helsinki. The local Ethics Committee Comitato Etico (CE) of Azienda Ospedaliero-Universitaria “Ospedali Riuniti” di Foggia approved the protocol; every patient signed the informed consent of the treatment procedures and the adverse effects.
The authors treated a total of 37 patients with 45 keloid scars with intralesional injection of TAC 20 mg/ml at an interval of three weeks for a total of four sittings.
The investigators used an Antera3D® camera to take the images and dates of the treated area in each patient, before the treatment (T0) and at three weeks after the last injection (84 days from the first injection, T1). The Antera3D® system processed the levels of color, elevations, melanin and hemoglobin expression (Figures 2 and 3). All the scars were also evaluated, at the same time, by validated Vancouver Scar Scale (VSS) that assesses four variables: vascularity, thickness, pliability, and pigmentation.

Antera 3D® analysis of keloid developed after a skin infection (pimple); (a) dimensions; (b) protrusion; (c) melanin; (d) hemoglobin.
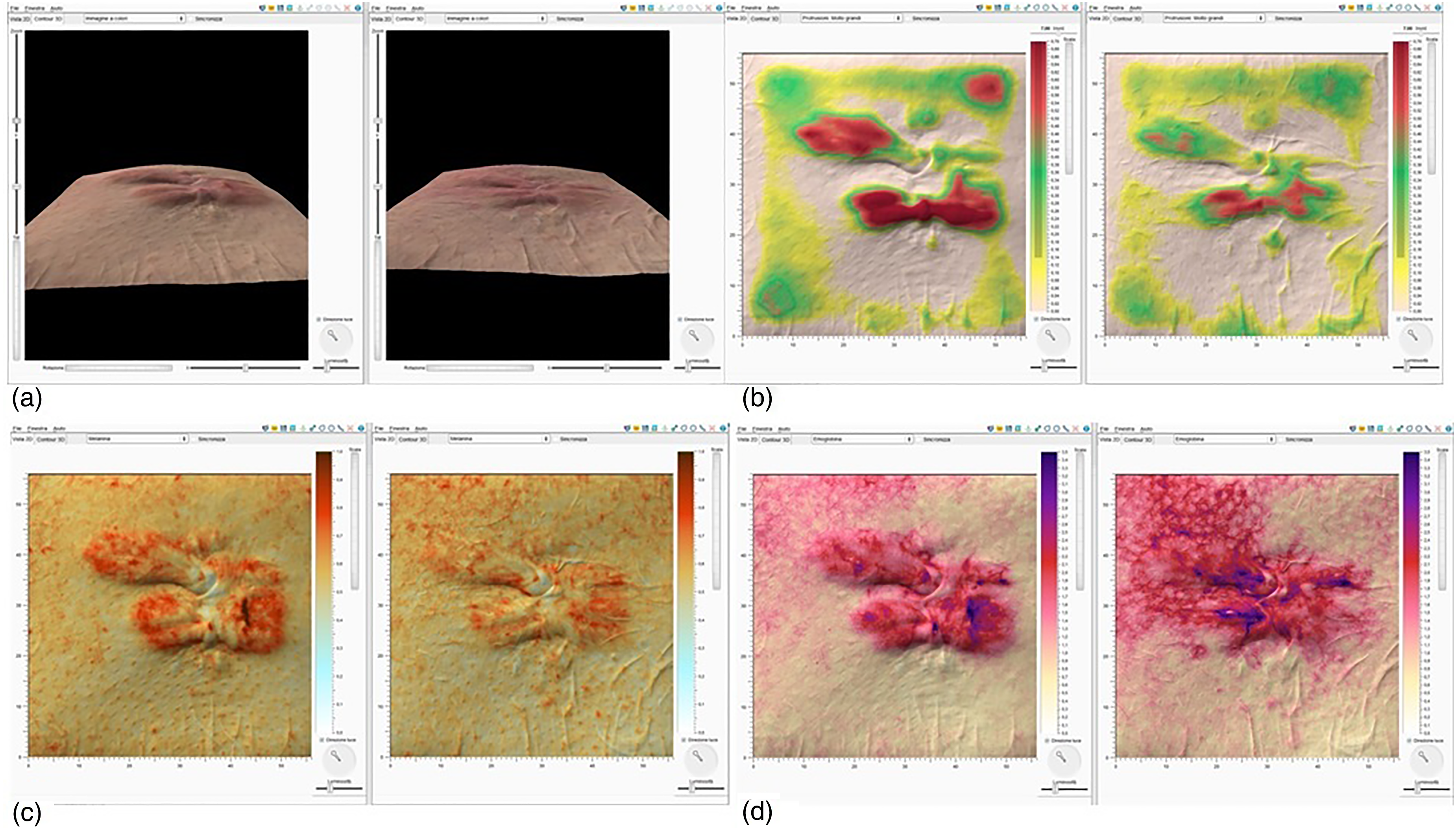
Antera 3D® analysis of keloid pre- and post-treatment (a) dimensions; (b) protrusion; (c) melanin; (d) hemoglobin.
