
Abstract
Introduction
The extracellular matrix (ECM) plays an integral role in wound healing. It provides both structure and growth factors that allow for the organised cell proliferation. Large or complex tissue defects may compromise host ECM, creating an environment that is unfavourable for the recovery of anatomical function and appearance. Acellular dermal matrices (ADMs) have been developed from a variety of sources, including human (HADM), porcine (PADM) and bovine (BADM), with multiple different processing protocols. The objective of this report is to provide an overview of current literature assessing the clinical utility of ADMs across a broad spectrum of applications.
Methods
PubMed, MEDLINE, EMBASE, Scopus, Cochrane and Web of Science were searched using keywords ‘acellular dermal matrix’, ‘acellular dermal matrices’ and brand names for commercially available ADMs. Our search was limited to English language articles published from 1999 to 2020 and focused on clinical data.
Results
A total of 2443 records underwent screening. After removing non-clinical studies and correspondence, 222 were assessed for eligibility. Of these, 170 were included in our synthesis of the literature. While the earliest ADMs were used in severe burn injuries, usage has expanded to a number of surgical subspecialties and procedures, including orthopaedic surgery (e.g. tendon and ligament reconstructions), otolaryngology, oral surgery (e.g. treating gingival recession), abdominal wall surgery (e.g. hernia repair), plastic surgery (e.g. breast reconstruction and penile augmentation), and chronic wounds (e.g. diabetic ulcers).
Conclusion
Our understanding of ADM’s clinical utility continues to evolve. More research is needed to determine which ADM has the best outcomes for each clinical scenario.
Lay Summary
Large or complex wounds present unique reconstructive and healing challenges. In normal healing, the extracellular matrix (ECM) provides both structural and growth factors that allow tissue to regenerate in an organised fashion to close the wound. In difficult or large soft-tissue defects, however, the ECM is often compromised. Acellular dermal matrix (ADM) products have been developed to mimic the benefits of host ECM, allowing for improved outcomes in a variety of clinical scenarios. This review summarises the current clinical evidence regarding commercially available ADMs in a wide variety of clinical contexts.
Keywords
Introduction
Historically, large and/or complex soft-tissue defects have been treated with techniques including full and split-thickness skin grafts (FTSG and STSG), local flap coverage and free tissue transfer. Each of these has disadvantages such as donor site morbidity, risk of flap/graft complications or even failure. 1 In some cases, such as excessive wound depth or specialised function of tissue needing repair, patient and/or wound characteristics may preclude the use of traditional techniques for soft-tissue coverage. 1
Successful wound healing depends largely on the interactions of proliferating cells with the extracellular matrix (ECM) in a process known as dynamic reciprocity. 2 The ECM—composed of proteoglycans, hyaluronic acid, collagen and elastin—directs tissue regeneration and differentiation via mechanical cues and signalling molecules. 2 In traumatic or chronic wounds, the ECM is often damaged to the extent that it no longer adequately supports healing. Acellular dermal matrices (ADMs) were developed in an attempt to capitalise on the properties of native ECM and promote organised regeneration of host tissue in a wide variety of clinical contexts. 2
When ADMs are placed, host cells are incorporated into the matrix and directed by preserved growth factors and mechanical cues in the matrix structure.2,3 A variety of cells invade the ADM, including fibroblasts, myofibroblasts, lymphocytes, macrophages, granulocytes, mast cells and others.3,4 After inflammatory cell infiltration, the matrix undergoes remodelling, collagen and elastin levels increase, and revascularisation is initiated.3,5–7 Lymphangiogenesis is possible, but is slower. 3 Essentially, the ADM acts as a scaffold to promote host tissue growth. 1
ADMs were initially used to treat burn wounds in the 1990s and have since become a valuable addition to reconstructive algorithms as they are available off the shelf and have superior biocompatibility compared to synthetic soft-tissue grafts.8,9 All ADMs are decellularised and antigenic components have been removed to prevent immune rejection 4 (Figure 1).

Schematic representation of ADM preparation. ADM, acellular dermal matrix.
Given the success of early ADM applications, interest has evolved to include a variety of procedures spanning multiple surgical subspecialties. 10 Over the past two decades, a number of commercially available ADMs have been developed that vary both in origin of tissue and level of processing (Table 1, Figure 2). 11 Human cadaver (HADM), bovine (BADM) and porcine (PADM) tissues have been used in a variety of different clinical contexts, with results differing by product and application. 11 Products are further distinguished by tissue type (Figure 2), additives (e.g. antibiotics or surfactants) and preparation regulations. 12 In this article, we review the current literature assessing the clinical utility of ADM across a broad spectrum of applications.
Diagrams showing common sources of ADM tissue. Yellow highlighted portions represent the area harvested for processing. ADM, acellular dermal matrix.
Common commercially available ADMs.

ADM, acellular dermal matrix.
Methods
The authors performed a review of the PubMed, MEDLINE, EMBASE, Scopus, Cochrane and Web of Science databases using keywords ‘acellular dermal matrix’, ‘acellular dermal matrices’ and brand names for commercially available ADMs shown in Table 1. Articles were screened by title and abstract, then by full text for inclusion. Our search was limited to English language articles (or those with available English translations) published from January 1999 to September 2020. This review is focused on recent clinical data with special attention to studies comparing different ADMS.