During the study every consideration and adverse effects were signaled. Patients were followed-up with from 84 to a max of 168 days after first treatment. The study was planned as a case-series study to objectively evaluate the efficacy of TAC with respect to scar outcome using the Antera3D® system.
We present summary statistics as means with standard deviation (Std) and medians with a range for continuous variables. Comparison of the categorical variables pre- and post-treatment was performed using a Wilcoxon signed-rank test An expert bio-statistician performed the statistical analysis using Statistical Package for Social Sciences (SPSS version 16.0). A p value of less than 0.05 was considered statistically significant.
Results
A total of 37 patients were treated with ILITA 20 mg/ml. All completed the sessions, and there were no dropouts. There were 27 (73%) male participants and 10 (27%) female, and the mean age was 29.3 ± 10.4 years (range 18–47). 31 patients (83.8%) had one keloid; six (16.2%) had two or more keloids, with a total of 45 keloids treated. Duration of keloid ranged from one to 36 months with a median of four months.
Scar locations were: chest 27 (60%), shoulder 11 (24.4%), ear 4 (9%), neck 2 (4.4%), thigh/leg 1 (2.2%). See Table 2.
Epidemiological characteristics of keloids.

An assessment of VSS score was carried out at the baseline (T0, before the treatment) and at three weeks after the last injection (T1, at 12 weeks after the first treatment).
At T0, mean VSS score was 8.67 ± 1.35 (median 8.0) which decreased to 3.62 ± 1.72 (median 3.0) at the final follow up, showing a mean change of −5.05 ± 1.41. On evaluating the data, it was found to be statistically significant (z is 4.325; p-value = 0.025). See Table 3.
VSS scores before and after treatment.

Patients reported these adverse effects: pain in 13 cases (35.1%), telangiectasia in three cases (8.1%), atrophy/hypopigmentation in two (5.4%).
The Antera3D® score (see Table 4):
For COLOR after four sessions of ILITA were 8.14 ± 2.41, which were significantly lower than before the treatment (9.54 ± 1.81, z = 3.216, p-value <0.05). For LARGE ELEVATIONS after four sessions of ILITA were 198.6 ± 21.3, which were significantly lower than before the treatment (381.3 ± 15.6, z = 2.635, p-value <0.05). For MELANIN after four sessions of ILITA were 0.53 ± 0.02, which were significantly lower than before the treatment (0.62 ± 0.2, z = 2.4, p-value <0.05). For HEMOGLOBIN after four sessions of ILITA were 1.26 ± 0.41, which were significantly lower than before the treatment (2.21 ± 0.41, z = 2.09, p-value <0.05).
Antera3D scores before and after treatment.

Discussion
Nowadays, there is no gold standard treatment for keloids. Combined therapies are more successful than one alone: in fact, ILITA, alone or in combination with other drugs (5-FU, verapamil, bleomycin), radiation therapy or laser or after surgical excision, is an optimal non-surgical approach. It reduces scar dimensions and symptoms such as pain and itching, and it prevents recurrence.7,10,13–22 The action mechanism is multiple: reducing collagen and Glycosaminoglycans (GAGs) synthesis, inhibiting fibroblast growth, enhancing fibroblast degeneration, and having anti-inflammatory effects. 22
The evaluation of therapeutic effectiveness on scars is often made with subjective evaluation (patient/surgeon) using clinic scales (i.e., VSS, DLQI, MSS, P/OSAS, UNC4P, etc.). These scales are simple but no single one had been shown to be reliable, consistent, feasible, and valid at the same time because they are subjective to bias, lack of objectivity and repeatability of measure. So, an objective and independent assessment is needed. Antera3D® is a validated new tool for the objective evaluation of skin characteristics and, therefore, of the scars.