Summary findings of included studies are presented in tables divided by clinical context (Tables 2–9). Within each table, articles are grouped by level of evidence (e.g. case report/series, retrospective study, prospective study, meta-analysis).
Clinical evidence for ADMs in burn wounds.

ADM, acellular dermal matrix; BADM, bovine acellular dermal matrix; CI, confidence interval; HADM, human acellular dermal matrix; mVSS, modified Vancouver Scar Scale; PADM, porcine acellular dermal matrix; STSG, split-thickness skin graft; TBSA, total body surface area; TNP, topical negative pressure; VSS, Vancouver Scar Scale.
Results
After duplicates were removed, there were 2443 records identified that underwent screening. After screening, 170 articles were included in our synthesis of the literature. A total of 19 articles were included in Burn, 18 in Wound Care, 30 in Breast Reconstruction, 9 in Andrology, 11 in Gynecology and Gynecological Oncology, 26 in Orthopaedic Surgery, 18 in Oral and Maxillofacial Surgery, 9 in Craniofacial Surgery, 16 in Abdominal Wall / Hernia and 7 in Otolaryngology/Ear, Nose, and Throat (ENT).
Plastic and reconstructive surgery—burn
ADMs have been used as an adjunct for tissue modification and enhancement following severe burns (Table 2).13–16 ADM application to self-assembled skin substitute (SASS) has been shown to increase cell proliferation, preserve intrinsic properties and reduce likelihood of rejection. 13
Researchers have manipulated the biological signalling pathway via either direct application of signalling cells to an ADM or by combining a deep-degree burned dermal matrix (DDBDM) harvested from the host with an ADM.14,17 ADMs impregnated with signalling cells or DDBDMs had higher probability of maintaining integrity, histocompatibility and stability. 14
Integra™ (BADM) is the most commonly used ADM for treating severe burns.18,19 In a large, multicentre study, Integra™ showed improvements in hypertrophic scarring compared to controls. 20 While subsequent studies have confirmed its efficacy in improving appearance, elasticity and functional outcomes, 21 infection rates remain a concern.22,23 The use of antimicrobial dressings and/or negative pressure wound therapy (NPWT) in conjunction with Integra™ has led to improved infection rates.19,24 Recently, MatriDerm (BADM) has been used in pediatric 25 and adult populations26–28 to treat burns via a single staged procedure. 19 Compared to Integra™, MatriDerm has demonstrated increased neovascularisation and higher degradation rates. 19 The concurrent use of NPWT with MatriDerm has improved clinical outcomes. 18 While early clinical data on MatriDerm are promising, the literature lacks direct clinical comparisons of MatriDerm and Integra™. 18
One case study described HADM application to infant calvarial burns involving the brain. 29 Recommended treatments typically involve high speed drilling for massive calvarial exposure or coverage with adjacent vascularised scalp tissue,30,31 but these techniques prove challenging with immature cranial development. However, in this case, HADM (AlloDerm) was used to reconstruct a large dural defect and calvarial burn, which successfully prevented cerebrospinal fluid leakage, facilitating dural reconstruction and efficient revascularisation of tissues. 29 Candida parapsilosis, a common exogenous yeast that resides in burn wounds, has been observed proliferating on HADM (Pelnac®) after seven days of incubation as well as penetrating and crossing the ADM within three days. 16
While existing literature is limited, PADM has been used in treating burn wounds due to its ability to support proliferation and enhanced epidermal cell attachment given the partial conservation of basement membra. Dermabrasion used in conjunction with PADM resulted in wound healing duration of 22.5 days, whereas those treated conservatively without PADM required 30.3 days. 15 Limited use of PADM in this context may be attributed to high cost and/or concern for transmitting infection from source tissue. 19
Wound care
Lower limb skin and tissue are extremely thin, especially from the foot and ankle, which poses a challenge for obtaining wound closure (Table 3). Reverse sural adipofascial flaps (RSAF) are commonly used to achieve coverage, but when used in conjunction with STSG, healing is prolonged.32,33 One report detailed a method of RSAF application in which ADM was successfully (25% faster healing) used in concert with NPWT. 34 ADMs may be a useful adjunct to RSAF as they increase tissue vascularisation and support early fibroblast and endothelial cell growth.22,35 A retrospective study of eight patients with foot and ankle wounds reported healing in an average of 104.5 days when treated with ADM and NPWT before STSG and RSAF compared to 141.2 days with STSG and RSAF alone. 34 Other reports have shown that patients treated conservatively (nano-silver dressing alone) or with dermabrasion + nano-silver dressing had a longer average hospital stay than those treated with dermabrasion + PADM. 15
Clinical evidence for ADMs in wound care and ulcers.

ADM, acellular dermal matrix; BADM, bovine acellular dermal matrix; CEAP, clinical aetiology anatomy pathophysiology; DFU, diabetic foot ulcer; FBADM, fetal bovine acellular dermal matrix; HADM, human acellular dermal matrix; NPWT, negative pressure wound therapy; RSAF, reverse sural adipofascial flap; STSG, split-thickness skin graft; TBSA, total body surface area; VLU, venous leg ulcer.
ADM application for upper-limb wounds has resulted in improved elasticity and range of motion (ROM) compared to wounds treated with skin graft alone. 36 Axillary and cubital joint dermis wounds are associated with high rates of contracture and severe scarring. 37 However, with ADM application, one retrospective study of 89 patients reported patient satisfaction with pain relief, ROM and aesthetic outcome in 82%, and 75% had good-excellent physician-reported functionality and ROM. 38
ADMs are particularly useful when treating exposed tendons and bones that may be unsuitable for skin graft coverage.37,39 In radial forearm flap donor site closure, ADM application has led to minimal scar contracture and complications, as well as normal ROM, grip and pinch.37,40,41 In tumour resection surgery, skin contracture is a common complication; however, application of ADM rather than skin grafts alone has improved final ROM. 42
Skin grafting can be difficult in lower-limb wounds as limited available tissue may lead to dermal tension. However, one study of 30 lower-limb injuries treated with combination ADM and STSG reported successful grafting in 29 wounds and an average of 56.4 days to complete healing. 43 Success in these patients may be attributed to ADM’s ability to maintain elasticity and tensile strength while promoting vascularisation and preventing infection.
ADMs have shown efficacy as an adjunct in lower limb ulcers treatment.2,44–46 One randomised controlled trial showed that HADM resulted in greater reduction in wound size at 24 weeks (59.6% HADM vs. 8.1% control). 44 In the same study, 100% of HADM-treated wounds remained closed at four weeks postoperatively and 75% remained closed at 12 weeks compared to 66.7% at four weeks and 33.3% at 12 weeks in the control group. 44 Fetal BADM has been used in treatments for diabetic foot ulcers (DFUs) and venous leg ulcers (VLUs).45,46 BADM has improved DFU healing outcomes by 40% and led to a wound closure of 76% in 53.1 ± 21.9 days in one cohort. 45 In VLUs, BADM application resulted in a median reduction of 23.5% in the wound area at four weeks postoperatively. 46 When compared to advanced moist wound therapy (AMWT), such as foams and gels, HADM application in DFUs resulted in complete closure in 69.6% compared to 46.2% with AMWT. 2
In addition to wound closure, ADMs have been shown to improve the aesthetic properties of skin. In burn scars, HADM has been used to achieve significant improvement of burn scar quality as measured by the Vancouver Scar Scale. 47
ADMs have been associated with complications, including the following: hypopigmentation; lack of vascularisation and lymphatics; absence of hair follicles, sweat and sebaceous glands; and incomplete innervation. 17 Increased duration of treatments raises costs associated with ADMs.2,45,48,49 When incorporating BADM into DFU treatment, 42.9% of patients needed multiple applications with an average wait of 23 days between appplications. 45 ADM + STSG treatment is a staged process in which STSG is performed 3–4 weeks after ADM application. 34 When incorporating ADM in wound treatment algorithms, the effects of treatment duration should be considered.
Breast reconstruction
ADMs have become a popular adjunct to enhance wound healing, organised tissue regeneration and cosmesis in breast reconstruction and augmentation (Table 4).2,50,51 While individual reports vary, aggregate data indicate that complications are rare.52–57 A systematic review of 1039 breast reconstructions with either PADM or HADM showed low overall rates of skin and nipple necrosis (11% and 5%, respectively), infection (12%), hematoma (1%) and seroma (5%), with only 9% of patients requiring reoperation. 52 This success may be attributed to ADMs’ ability to fully integrate into host tissue with neovascularisation, cell repopulation and lack of inflammatory cells observed at both short- and long-term follow-up.56,58
Clinical evidence for ADMs in breast reconstruction.
ADM, acellular dermal matrix; BADM, bovine acellular dermal matrix; BMI, body mass index; FBADM, fetal bovine acellular dermal matrix; HADM, human acellular dermal matrix; JP, Jackson Pratt; OR, odds ratio; PADM, porcine acellular dermal matrix.