It is a new device, developed in the Department of Physics of Trinity College in Dublin, which contains a camera for image acquisition of 56*56 mm (3136 mm2) and a computer with a software for analysis of the acquired image data. This novel 3D camera system collects the reflections after irradiation of the skin with a multi-spectrum light emitted from different directions by seven different wavelengths LED (light-emitting diodes).
With the spatial and spectral analysis of the different reflections and optical penetration lengths of different waves, a digital processing of the lights signals reconstructs the skin surface in two and three dimensions and allows evaluation of the skin topography and the chromophores’ concentration. Therefore, it can be used to evaluate skin color, texture, pore, depression wrinkle, elevation, melanin, hemoglobin and lesions.24,25 The reconstruction of the skin texture is achieved using a technique based on Shape from Shading (SFS), modified to improve accuracy and to eliminate skin glare. Moreover, the device uses seven different wavelengths of LED light (entire visible spectrum) to acquire the reflectance data which are transformed into skin absorption coefficients and used to quantify melanin and hemoglobin concentrations, using mathematical correlation with known spectral absorption data of these chromophores.26,27 The skin surface shape is used to compensate for light intensity variation due to the varying direction of incident light.
The images acquired are independent of lighting conditions, using a combination of polarizing filters and a software, which guarantees reproducible conditions and accuracy of the results.
The analysis of melanin and hemoglobin are important for more skin lesions, such as benign and malign cancers, precancerosis, rosacea, vitiligo, port wine stains, melasma, scars, etc.
In particular, the measurement of melanin and hemoglobin concentrations is relevant in analyzing the properties of keloid scars because: hemoglobin is contained in blood vessels of papillary dermis that are hyperexpressed in these pathologic scars, because of neoangiogenesis and local inflammation5,28; and because melanin, produced by melanocytes, has a duplex rule in keloid formation. In fact, it causes a decreasing of histological pH which inhibits collagenase that disrupts collagen degradation process; moreover, during wound healing, melanocytes from the stratum basal interact with dermal fibroblast facilitating fibroblast proliferation and secretion/deposition of collagen.29,30
So, the reduction of melanin and hemoglobin concentrations after the treatment is indicative of the improvement of the clinical status of scar and of the efficacy of therapy.
Antera3D® is a great support to the diagnostic evaluation for the following reasons:
It is an objective method because it responds to sophisticated mathematical software for spectrometric conversion of the light and converts all possible skin parameters, except for the tactile property, into numbers; there is no subjective bias of evaluation with clinic scales. It allows comparison pre- and post-therapeutic treatment images. It is an operator-independent system. It is possible to catch the image at a specific capture rate (preferable > 98%); if there are problems relating to the centering of the image, a specific function helps to correct any possible error. It is possible to repeat the analysis any time and without limitation. It is safe and intuitive (very short learning curve is necessary).
In our series, for Antera3D® scores there were statistically significant differences in color, protrusion, melanin and hemoglobin expression levels, before and after treatment with triamcinolone acetonide. The device directly shows the treatment changes, measured objectively and accurately, without bias of traditional evaluation scoring scales.
Thanks to the three-dimensional multispectral analysis performed with Antera 3D®, data of this study revealed an improvement of the aesthetic-functional outcomes in a clearer and more objective way.
Moreover, this type of analysis would allow the clinician to modify the treatment plan according to the changes of these indexes after the therapy, obtaining a better result.
The limitation in our study is its small simple size; in fact, though Antera3D® is able to define a standard treatment/therapeutic success through specific parameters and scores, its major limit is the need for several clinical cases to reach standardization. Therefore, further research using Antera3D® is needed; we are consequently collecting and analyzing other data in order to expand this clinical trial in future and produce a stronger study.
Furthermore, our participants were followed-up with for maximum of 168 days after the first treatment, but as keloids tend to relapse, an extended follow-up is needed.
Conclusions
In our clinical trial, the data results demonstrated that ILITA seems to be effective in reducing keloid dimensions and symptoms such as itching and pain, even if the treatment has local minimal adverse effects such as pain, telangiectasias and atrophy.
This camera analysis system guarantees an objective evaluation of scar treatment effectiveness; so clinicians can modify the therapy according to the scores registered. It is worth promoting widely because it is easy to use, safe, objective, repeatable, with low cost, and helpful to measure in clinical studies the efficacy of treatment, even with a long follow-up.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
How to cite this article
Lembo F, Cecchino LR, Parisi D and Portincasa A. The objective evaluation of triamcinolone acetonide efficacy in keloids management using Antera3D® imaging system. Scars, Burns & Healing, Volume 8, 2022. DOI: 10.1177/20595131221137768.