ADMs have been applied to revision augmentations, as they adequately reinforce the soft tissue and implant pocket, thereby decreasing rates of capsular contracture.53–55 A retrospective review of 850 breast reconstructions reported that out of 450 breast reconstructions using PADM, there was a total complication rate of 33.2%: 12.2% developed seromas; 5.2% major infections; and 6.5% minor infectons. 59 One study of 3189 breast reconstructions noted that if antibiotics were administered for <24 h after operation, the infection rate was 2.48%, whereas regimens that lasted >24 h had an infection rate of 13.21%. 60 In a prospective study of 27 patients, ultrasound detected lymphoceles in only three patients; one patient experienced infection, and all three cases of seroma resolved by 12 months. 61
A 13-year cumulative study of 1584 breast reconstructions with ADM reported capsular contracture of 0.8% in the entire cohort and 1.9% in irradiated breasts. 53 A separate study of 455 breasts revealed minimal contracture 21 months after breast reconstruction surgery. 54 By facilitating an optimal breast pocket, ADMs help to obtain symmetrical coverage, enhance the aesthetic outcome, decrease pain from pectoralis muscle mobilisation and reduce scarring.57,62 Limited capsule contracture and scarring may also be attributed to the decreased inflammatory response associated with ADMs.63,64 Additionally, it is more difficult for scar tissue or capsules to develop on the ADM surface. Once revascularised, the ADM-treated tissue will exhibit improvements, such as enhanced elasticity, that minimise contracture. 65
One case study described the use of ADM to rescue a non-ADM reconstructed breast from complications. 66 A patient undergoing radiotherapy after breast reconstruction developed a radiation ulcer, and by utilising PADM with Becker’s 50 expander as reinforcement, the breast and ulcer were resolved. 66
While ADM appears more costly in the short term ($6686 ADM vs. $5615 non-ADM), ADM has been associated with lower total cost at two years postoperatively ($11,862 vs. $12,319). 67 ADM integration with fenestrations and perforations led to decreased risk of infection, duration of tissue draining and length of hospital stay. 68
Thick ADM implants (≥1.2 mm), compared to thin ADM implants, have been linked to increased rates of necrosis (+3.5%), seroma (+3.5%), infection (+8.8%) and need for drainage two weeks postoperatively (+15%).60,69 This may be the result of reduced neovascularisation in thicker ADMs. 69 One study showed that implants <400 mL were 10.3 times more likely to experience capsular contracture. 53
Implants from different manufacturers (with different processing protocols) may produce different outcomes. In two comparative studies of HADMs, FlexHD resulted in more complications than AlloDerm and Cortiva.70,71 In studies directly comparing ADMs of different origins, results indicate that BADM may be more suitable for breast reconstruction compared to HADM and PADM.12,71–73
Patient lifestyle factors are known to affect outcomes in ADM procedures.53,58,69,74,75 Smoking status, chemotherapy or radiation, and diabetes mellitus have been associated with increased risk for seroma, cellulitis, wound infection and implant failure.53,58,69,74,75 Body mass index (BMI) has been identified as a predictor of tissue drainage time. 69
Surgeon expertise appears to influence outcomes of ADM procedures.70,76,77 Multiple factors must be carefully considered when performing ADM breast procedures, including the following: pectoralis muscle anatomy; flap conditions; skin excess; sentinel-node status; flap vascularity; BMI; and the type of tumour, if present. 78
Andrology
Following application in breast reconstructions, ADM usage evolved to include penile augmentations, erectile dysfunction (ED) treatments and phalloplasties (Table 5).79,80 Advantages of ADM include lower risk of necrosis, shorter operation time and more subtle incisions.79–81
Clinical evidence for ADM in andrology.

ADM, acellular dermal matrix; IELT, intravaginal ejaculation latency time; PADM, porcine acellular dermal matrix; XADM, xenographic acellular dermal matrix.
One study of 69 patients described a technique in which PADM was placed circumferentially from the groove between cavernous and spongious bodies on one side to the other and secured to Bucks fascia. 79 One year postoperatively, penile circumference increased 3.1 cm while flaccid and 2.4 cm while erect. 79 A retrospective study of 78 patients who received ADM administrations as filler material also showed increased measurements (mean + 1.1 cm). 82 A pilot study assessing an acellular collagen matrix reported results varying by ADM insertion method, with a bilayer inserted through V-Y suprapubic incision producing greater circumference increases and patient satisfaction. 83
ADMs may contribute to improved erectile function and reduced premature ejaculation in penile augmentation patients.81,84 One study followed 39 patients seeking treatment for ED, and after six months, flaccid girth increased >1 cm, erect girth by >2 cm and intravaginal ejaculatory latency time increased by 200 s on average. 84
PADM has been used as an adjunct in Fournier gangrene treatment. 85 In one study, average wound preparation time was 13.6 days when using PADM whereas non-PADM treatment required 22.4 days. 85 Overall hospitalisation decreased by 14 days on average. PADM was shown to promote granulation tissue growth, with maximum retention of penile and perineum function, morphology and protective features. 85
While aphallia is a condition typically addressed by either the De Castro technique or a scrotal flap phalloplasty,86,87 one case report has detailed usage of ADM in this procedure for an infant, with the goal of supplying additional support and girth to the phallus as well as increased vascularisation. 80 After harvesting scrotal skin flap for neophallus construction, the ADM was sutured to the pubic symphysis, then covered with a layer of tunica vaginalis. Twelve months postoperatively, the patient had no complications and good cosmetic outcome. 80 Aphallia in children, however, is a rare disease with limited published data, and further research is needed to assess efficacy of ADM in this context.
One study reported that 60.3% of patients experienced erectile discomfort and 12.8% had no obvious augmentation effects when treated with ADM. 82 Reported complications include severe penile oedema, ischemic shaft ulcers, hematomas and wound infections.82,83 Upon suturing the ADM to Buck’s fascia, micro-branches of the dorsal nerve of the penis may become covered and lead to less receptor threshold. 84 Additionally, a thick ADM may affect proprioception receptors in the deep tissue and on the skin surface, leading to abnormal temperature and pressure differences. 84
Gynaecology and gynaecological oncology
Historically, vaginoplasties were performed using peritoneal tissue, STSGs or allogenic epidermal sheets.88,89 However, ADM has recently been utilised to reduce postoperative pain, procedural complexity and preserve the vaginal mucosa histology. 90 In one study, 16 patients diagnosed with uterine cervix carcinoma underwent vaginal repair using ADM after radical hysterectomy and radiotherapy. 90 Two weeks postoperatively, normal epithelial tissue and vaginal mucosa histology were observed whereas histology previously revealed granulation and inflammatory cells.
Published reports suggest that vaginal length <7 cm is correlated to less sexual satisfaction with lower sexual function. 91 After vaginoplasty with ADM secondary to carcinoma resection of the cervix, vaginal length was improved to an average final length of 9.25 cm, with 75% of patients reporting improved sexual satisfaction. 90 By utilising the ADM in the cervical repair, the superior end of the vagina is preserved, thus retaining cells for future cervical screening tests. 90 Unlike biological tissue, which is at risk of defects and infections when exposed to radiation, a synthetic ADM mesh may be better suited for harsh environments and minimise inflammation and malformations in surrounding tissue.92–94 Of note, successful integration of ADM relies on implantation within highly vascularised tissue. 94
Recurrent gynaecological cancer is traditionally treated with pelvic exenteration using synthetic mesh, myocutaneous flaps from the abdomen or thigh, or pedicled greater omental flaps (PGOF) to secure the pelvic floor. 95 However, a recent case report described the use of PGOF, HADM, and autologous adipose-derived cells to improve pelvic cavity support and volume. 96 Success in this case may be attributed to accelerated angiogenesis and the favourable environment for adipose-derived stem cell incorporation provided by HADM. 97 Another patient with osteoradionecrosis and recurrent vulvar squamous cell carcinoma underwent exenteration, and pelvic floor reconstruction incorporated HADM with bilateral, thigh-based tissue flaps. The carcinogenic and bacterial-infected wounds resolved without complication. 98
Orthopaedic surgery
Foot and ankle
ADMs have been used to promote bony regrowth and periosteum replacement, ultimately leading to cell proliferation, neovascularisation and resolution of bone defects (Table 6).99,100 ADMs have gained popularity in foot and ankle procedures as they lack the disadvantages inherent in many human auto- or allografts, xenografts or synthetic grafts. 101
Clinical evidence for ADMs in orthopaedic surgery.

ADM, acellular dermal matrix; AOFAS, Association of Orthopaedic Foot and Ankle Society; ASES, American Shoulder and Elbow Surgeons; FFI-R, Foot Function Index-Revised; M-ADM, human dermis processed with Matracell®; MTP, metatarsophalangeal; PADM, porcine acellular dermal matrix; PAS, Periodic acid–Schiff; ROM, range of motion; RSAF, reverse sural adipofascial flap; STSG, split-thickness skin graft; VAS, Visual Analogue Scale.
Multiple case reports describe ADM augmentation of Achilles tendon repairs with no instances of tendon rerupture or complications.101,102 ADMs have been used in interpositional ankle arthroplasty, either as a way to resurface the talus 103 or as a spacer in the first metatarsophalangeal joint. 104 Both procedures were successful, with increased ROM, decreased pain, and no complications.103,104 ADMs have also been successfully utilised to facilitate ankle wound healing. 105 When combined with a reverse sural adipofascial flap (RSAF), ADMs led to 25% faster healing compared to RSAF alone. 34
Shoulder and upper extremity
In both primary and revision rotator cuff repairs, incorporation of ADMs has led to improvements in pain, ROM and muscle strength.106,107 These repairs remained intact at long-term follow-ups. 107 In irreparable rotator cuff tears, ADMs have been used to cover the exposed bone, leading to decreased pain and better functional scores. 108 ADM augmentation of distal biceps repair in a tendon-deficient model led to a stronger tendon than without ADM. 109
ADMs have been shown to improve interface strength and decrease re-tear rates when applied at the suture-tendon interface of rotator cuff repairs. 110 Though the procedure is technically challenging, surgeons have also utilised ADMs in superior capsular reconstructions, resulting in improved pain and shoulder function. 111
ADM use has been described in glenoid resurfacing with improved outcomes in most cases. 112 However, foreign body reactions have been reported and should be considered if there is significant postoperative pain. 112 ADMs have been interposed between the radius and ulna to prevent heterotopic ossification after a forearm injury, leading to improvements in ROM and no recurrence. 113 ADMs are also thought to be more resistant to infection than silicone and collagen-based alternatives. 113
Hand and wrist
ADMs have been used to reconstruct ligaments in arthritic hands. 114 Historical methods utilised donor tendon, but were associated with scarring, pain, tendon rupture, tendonitis and neuroma formation. 114 Xenografts addressed some of these disadvantages, but caused immunologic reactions in some patients. 114 In a cadaveric scapholunate reconstruction model, HADM provided tensile strength comparable to traditional techniques and may potentially decrease donor site morbidity in these repairs. 115 A study of 100 ligament reconstructions in patients with thumb carpometacarpal arthritis found that, when using ADM, there were no adverse effects, foreign body reactions or infections. 114
When used for Dupuytren’s disease, ADMs have been shown to decrease the rate of recurrence, presumably via ADM-mediated inhibition of myofibroblasts that might otherwise create contractures.116,117 ADMs have been used in proximal row carpectomies to prevent degradation of the radiocapitate space and have been effective in treating radiocarpal arthritis. 118 ADMs have demonstrated efficacy as an adjunct in treating neuropathic wrist pain. 119 In these cases, ADM was used to cushion the nerve as an alternative to the traditional flap coverage. 119
Hip and pelvis
ADMs have been used effectively to augment gluteus medius and minimus repairs. 120 This technique is thought to decrease re-tear rates by providing structural strength to the repair, better tendon-bone healing and increased tensile strength due to revascularisation of the graft. 120
Capsular defects have been filled using ADMs to create hip stability in hip reconstructions. 121 ADMs have shown some utility in addressing shortcomings of common hip abductor repair methods. 122 Traditional techniques are associated with unpredictable results with extended periods of rehabilitation. 122 However, patients receiving ADM treatments had significant improvement in Visual Analogue Scale pain and Harris Hip scores across groups. 122
Significant complications are common in pelvic reconstructions due to the complex anatomy, multi-level organ involvement and microbial environment associated with these procedures. 96 Historical attempts to improve outcomes such as synthetic meshes led to adhesions and infections, and myocutaneous flaps from the thigh were too invasive in many cases. 96 One case report described a less-invasive technique using HADM combined with a pedicled omental flap and autologous adipose derived cells that led to fewer adhesions. 96 Other cases have described the successful use of HADM in pelvic floor reconstruction after total exenteration or cylindrical abdominoperineal resection.96,98,123
Oral and maxillofacial surgery
The current gold standard for the treatment of gingival recession is the bilaminar technique using subepithelial connective tissue graft (SCTG); however, this technique has limitations, including the following: lack of available grafts; need for a second surgical site; pain after the surgery; proximity to the palatine neurovascular bundle; and suboptimal aesthetic outcomes. 124 ADMs have been shown to reduce the need for donor tissue and surgical time, and increase patient acceptance (Table 7). 125
Clinical evidence for ADM in oral and maxillofacial surgery.
AB, bone allograft; ADM, acellular dermal matrix; CAF, coronally advanced flap; EMD, enamel matrix derivative; FDADM, freeze-dried ADM; FGG, free gingival graft; HADM, human acellular dermal matrix; KMW, keratinised mucosa width; PADM, porcine acellular dermal matrix; PPG, periosteal pedicle graft; SDADM, solvent-dehydrated ADM.
ADMs have shown increased efficacy in treating Miller Class I, II and III gingival recessions in non-smokers124–127 and Miller Class I and II in smokers 128 compared to non-ADM controls. ADMs were also an effective adjunct when used in conjunction with a coronally advanced flap in Miller Class I and II recessions.129,130
Multiple formulations of ADMs have been used in gingival recession treatment, with both freeze-dried and solvent-dehydrated ADMs successfully achieving root coverage. 131 HADMs have produced superior aesthetic outcomes when compared to autogenous free gingival graft but were associated with delayed healing. 132 Of note, one study reported complete root coverage in only 42.86% of patients using PADM. 133
There is a growing body of research evaluating ADMs in other conditions, including gingival fenestrations, 134 persistent parotid fistulas, 135 ora-antral fistulas, 136 alveolar bone loss/grafting137,138 and dental implants.139–141 Generally, ADMs were used to limit donor tissue harvest, 134 promote soft tissue growth137,139 and improve aesthetic outcomes. 141
Craniofacial surgery
ADMs have been used in craniofacial surgery to treat soft-tissue defects secondary to congenital conditions, disease and surgical wounds.142–150 In aplasia cutis congenita (ACC), ADMs have shown utility both as an adjunct to grafting and as a conservative treatment for scalp coverage.142,143
BADM has been used as a spacer graft for upper eyelid retraction procedures secondary to thyroid eye disease. 145 In a study of 32 eyelids in 26 patients, average upper margin reflex distance was lowered from 7.7 mm to 3.3 mm with 69% of patients achieving perfect results. 145 ADMs have also been used to manage nasal lining deficiency in Le Fort 1 osteotomy, prevent Frey syndrome after parotid neoplasm surgery and as an implant for dorsal augmentation in rhinoplasty.146–148 In patients with cranial defects, ADM has been used to improve bone regeneration and closure of chronic wounds after skull defect reconstruction.149,150
Abdominal wall/hernia
Ventral hernias, though common, continue to present surgical challenges, and there is no consensus regarding optimal treatment (Table 8).151,152 Biological mesh composed of ADM has recently been used in efforts to address the shortcomings of synthetic materials in abdominal wall reconstructions.74,153,154 In 2010, the Ventral Hernia Working Group published a grading system with recommendations for use of either synthetic (Grade 1) or biological mesh (Grades 2–4), with grades designated by risk of postoperative complications.152,155
Clinical evidence for ADMs in AWR.
ADM, acellular dermal matrix; AWR, abdominal wall reconstruction; BADM, bovine acellular dermal matrix; FBADM, fetal bovine acellular dermal matrix; HADM, human acellular dermal matrix; PADM, porcine acellular dermal matrix.
Compared to synthetic mesh, ADM has been associated with decreased rates of infection, extrusion, erosion and adhesion formation. 154 In studies comparing different types of ADM, PADM and BADM appear to outperform HADM.153,154,156 While HADM may be equally effective in reducing infection, recurrence rates are higher than in PADM or BADM.74,153,154,156,157 The high elastin content of HADM is believed to contribute to relaxation over time and may be the cause of increased reports of laxity and/or bulging.154,156–158
PADM has been used effectively in giant and recurrent hernias, as well as in both elderly and paediatric patients and recurrent hernias.155,159,160 One study comparing PADM and BADM showed similar outcomes between the two formulations. 161
The literature assessing PADM and BADM is lacking in some surgical procedures such as bladder exstrophy repair, urethral reconstruction and treatments for premature ejaculation; however, HADM has shown utility in these procedures (Table 9).4,162,163
Clinical evidence for ADMs in urology.
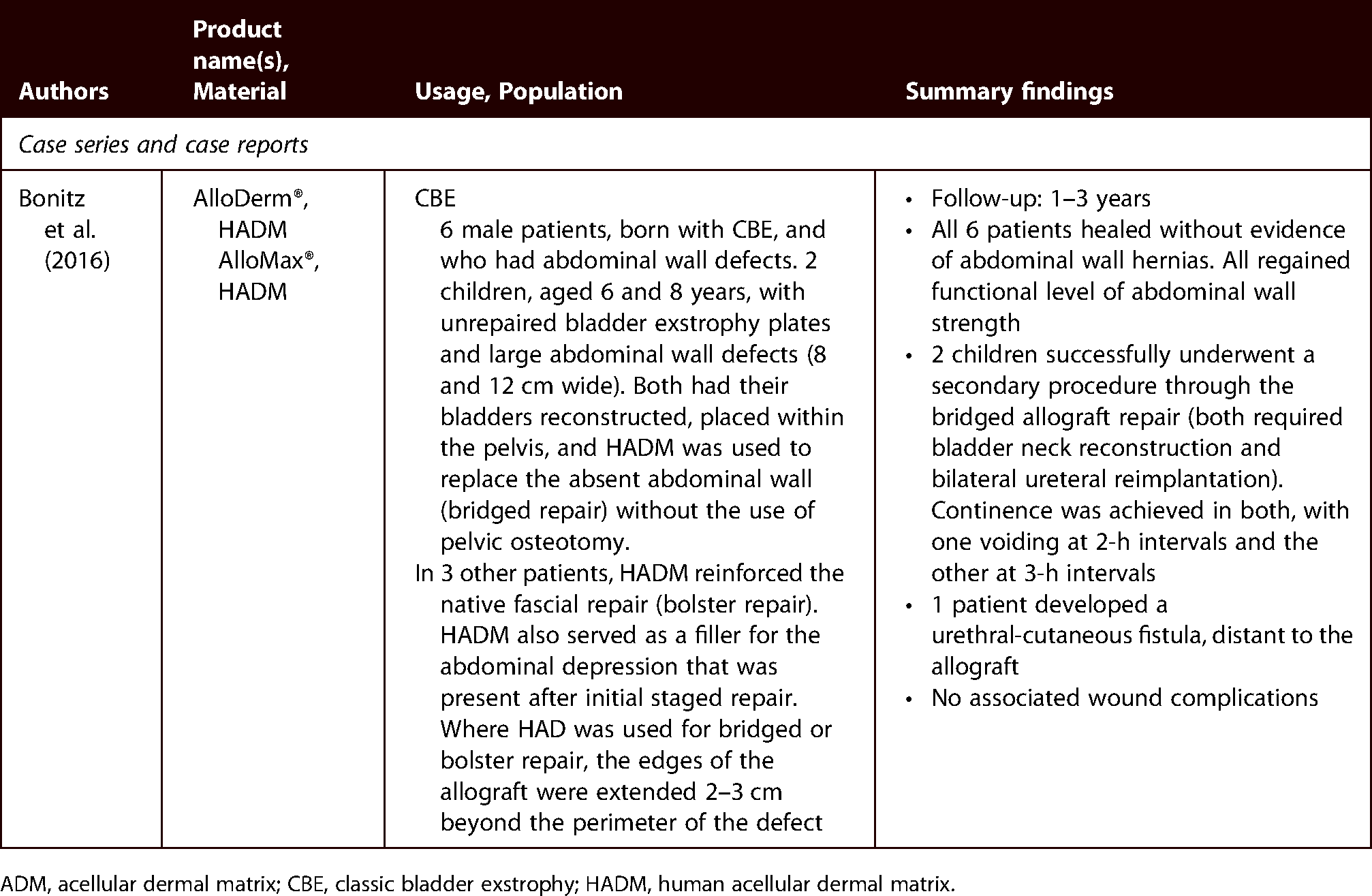
ADM, acellular dermal matrix; CBE, classic bladder exstrophy; HADM, human acellular dermal matrix.
Of note, one case report described a delayed type IV hypersensitivity reaction to PADM. 164 When infection is suspected after ADM placement, hypersensitivity should be considered as part of the diagnostic algorithm. 164
Otolaryngology/ear, nose and throat (ENT)
HADM and xenogeneic ADMs have been used in laryngotracheal and pharyngeal reconstruction as they are relatively thin and flexible compared to myocutaneous flaps.165–169 ADM grafts carry lower risk of fistula and stricture formation and avoid donor site complications associated with flap harvest. 165 Thin ADMs are more often used for partial superficial defects in the trachea, larynx or hypopharynx. Thicker sheet ADMs were typically used for complex pharyngeal fistula closure and partial pharyngoplasty for stage III–IV carcinomas. 165 Other successful uses of ADM in otorhinolaryngology include closure of hard palatal fistula and tympanoplasty.170,171
Discussion
The current literature indicates that there is not a single ADM that has proven superiority in every clinical context.70,153,154,156 In burn wounds, BADMs have produced the most favourable outcomes (compared to PADM and HADM). While Integra™ is the most popular option for coverage, MatriDerm® has seen increased utilisation as it can be applied in a single-stage procedure and provides improved neovascularisation and degradation. 19 Further studies are needed to compare PADM and BADM.
In breast reconstruction, multiple studies have been performed to directly compare ADMs of different tissue origins.12,73 There is no clear aggregate trend indicating that one tissue source consistently produces favourable outcomes.12,72,73 However, of the available HADMs, AlloDerm® may outperform other HADMs in breast reconstruction.71,75 In these procedures, increased implant size and/or thickness (≥1.2 mm) appears to negatively impact outcomes.53,60,69
In procedures such as abdominal wall reconstruction, structural components of ADM play a role in the stability of the repair. Aside from providing mechanical cues, properties that confer rigidity, such as lower elastin content, may influence the success of a repair.154,156–158
As previously mentioned, ADMs are frequently used to treat gingival recessions and provide improved cosmesis compared to traditional autograft techniques. HADM outcomes are generally superior to PADM, though the literature is lacking in studies with direct comparisons.132,133 Of note, standardised ADM graft size may skew outcomes as individual patients have highly variable gingival defects. 132
In orthopaedic procedures, ADMs have primarily been used in orthoplastic reconstructions (e.g. reverse sural flap) and in tendon repairs where limited vascularisation and/or adhesion is a concern. 120 Future applications of ADM in orthopaedic applications may incorporate more injectable formulations.
Many ADMs have been treated with different products, cells and signalling molecules.6,7 For example, ADMs pretreated with bFGF had better recruitment of mesenchymal stem cells, 71 proliferation and differentiation compared with a matrix pretreated with BMP-2 (though both were better than controls).6,172 Further studies are needed to assess the clinical utility of various treated ADMs.
ADMs have been produced from a variety of sources including human, porcine and bovine tissue and can be further classified by tissue source (dermis, intestinal submucosa, urinary bladder, pericardium, etc.).173,174 The variable efficacy between different allogenic or xenogenic ADMs may be attributed to advantages and/or disadvantage of each in providing barrier function, vascular ingrowth, innervation potential, growth factors and mechanical cues to induce site-appropriate healing. 175 In addition to the origins of each ADM, products vary by type and level of processing and/or sterilisation. 176 Some studies have suggested that aseptic processing is more beneficial than sterilisation, but others have found them to be equivalent, and there is currently no consensus on optimal processing.177,178
In addition to efficacy considerations, practical and ethical constraints must be considered in discussions of ADM products. Xenogenic ADMs are more readily available (compared to HADMs). However, patients belonging to certain ethnic and/or religious groups may hold beliefs that preclude the use of products with certain tissue origins. 179 Patients’ belief systems often require a nuanced understanding of religious and cultural norms. 179 For example, while Jewish and Islamic dietary restrictions may not translate to tissue implantation, Buddhists and Seventh-day Adventists often practice veganism, which could lead them to refuse xenogenic tissue products. 180 Furthermore, some Hindus and Sikhs are opposed to all allogenic and xenogenic products, but other Hindus allow the use of donated allogenic tissues.179,180
Given that ADMs represent a relatively new addition to the reconstructive ladder, datum is limited regarding the efficacy of different commercially available ADMs in specific clinical contexts. This review does not include quantitative meta-analyses and is limited by the quality and/or amount of clinical data available for some injury patterns. Additional studies are needed for direct comparison of various ADMs. While formulations and clinical uses of ADM continue to evolve, this review provides a broad overview to better define our current understanding of its clinical utility.
Conclusion
ADMs have been used in a variety of clinical contexts, utilising the properties of the ECM to aid in organised native tissue regeneration. There is clinical evidence to support ADM usage in various subspecialties and procedures, including orthopaedic surgery, breast reconstruction, burn, wound care, andrology, oral and maxillofacial surgery, craniofacial surgery, abdominal wall/hernia repair and otolaryngology. Early reports on ADMs are promising, and further research is needed to determine their place in current reconstructive algorithms.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: SBH1038313. Though they are not directly related to this case report, the authors would like to disclose the following support for Brendan MacKay: Paid teaching for TriMed. Paid teaching and consulting, as well as research support from AxoGen. Paid consulting for Baxter/Synovis and GLG. The remaining authors have nothing to disclose.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
How to cite this article
Petrie K, Cox CT, Becker BC and MacKay BJ. Clinical applications of acellular dermal matrices: A review. Scars, Burns & Healing, Volume 7, 2021. DOI: 10.1177/ 20595131211038313.